
Abstract
BACKGROUND AND PURPOSE: Vertebrobasilar dolichoectasia aneurysm is a rare type of cerebrovascular disorder with a poor natural history, and endovascular treatment is widely accepted. Whether a high-profile braided stent (flow diverter) could promote occlusion of vertebrobasilar dolichoectasia aneurysm without increasing the complications rather than a low-profile braided stent remains uncertain. The aim of the study was to present a single-center experience of the safety and efficacy of a low-profile braided stent versus a flow diverter in treating patients with vertebrobasilar dolichoectasia aneurysms.
MATERIALS AND METHODS: The retrospective review was conducted on a total of 432 consecutive patients diagnosed with posterior circulation aneurysms who underwent endovascular treatment in our center from August 2013 to December 2021. Among these patients, 47 individuals with vertebrobasilar dolichoectasia aneurysms who were treated with low-profile braided stents or flow diverters were included. Vertebrobasilar dolichoectasia aneurysms involving only the vertebral artery were excluded. Patients were divided into 2 groups: the low-profile braided stent group and the flow diverter group based on the device used. Safety and efficacy outcomes were subsequently analyzed.
RESULTS: There were 25 total patients enrolled in low-profile braided stent group and 22 patients in flow diverter group. The safety of low-profile braided stents and flow diverters in the treatment of vertebrobasilar dolichoectasia aneurysms was evaluated by clinical outcome, a new neurologic deficit due to procedural complications, and neurologic death. The rates of good clinical outcome were similar between the 2 groups (low-profile braided stent, 56%, versus flow diverter, 59.1%; P = .831), and the rates of neurologic death were also similar (low-profile braided stent, 12%, versus flow diverter, 9.1%; P = .747). Higher rates of new neurologic deficits due to procedural complications were observed in the flow diverter group, but the difference was not significant (low-profile braided stent, 24%, versus flow diverter, 40.9%; P = .215). The efficacy was evaluated by angiographic occlusion of vertebrobasilar dolichoectasia aneurysms and progression of mass effect resulting from these aneurysms. Significantly higher rates of complete occlusion of vertebrobasilar dolichoectasia aneurysms were shown in the flow diverter group (41.2%; P = .028) than in the low-profile braided stent group (10%).
CONCLUSIONS: Both low-profile braided stents and flow diverters have similar high risks in reconstructive techniques in the treatment of vertebrobasilar dolichoectasia aneurysms, while a flow diverter is more effective in promoting complete occlusion of vertebrobasilar dolichoectasia aneurysm than a low-profile braided stent. A flow diverter may be a better alternative for carefully selected patients with vertebrobasilar dolichoectasia aneurysms.
ABBREVIATIONS:
- FD
- flow diverter
- LPBS
- low-profile braided stent
- VBDA
- vertebrobasilar dolichoectasia aneurysm
Vertebrobasilar dolichoectasia aneurysm (VBDA) is a rare type of cerebrovascular disorder resulting in ectasia, elongation, and tortuosity of the vertebrobasilar artery. Flemming et al1 assumed that the incidence was <0.05%, while Ince and Alpaslan2 revealed that a VBDA was detected in approximately 2.06% of the first-ever stroke population. Patients with VBDAs commonly present with ischemic stroke, intracranial hemorrhage, and compression of the brainstem and/or cranial nerves, which could lead to high rates of morbidity and mortality.3⇓⇓⇓-7 The natural history of VBDA is poor, and the cumulative proportion of survivors free of adverse health events was 54.1% at 5 years, 39.5% at 10 years, and 23.5% at 15 years.8 Such a poor natural history indicated that professional intervention was necessary. However, treatment of VBDAs was also challenging.
Surgical treatment of VBDAs is rarely reported, and even the most experienced team reported an extremely high mortality in surgical outcome.9,10 Endovascular treatment is more widely accepted and relatively simple in comparison. The low-profile braided stent (LPBS) has proved to be effective and relatively safe in treating VBDA during short-term follow-up, but it showed limited effectiveness in improving long-term prognosis and clinical outcome of patients with compressive symptoms.11⇓-13 The flow diverter (FD) has revolutionized the treatment of intracranial aneurysms and showed great potential in treating such nonsaccular intracranial aneurysms. However, complication rates using a FD in treating posterior circulation aneurysms are much higher than those for the anterior circulation.14 Additionally, patients with basilar artery aneurysms have even significantly higher rates of mortality than those with vertebral artery aneurysms due to a high profile and existence of pontine perforators.15 Whether a high-profile braided stent (FD) could promote occlusion of VBDAs without increasing the complications more than LPBSs remains questionable. Therefore, we aimed to present our single-center experience based on 47 patients with VBDAs treated with LPBSs and FDs.
