
Abstract
BACKGROUND AND PURPOSE: Endovascular treatment has been increasingly used for anterior cranial fossa dural AVFs. Evidence on the safety and efficacy of different endovascular treatment strategies is limited. We report clinical and angiographic outcomes of patients with anterior cranial fossa dural AVFs who underwent treatment using transarterial embolization with n-BCA as a first-line approach.
MATERIALS AND METHODS: Consecutive patients undergoing treatment for anterior cranial fossa dural AVFs at the Amsterdam University Medical Centers between 2010 and 2023 were retrospectively included. Transarterial embolization was used as a first-line approach, while transvenous treatment and surgery were used in cases of unsuccessful transarterial embolization. Treatment was evaluated on the basis of the angiographic cure rate, procedural complications, and clinical outcome.
RESULTS: Fourteen patients were included with 15 anterior cranial fossa dural AVFs. All patients underwent primary endovascular treatment (12 transarterial, 1 transvenous, and 1 combined). Complete occlusion using only transarterial embolization was reached in 69% of patients (9/13), while the overall complete occlusion by endovascular treatment was reached in 79% of patients (11/14). Navigation and embolization were performed through the ophthalmic artery in 13 patients, with no procedural complications. Visual acuity was preserved in all patients. Three patients underwent an operation after failed endovascular treatment. All patients had complete anterior cranial fossa dural AVF occlusion at follow-up.
CONCLUSIONS: Treatment of anterior cranial fossa dural AVFs using transarterial embolization with n-BCA as a first-line approach is a safe and feasible first-line treatment strategy. No visual complications due to embolization through the ophthalmic artery occurred in this study.
ABBREVIATIONS:
- ACF
- anterior cranial fossa
- dAVF
- dural AVF
Anterior cranial fossa (ACF) dural AVFs (dAVFs) are a rare and relatively aggressive subtype of intracranial dural dAVF. Because of their drainage through cortical veins and the associated risk of hemorrhage, treatment is recommended in nearly all cases.1 The most common primary arterial feeders of ACF-dAVFs are formed by ethmoidal branches from the ophthalmic artery, with possible secondary contribution through collateral branches from the internal maxillary and middle meningeal arteries. Following advances in endovascular microcatheters and embolic agents, endovascular treatment of ACF-dAVFs has become the primary treatment technique in the past decade.2 However, no consensus exists on the optimal endovascular approach, either transarterial or transvenous, or if microsurgical disconnection is preferred over these techniques.3⇓⇓-6
Transarterial embolization is most commonly performed through the ophthalmic artery. A common concern with this approach is occlusion of the central retinal artery due to excessive reflux of embolic agent.3 Thus, some authors have proposed transvenous embolization as a preferred first-line approach.4,7 However, a venous approach carries the risk of venous perforation, and catheter positioning can be arduous in case of a tortuous venous anatomy.3,4,7
A recent study evaluated the use of transarterial embolization of ACF-dAVFs as a first-line approach, though primary transarterial embolization was only performed in 54% of patients (19/34), with central retinal artery occlusion occurring in 1 patient after embolization using Onyx (Medtronic).3 Ethylene-vinyl alcohol copolymers dissolved in dimethyl sulfoxide, such as Onyx or Squid (Balt), have been increasingly used in recent years for dAVF embolization, because they allow long injection times and controlled embolization. However, in contrast to n-BCA, copolymers require reflux for distal progression of the liquid agent, which is unwanted in embolization through the ophthalmic artery due to the proximity of the central retinal artery. The aim of this study was to report on outcomes of patients who underwent treatment of ACF-dAVFs using transarterial embolization through the ophthalmic artery with n-BCA as the first-line approach.