MATERIALS AND METHODS
Study Design
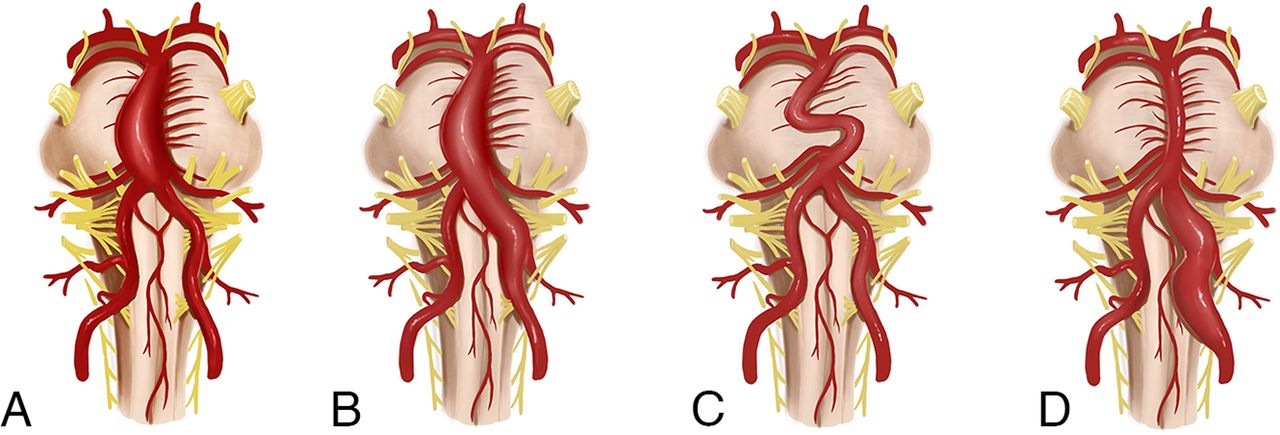
This was a single-center retrospective study; it was approved by the ethics committee and local institutional review board of Xuanwu Hospital, Capital Medical University, Beijing, China (Nos. NO.2017024 and No 2017082). The requirement for written informed consent was waived because of the retrospective nature. The retrospective review was conducted on a total of 432 consecutive patients diagnosed with posterior circulation aneurysms who underwent endovascular treatment in our center from August 2013 to December 2021. The diagnosis of all enrolled patients with VBDAs was radiologically confirmed by DSA after admission. The inclusion criteria for the subjects were as follows: 1) untreated and unruptured VBDAs meeting the diagnostic criteria defined as uniform aneurysmal dilation of an artery of >1.5 times normal involving the basilar artery with a superimposed dilation of a portion of the basilar trunk;1 and 2) use of a reconstructive technique with an LPBS or FD for treatment, with or without adjunctive coils. The exclusion criteria for the subjects were as follows: 1) a VBDA presenting with only elongation and/or tortuosity but without ectasia (Fig 1C); 2) a VBDA involving only the vertebral artery (Fig 1D). A VBDA without significant dilation was not included due to its relatively benign natural history. A VBDA involving only the vertebral artery was also excluded because the difficulty and risk of the treatment was largely different whether or not the basilar trunk was involved due to the existence of pontine perforators. Finally, 47 patients with VBDAs were included. All enrolled patients were classified into 2 groups: the LPBS group and the FD group according to the device used.

Artistic illustration of the inclusion criteria: VBDA involving the basilar artery (A), and VBDA involving both basilar and vertebral arteries (B) with superimposed dilation of a portion of the arterial segment. Artistic illustration of the exclusion criteria: A VBDA presenting with only elongation and/or tortuosity but without ectasia (C), and a VBDA only involving only the vertebral artery (D). The pictures are drawn by courtesy of Dr Jian Ren.