MATERIALS AND METHODS
Study Design
We retrospectively retrieved consecutive patients with ACF-dAVFs who were treated at Amsterdam University Medical Centers between January 2010 and April 2023. Of 14 eligible patients, 13 were previously included in a large cohort investigating the association between dAVFs and cerebral venous thrombosis, though without a description of the current subgroup and specific outcome measures.8 For this observational study, the ethics committee of the Amsterdam University Medical Centers waived the necessity for formal approval. In accordance with the General Data Protection Regulation, all eligible patients received an information letter about the study, with the option of refusing the use of their pseudonymized data. The current study was performed in accordance with Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.9
Treatment and Follow-Up
All referred patients were discussed in our neurovascular multidisciplinary team meeting to determine the indication for endovascular or surgical treatment. When possible, a first-line endovascular approach was preferred due to a less invasive nature than surgery. A primary transarterial approach was used, except in cases with unfavorable arterial anatomy or unfavorable (high) flow conditions. Depending on the angiographic anatomy, a primary route was chosen through the ophthalmic artery, ethmoidal branches, or middle meningeal artery. As a first choice, catheterization of the ophthalmic artery was attempted in all cases, regardless of the caliber or angle of origin. Flow-directed microcatheters (Magic 1.2F or 1.5F; Balt) in combination with microguidewires were used for selective microcatheterization. The size of the microcatheter was chosen depending on the caliber of the (distal) feeding branch from the ophthalmic artery. This choice allowed very distal catheterization with the goal of obtaining, as much as possible, a wedged microcatheter position. No vasodilators were used. A mixture of n-BCA (Histoacryl; B. Braun) and ethiodized oil (Lipiodol; Guerbet) was used for embolization with a ratio ranging from 1:1.5 to 1:4, depending on the estimated distance, flow speed, and size of the catheterized vessel. A wedged position of the microcatheter was preferred to allow maximum forward progression of n-BCA. Embolization through the ophthalmic artery was only performed if a safe position could be reached far enough distal to the origin of the central retinal artery. Injection with n-BCA was stopped after successful occlusion of the venous outlet or in case of progressive reflux nearing the origin of the central retinal artery. In cases of partial occlusion or when no embolization could be attempted, a transvenous approach could be considered, depending on the estimated risk of venous perforation. In cases of unsuccessful endovascular treatment, patients were referred for surgical disconnection. All endovascular procedures were performed by neurointerventional radiologists with extensive experience in endovascular procedures. Operations were performed by vascular neurosurgeons with extensive experience in dAVF surgery. Frontal or frontotemporal approaches were used with subsequent selective surgical disconnection.
Data Collection
Patient data on demographics, medical history, symptoms, and clinical outcome were retrieved from our electronic patient file system. Clinical outcome was defined on the basis of the presenting symptoms of the ACF-dAVF and classified as asymptomatic, improvement of symptoms, worsening of symptoms, or death. Visual function was subjectively assessed after treatment, while advanced assessment was performed in cases of suspected visual symptoms. Overall functional outcome at the last follow-up visit was retrospectively assessed using the mRS. An mRS ≥3 was defined as a poor (unfavorable) outcome.10 Follow-up imaging studies were reviewed for each patient.
The angiographic anatomy of each lesion was detailed by describing the arterial feeders, venous drainage pattern, and the presence of venous ectasia. Each lesion was classified according to the Cognard classification.11 Angiographic outcomes after embolization were complete or partial occlusion; the latter was defined as residual flow through the fistulous point and/or early venous filling of the draining vein of the dAVF.
Statistical Analysis
All analyses were performed using SPSS Statistics 28.0 (IBM). Continuous variables were described using mean (SD) or median with interquartile range, depending on their distribution.
RESULTS
Patient Characteristics
Fourteen patients were included in the study (Online Supplemental Data). The mean age was 59 (SD, 11) years with a range of 34–79 years. Sixty-four percent of patients were men (9/14). Medical history showed evidence of hypertension (n = 1), a previous cerebrovascular accident (n = 4), and previous cranial surgery (n = 2). Ten patients (71%) were past smokers, though none were active smokers. No patients had known previous head trauma. ACF-dAVF diagnosis was made by CT in 3 patients, MR imaging in 5 patients, and angiography in the remaining 6 patients. Twelve patients (86%) were symptomatic. Three patients presented with hemorrhage, namely SAH (n = 1) and frontal intraparenchymal hemorrhage (n = 2), the latter in 1 case combined with a subdural hematoma. Two patients were asymptomatic; in both, the ACF-dAVF was discovered incidentally.
Angiographic Anatomy
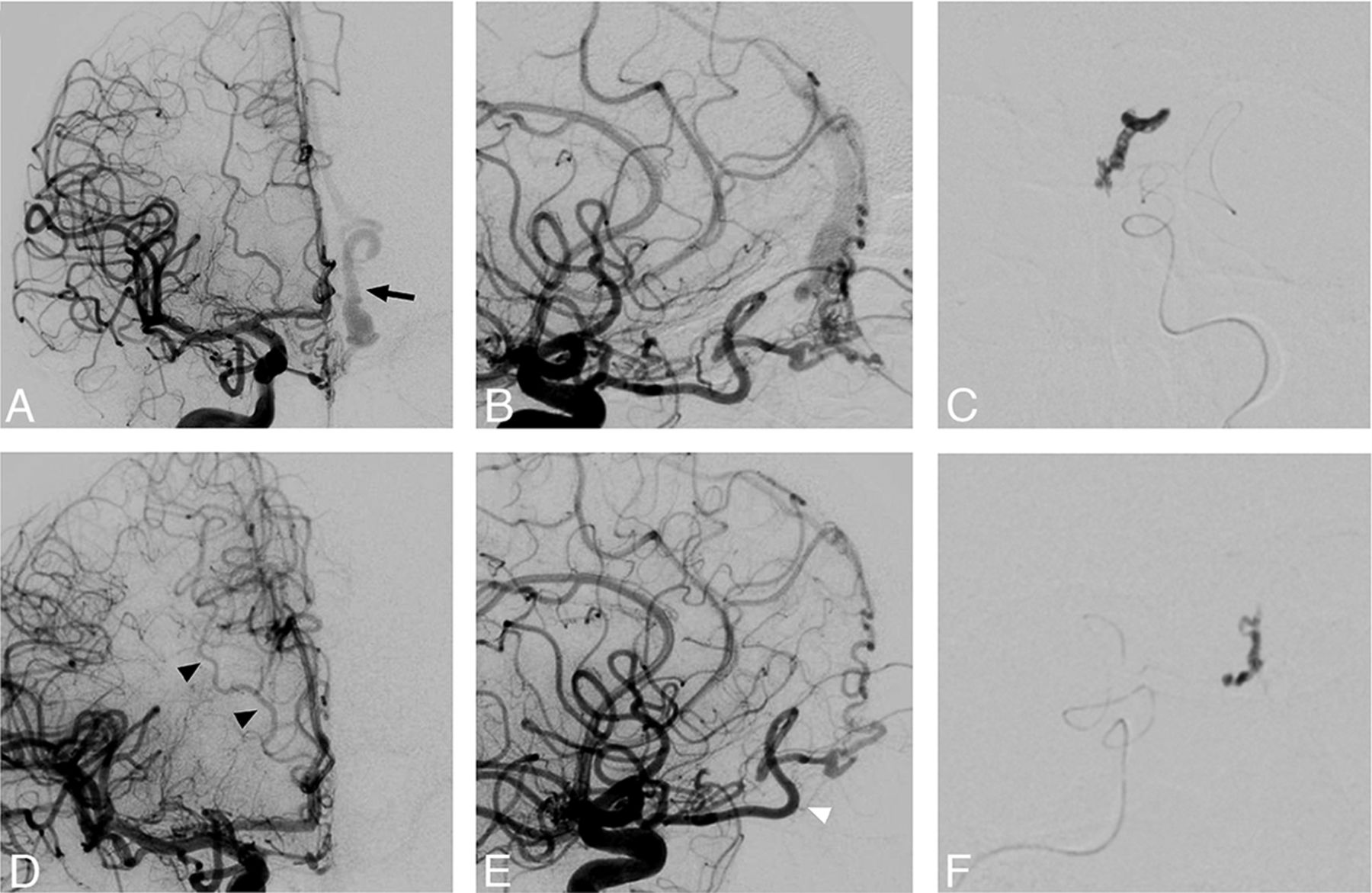
A total of 15 ACF-dAVFs were described for 14 patients, because 1 patient was found to have 2 ACF-dAVFs with separate arterial feeders and venous drainage (Fig 1). All ACF-dAVFs were supplied by the ophthalmic artery; in 67% of cases (n = 10), there was bilateral supply from the ophthalmic artery. Additional dural feeders were seen from the internal maxillary artery (n = 5), middle meningeal artery (n = 3), and facial artery. Pial feeders were seen in 1 ACF-dAVF through a branch from the orbitofrontal artery. All ACF-dAVFs showed drainage through cortical veins before entering the venous sinus (Borden type III). All ACF-dAVFs drained to the superior sagittal sinus, while 2 showed additional drainage to the cavernous sinus (n = 2) and superficial middle cerebral vein, connected through the vein of Labbé to the sigmoid sinus (n = 1).