Procedures
All procedures were performed with the patient under general anesthesia, with a femoral approach used in all patients. A 5F or 6F Navien intermediate catheter (Medtronic) was placed in the vertebral artery within a 6F Envoy DA guiding catheter (Codman Neuro), a 6F or 8F Envoy guiding catheter, or a 6F Neuron MAX long sheath (Penumbra). Marksman (Medtronic), Phenom 27 (Medtronic), or a Fast-track (MicroPort) microcatheter was introduced over a 0.014-inch Synchro guidewire (Stryker) into the distal posterior cerebral artery. Two types of LPBS, LVIS stent (MicroVention) and LEO stent (Balt Extrusion), and 2 types of FDs, the Pipeline Embolization Device (Medtronic) and the Tubridge Embolization Device (MicroPort), were used for treatment.
Anticoagulation and Antiplatelet Management
Before endovascular treatment, routine daily doses of dual antiplatelet therapy, including at least 100 mg of aspirin combined with 75 mg of clopidogrel, were given for at least 3 days. However, platelet function testing was not conducted systematically because of the retrospective nature of the study. Intraoperative unfractionated heparin was given according to the patients’ weight at a dose of 0.67 mg/kg once the endovascular treatment approach was established, and an additional dose was given depending on the length of the procedure. Additional postoperative tirofiban (0.1 μg/kg/min) was administered at the discretion of the operators. All patients would continue 100 mg of aspirin daily for at least 12 months and 75 mg of clopidogrel for at least 6 months.
Follow-Up and Outcome Measurements
Clinical follow-up was conducted at least 6 months after endovascular treatment, and the mRS was used to evaluate the clinical outcome. An mRS score of ≤2 was considered a favorable clinical outcome, and an mRS score of ≥3 was considered an unfavorable clinical outcome. Changes in the mRS score were used to evaluate changes in clinical outcomes from admission to the latest clinical follow-up. A radiologic examination was also conducted at least 6 months postoperatively. Angiographic occlusion was evaluated by DSA,16 and the result was categorized as complete (100% volume of dilation was occluded), near-complete (>90% volume of dilation was occluded), or incomplete (<90% volume of dilation was occluded). Progression of a mass effect resulting from a VBDA was evaluated by MR imaging. Measurements of the maximum transverse diameter of the vessel wall were performed at the same level on preoperative and follow-up MR imaging. Progression of mass effect was defined as enlargement of the maximum transverse diameter of the vessel wall of ≥5 mm, or the result would be considered as no progression.
All complications thought to be procedural were reported. Complications were classified as intracranial hemorrhagic and ischemic. Procedural ischemic complications were defined as any ischemic events with definite clinical expression that contributed to an increase of ≥1 point on the NIHSS and radiographically confirmed fresh cerebral infarction around posterior circulation territories. Procedural hemorrhagic complications were defined as any intracranial bleeding events, radiographically confirmed intracranial or subarachnoid hemorrhage on CT.
All the above evaluations were conducted independently by 2 neurointerventionalists with >5 years of experience and confirmed by a neurointerventionalist with >15 years of experience.
Statistical Analysis
Descriptive statistics were used. Categoric variables are presented as numbers and percentages. Continuous variables are presented as mean and range. Differences in baseline characteristics, clinical outcomes, and radiologic outcomes between groups were analyzed using t tests and χ2 tests. SAS software, Version 9.4 (SAS Institute) was used for statistical analyses.
RESULTS
Baseline Characteristics
The study included a total of 47 consecutive patients with VBDAs according to the inclusion and exclusion criteria above. The mean age of the patients enrolled was 59 years (range, 43–79 years). Thirty-eight (80.9%) patients were men, hypertension was observed in 42 (89.4%) patients, and 41 (87.2%) patients had an mRS score of ≤2 at admission. The mean length of the VBDA was 35.8 mm (range, 14.4–70.1 mm), and the mean diameter of the VBDA was 15.3 mm (range, 7.2–26 mm). All patients were classified into 2 groups according to the device used, with 25 patients in the LPBS group and 22 patients in the FD group. There were no statistically significant differences in baseline patient and VBDA imaging characteristics between groups. The detailed baseline patient and VBDA imaging characteristics are shown in Table 1 and the Online Supplemental Data.