A patient with 2 dAVFs with separate arterial feeders and venous drainage. A right-sided injection of the ICA shows a dAVF with supply from the right ophthalmic artery with drainage through a dilated cortical vein on the left side (arrow) into the superior sagittal sinus (A and B). After successful embolization through 1 of the 2 ethmoidal branches of the left ophthalmic artery (C), a repeat right ICA injection clearly shows the second remaining fistula with separate transethmoidal supply refluxing into a nondilated vein on the right-sided cortical frontal vein (arrowheads) into the superior sagittal sinus. The bayonet sign is seen, signifying the origin of the central retinal artery (white arrowhead, D and E). Because the first embolization was performed without substantial arterial reflux, the second fistula was again successfully embolized through the right ophthalmic artery (F).
Treatment and Outcome
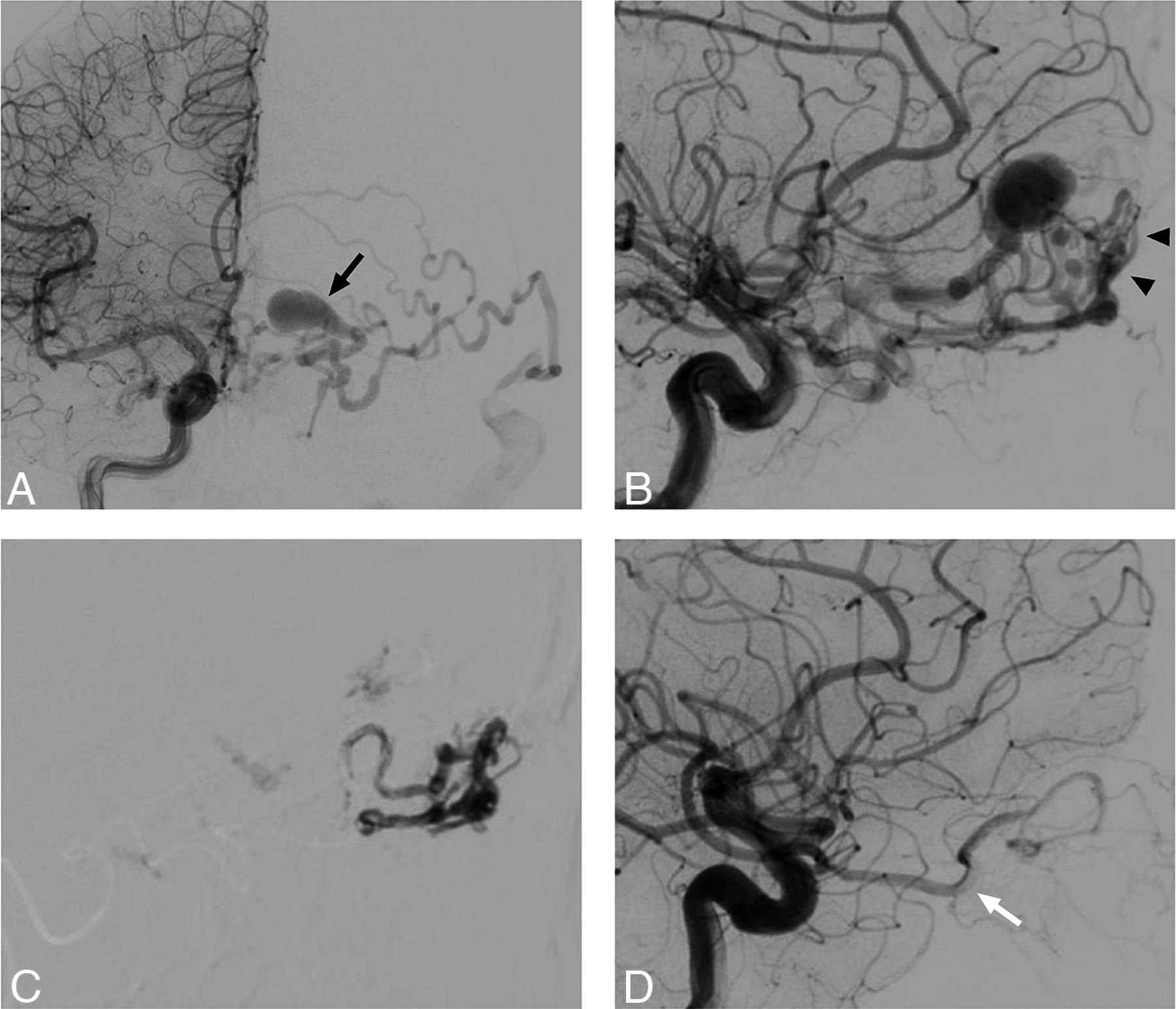
All patients underwent primary endovascular treatment (Table). Complete occlusion using endovascular treatment was achieved in 79% of patients (11/14). In 13 patients, transarterial catheterization was performed. In 11 of these patients with 12 ACF-dAVFs, embolization was attempted with a total of 14 glue injections through the ophthalmic artery (10 unilateral and 2 bilateral) with a mean injection time of 31 (SD, 8) seconds; range, 25–38 seconds). Additionally, 1 glue injection was through the middle meningeal artery, and 