Baseline patient and VBDA imaging characteristics
Safety Results
The safety of the LPBS and FD in the treatment of VBDA was evaluated by clinical outcome, new neurologic deficits due to procedural complications, and neurologic death. Clinical follow-up data were available for all 47 patients. The median duration of clinical follow-up was 28 months for the LPBS group and 23 months for the FD group. The rates of good clinical outcome were similar between 2 groups (LPBS, 56%, versus FD, 59.1%; P = .831), and there was also no significant difference in changes in symptoms. Higher rates of new neurologic deficits due to procedural complications were observed in the FD group, while ischemic complications accounted for the most deficits, but the difference was not significant (LPBS, 24%, versus FD, 40.9%; P = .215). Additionally, some patients presented with excellent recovery after treatment of symptoms, and the rates of mild-to-severe disability due to procedural complications were similar. Similar rates of neurologic death were also shown between 2 groups (LPBS, 12%, versus FD, 9.1%; P = .747). Two patients died of brainstem function failure resulting from brainstem infarction, 2 patients died of intracerebral hemorrhage resulting from thrombolysis from brainstem infarction, and 1 died directly from intracranial hemorrhage. Another 2 patients died of uncorrelated heart failure and pneumonia. The detailed safety results are shown in Table 2 and the Online Supplemental Data.
Safety and efficacy results
Efficacy Results
The efficacy of LPBS and FD in the treatment of VBDA was evaluated by angiographic occlusion of VBDA and progression of the mass effect resulting from VBDA. Radiologic follow-up data were available for 37 (78.7%) patients. Five deceased patients and 5 surviving patients were lost to radiologic imaging follow-up due to poor status except 1 patient. The median duration of radiologic follow-up was 24 months for the LPBS group and 19 months for the FD group. Significantly higher rates of complete occlusion of VBDAs were shown in the FD group than in the LPBS group (LPBS, 10%, versus FD, 41.2%; P = .028). Lower rates of incomplete occlusion of VBDAs were shown in the FD group than in the LPBS group, but the difference was not significant (LPBS, 30%, versus FD, 17.1%; P = .383). Although there was no significant difference, the FD group showed advancement in slowing down progression of mass effect resulting from the VBDA. The detailed radiologic follow-up outcomes are shown in Table 2 and the Online Supplemental Data.