1 glue injection, through a pial feeder from the orbitofrontal artery. Using only transarterial embolization, we achieved complete occlusion in 69% of patients (9/13) (Fig 2). In 1 patient with unsuccessful transarterial embolization, subsequent transvenous embolization was performed in the same session with complete occlusion of the ACF-dAVF. A primary transvenous approach was used in 1 patient because of high fistulous flow and very unfavorable vascularization through multiple small dural arteries. Treatment resulted in complete occlusion of the ACF-dAVF by glue embolization of the proximal part of the draining vein.

A patient who presented with transient aphasia. Angiography demonstrated a dAVF with arterial feeding through ethmoidal branches of the right ophthalmic artery in a posterior-anterior projection (A), the left ophthalmic artery in a lateral projection (arrowheads) (B), and the frontal branch of the left middle meningeal artery (not shown). Cortical venous reflux is seen through ectatic left-sided cortical veins (arrow) toward the superficial middle cerebral vein before ending in the sigmoid sinus (A and B). Embolization through the right ophthalmic artery, with filling of the proximal refluxing vein with a minor spill of glue in the more distal venous territory (C). Complete occlusion of the fistula was achieved. The bayonet sign is seen, signifying the origin of the central retinal artery (white arrow) (D). The patient was asymptomatic at follow-up.
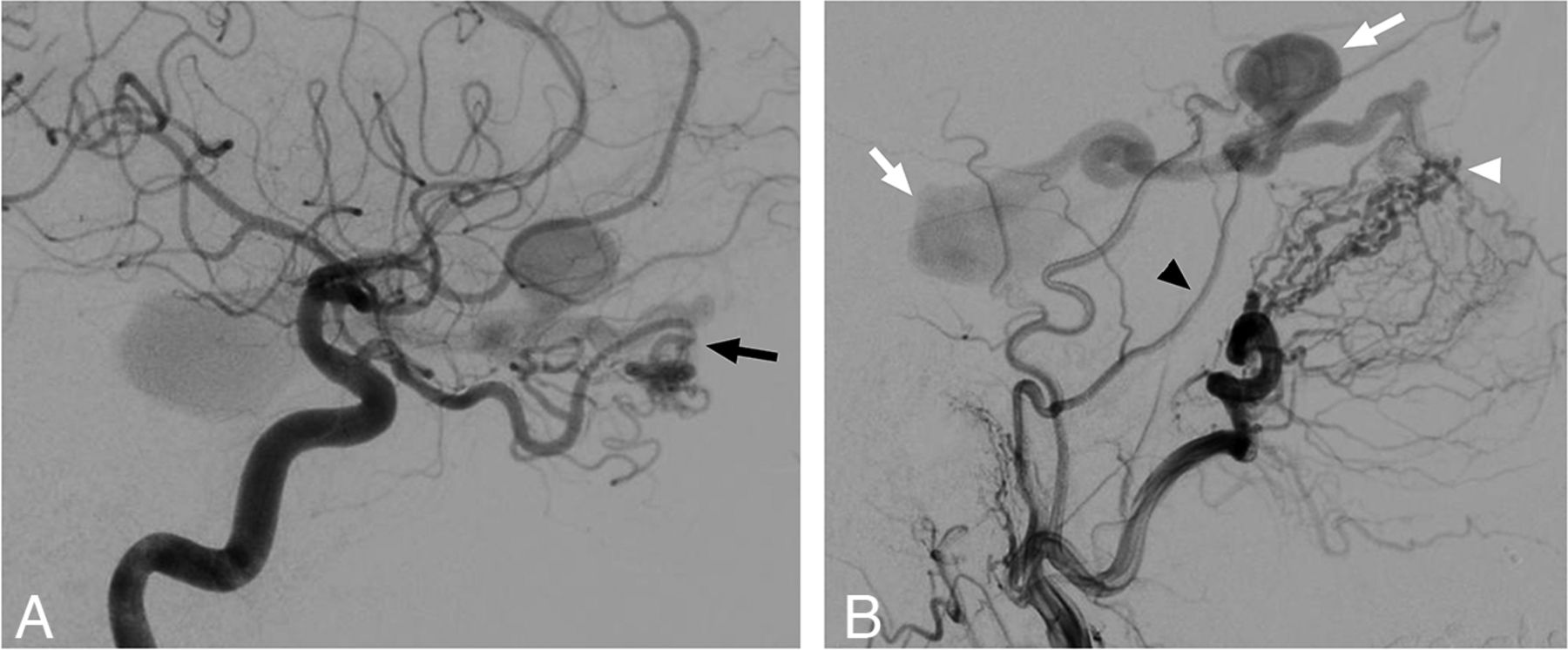
Endovascular treatment was unsuccessful in 3 of 14 patients (21%). One ACF-dAVF was only partially occluded despite multiple transarterial embolization attempts, which had to be halted due to progressive reflux of the embolic agent (Fig 3). In the remaining 2 patients, no embolization attempt was made because a distal-enough microcatheter position could not be obtained to allow safe embolization. All 3 patients were referred for surgery, with successful surgical disconnection of the ACF-dAVF.

A patient with a complex dAVF with extensive arterial supply from both ophthalmic arteries (arrow), right middle meningeal artery (arrowhead), and infraorbital branch from the maxillary artery (white arrowhead). Due to proximal elongation, the exact location of the bayonet cannot be determined (A and B). Multiple venous ectasias are visible along the cortical draining vein (white arrows). Embolization was attempted through both ophthalmic arteries, which had to be halted due to reflux before glue could reach the venous outlet. The patient finally underwent surgery, with successful disconnection of the fistula.
No procedural complications of endovascular treatment were seen. Visual acuity was preserved in all patients. Procedural complications were seen in 2 of 3 patients who underwent surgery. One patient developed postoperative anosmia, while another patient had transient postoperative symptoms attributed to a seizure.