Illustrated Cases
Case 1.
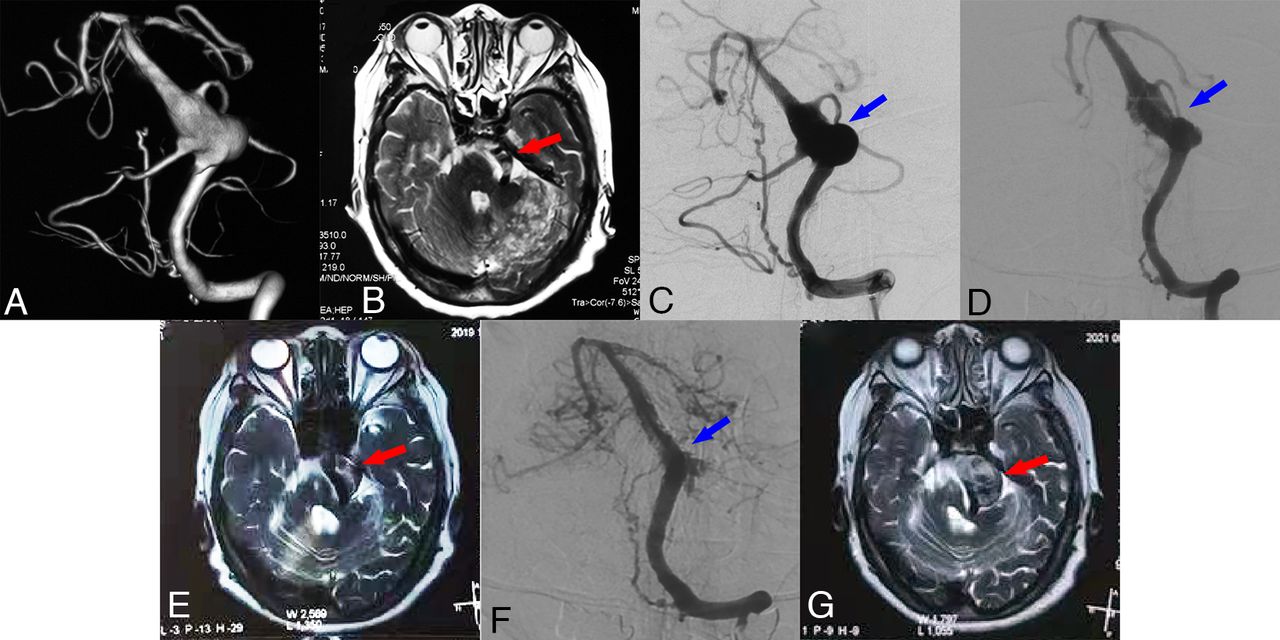
The patient (case No. 10) had choking, dysphagia, and weakness of the lower extremities with an mRS score of 2 and was admitted to our center 5 years ago. Further DSA showed vertebrobasilar dolichoectasia (VBD), while T2-weighted MR imaging indicated mild brainstem compression (Fig 2A, -B). Considering that the patient had compressive symptoms and obvious dilation of the basal-inferior segment, 2 LEO stents were implanted (Fig 2C). Two years later, the patient returned with choking recurrence, dysphagia, and weakness of the lower extremities accompanied by tinnitus. Follow-up DSA indicated partial occlusion of the VBD lesion, while T2-weighted MR imaging revealed progressive brainstem compression (Fig 2D, -E). Another LEO stent implantation was performed to obtain better direction of blood flow. Although the 5-year follow-up DSA showed that the VBD lesion was relatively stable, remarkable progression of brainstem compression was observed on the 5-year follow-up MR imaging (Fig 2F, -G). Meanwhile, the patient had aggravation of gait instability, choking, and dysphagia. Further FD implantation was planned for the patient, but unfortunately, the patient refused. The patient was unable to take care of herself at the latest follow-up with an mRS of 4. The long-term effectiveness of LPBSs in preventing recanalization and increased mass effect of the VBD remains questionable.

Preoperative DSA (A) and MR imaging (B) showing a VBDA and mild brainstem compression (red arrow). Angiography (C) after 2 LEO stents were implanted (blue arrow). Two-year follow-up DSA (D) indicating partial occlusion of the VBDA lesion (blue arrow), with MR imaging (E) revealing progressive brainstem compression (red arrow). Five-year follow-up DSA (F) showing further angiographic occlusion of the VBDA lesion (blue arrow), with MR imaging (G) revealing obvious progression of brainstem compression (red arrow).
Case 2.
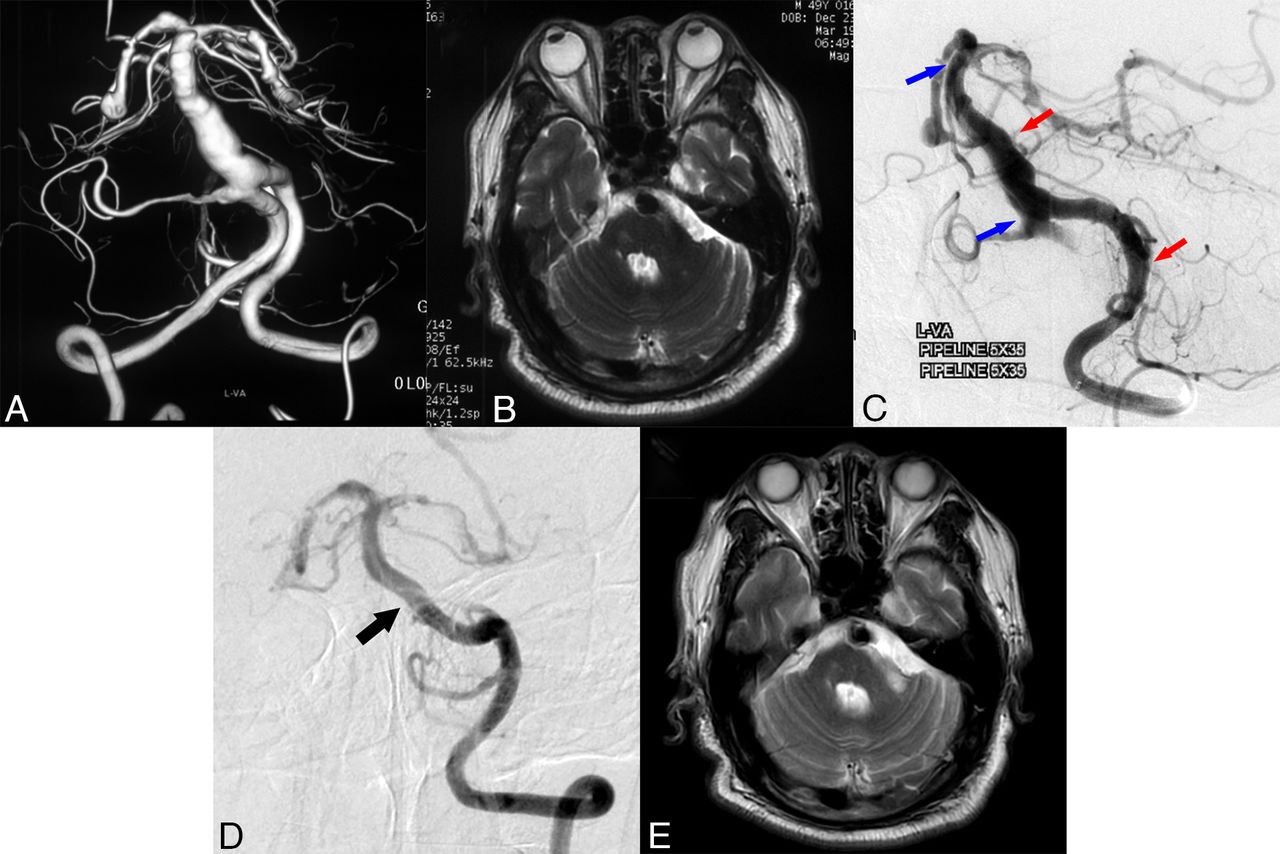
The patient (case No. 40) had dizziness and weakness of the lower extremities with an mRS score of 2 at admission, and planned DSA showed VBD, while MR imaging indicated no obvious brainstem compression or obvious dilation of the lesion (Fig 3A, -B). Endovascular treatment with 2 Pipeline Embolization Devices was performed (Fig 3C), and no periprocedural complications occurred. Nine-month follow-up DSA showed good healing of the dilation, with no obvious progression of compression observed on MR imaging (Fig 3D, -E). The patient also considered the symptoms to have gradually improved after endovascular treatment with FDs at the latest 2-year follow-up visit.

Preoperative DSA (A) showing a VBDA, with MR imaging (B) indicating no obvious brainstem compression. Angiography (C) after endovascular treatment with 2 Pipeline Embolization Devices was conducted. The blue arrows point to the proximal and distal edges of the first 5 × 35 cm Pipeline Embolization Device. The red arrows point to the proximal and distal edges of the second 5 × 35 cm Pipeline Embolization Device. Nine-month follow-up DSA (D) shows good healing of the dilation (black arrow) with no obvious progression of compression on MR imaging (E).
DISCUSSION
Both LPBSs and FDs have high risks in the reconstructive technique in the treatment of VBDAs, but whether a VBDA should be treated and the indications for the VBDA still remain confusing. The natural history of VBDA is poor, and the cumulative proportion of survivors free of adverse health events was 54.1% at 5 years, 39.5% at 10 years, and 23.5% at 15 years.8 However, except for radiologic progression of the VBDA, which has been suggested to be associated with poor clinical outcome, no other defined risk factors have been reported.17,18 Specific radiographic features that indicate VBDA tend to change from benign, even asymptomatic, to malignant and require treatment remain unanswerable. According to a recent meta-analysis, patients with VBDAs could not benefit significantly from endovascular treatment in comparison with the natural history. Therefore, the indications of VBDAs are of great importance.19 Patients with VBDAs who underwent endovascular treatment in our cohort usually presented with prominent clinical symptoms, obvious dilation with high rupture risk, or enlargement during follow-up. We prefer conservative treatment and regular follow-up for patients with VBDA who remain asymptomatic or VBDAs without dilation due to their relatively benign natural history.1 However, all treatment decision-making processes still depend on the discretion of operator instead of uniform consensus.
Previous reports had concluded that the high profile of the FD either mechanically blocks the orifice of the side branch or narrows it to an insufficient size, accounting for the occurrence of perforator infarction.20 Perforator infarction was associated with a significantly higher risk of posterior circulation aneurysms, especially the aneurysm around brainstem, due to a lack of collaterals and delicate perfusion.21 However, safety outcomes between the LPBS and FD groups were similar according to the result, on the basis of our experience. Although higher rates of new neurologic deficits due to procedural complications were observed in the FD group, while rates of ischemic complications in the FD group were 2 times higher than those of the LPBS group, the difference was not significant. Additionally, the rates of mild-to-severe disability due to procedural complications and clinical outcome were similar between groups.
The result was also consistent with a recent systematic review and meta-analysis, which showed no significant difference in favorable clinical outcomes between stent-assisted coiling and FD placement in the treatment of posterior circulation nonsaccular aneurysms.22 Early reports of VBDA treatment with an FD showed a very high complication rate of >50%,23 which has extremely restricted the application in the early stage. The telescope technique with multiple FDs may account for the poor results, and the technique was strictly limited in our cohort unless the dilated segment of the VBDA was too long, so the safety result was relatively acceptable. In addition, postoperative dual antiplatelet therapy with oral anticoagulation was reported to have a significantly better clinical outcome than dual antiplatelet therapy for patients with VBDA treated with an FD;24 similar regimens were also recommended for further treatment.
According to a recent systematic review and meta-analysis, no significant difference was shown in rates of complete/near-complete occlusion between stent-assisted coiling and FD placement in the treatment of posterior circulation nonsaccular aneurysms.22 This study had similar results in rates of complete/near-complete occlusion, but significantly higher rates of complete occlusion of VBDAs were shown in FD group than in the LPBS group. A large case series reported 28 subjects similar to VBDA in our cohort; the result revealed that 42.8% of patients had good angiographic results, which was almost consistent with our results.25 A multicenter study reported a total of 131 posterior circulation aneurysms treated with FDs, and the complete occlusion rates of fusiform aneurysms similar to VBDAs in our cohort was 59.7%, which was higher than our results.16 The VBDAs in our cohort were larger in diameter, while VBDAs only involving the vertebral artery being excluded may account for such results. In a study of 19 consecutive patients with VBDAs treated with LPBSs, the results showed that 84.2% of patients had good reconstruction of the VBDA during radiographic follow-up, a percentage that was also higher than our results.11 A significant proportion with adjunctive coils may account for such results. However, a similar strategy with LPBS and adjunctive coils was attempted in our cohort at an early stage, but rates of procedural complications were so high that adjunctive coils have been used with great caution since then.
Brainstem compression resulting from VBDAs was also a great therapeutic challenge. Although no significant difference was shown, the LPBS proved to be less effective in preventing progression of mass effect. As shown in illustrated case 1, despite favorable angiographic occlusion of the VBD lesion on DSA, mass effect still progressed and resulted in a poor prognosis. Another study reached a similar conclusion that the effects of LPBS were limited for patients with VBDAs presenting with compressive symptoms.12 The result reported by another team suggested that parent artery occlusion and flow diversion were better alternatives for VBDAs with brainstem compression, also partly consistent with our results.26 Last, different from other intracranial aneurysms, importance should be given to evaluating not only angiographic occlusion but also the progression of mass effect of the VBDA in follow-up because it was often ignored but could result in poor prognosis.
LIMITATIONS
This is a single-center retrospective study, but the sample size is large compared with similar studies. The VBDA is a rare type of cerebrovascular disorder, so the result is still acceptable. Results based on comparison between contemporaneous clinical and radiologic follow-up would be more persuasive, but such comparison is difficult to conduct because of the retrospective nature. Additionally, platelet function testing was also limited because of the retrospective nature. Only a subset of patients underwent platelet function testing, and the adjustment of antiplatelet regimens based on the results was also empirical.
CONCLUSIONS
There is no significant difference in the safety results between the LPBS and FD groups, but both strategies carry high risks. An FD is more effective in promoting complete occlusion of VBDAs than LPBSs. An FD may be a better alternative for carefully selected patients with VBDAs. However, advanced-level studies such as randomized controlled trials are still necessary and desired.
Footnotes
This study was supported by the Beijing Scientific and Technologic Project x, Z201100005520021, National Key Research Development Program x, 2016YFC1300800.
Chuan He and Hongqi Zhang contributed equally to this article.
We appreciate Jian Ren for drawing the artistic illustration.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received September 6, 2023.
- Accepted after revision November 2, 2023.
- © 2024 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}