Follow-Up
All patients had clinical follow-up with a median length of 13 months (range, 4–94 months). At last follow-up, 12 patients (86%) had an mRS of 0–2. Two patients had a poor clinical outcome (mRS 3 and 4) related to neurologic damage from the initial hemorrhage.
DISCUSSION
In this study, we describe outcomes of patients who were treated for ACF-dAVF using transarterial embolization with n-BCA as a first-line approach. Transarterial embolization reached direct, complete occlusion in 69% of patients. Overall, endovascular treatment including transvenous and combined approaches reached complete occlusion in 79% of patients. No procedural complications from endovascular treatment were seen. Visual acuity was preserved in all patients. Three patients underwent secondary surgery after failed endovascular treatment. All patients had complete ACF-dAVF occlusion at follow-up.
ACF-dAVFs are exceedingly rare lesions. The classification of “aggressive” subtype should be nuanced because modern literature has shown relatively lower rates of hemorrhage, ranging from 27% to 57%,3⇓-5 compared with the high rates of hemorrhage (62%–91%) reported in earlier literature.12,13 The hemorrhage rate of 21% in our study supports this notion and underlines the importance of a noninvasive first-line treatment approach. Previous studies on endovascular treatment of ACF-dAVFs have shown complete occlusion rates ranging from 53% to 92% and complication rates ranging from 3.6% to 12%.2⇓⇓-5,14 In a recent study, 23 patients underwent transarterial ACF-dAVF embolization using varying types of embolic agents (n-BCA, Onyx, and Squid).3 In this study, 1 case of central retinal artery occlusion occurred due to excessive reflux of Onyx. To our knowledge, no other cases of central retinal artery occlusion after embolization through the ophthalmic artery have been published, though this complication is likely underreported. When one performs embolization through the ophthalmic artery, only minimal reflux is allowed due to the proximity of the central retinal artery.15 Because copolymers require reflux to provide forward push of the embolic agent, from a procedural point of view, these are unfavorable in this procedure compared with n-BCA, which allows better control of reflux. In our study, only 13% of n-BCA injections through the ophthalmic artery (2/15) had to be aborted due to reflux, and this reflux could be safely managed without embolic material nearing the origin of the central retinal artery. In all other cases, no reflux occurred proximal to the tip of the microcatheter.
The experience of the neurointerventionalist does play an important role in the choice of the embolic agent, which might explain the predominant use of Onyx in all major studies on transarterial embolization of ACF-dAVF.3⇓-5,14,16,17 Two recent case reports have indicated that micro-balloon-assisted embolization might be used to avoid Onyx reflux through the ophthalmic artery.18,19 However, the more difficult navigation and risk of vessel perforation due to balloon inflation should be taken in account under these circumstances. In our opinion, the use of n-BCA in our study is an important factor in the relatively high rate of successful transarterial embolization without occurrence of complications.
Several technical aspects are important to consider when using a transarterial approach. In our center, we prefer very distal catheterization of the ophthalmic artery with very soft-flow-directed microcatheters allowing injection of diluted n-BCA for treatment of ACF-dAVFs. This approach allows control of the antegrade injection of the embolic agent with only very sparse reflux. The aim of embolization should be occlusion of the proximal venous outlet. Partial or absent occlusion of the proximal venous outlet and persistent outflow after occlusion of the primary arterial feeder might induce the development of secondary feeders through collateral arteries, with persistent flow through the dAVF and a continued risk of hemorrhage. Reflux of the embolic agent should not be allowed close to the origin of the central retinal artery. In most cases, the origin of the central retinal artery can be found where the ophthalmic artery crosses the optic nerve with the classically described “bayonet” appearance.15 However, under arteriovenous high-flow conditions, the ophthalmic artery will show elongation, making identification of the bayonet more challenging. In addition, the central retinal artery will hardly be opacified because of the steal effect toward the fistula. In such cases, any risks should be minimized by obtaining a very distal position and by allowing only minimal reflux. Furthermore, a wedge position of the microcatheter is preferred to reduce reflux. A transvenous approach can be used in cases with drainage to the superior sagittal sinus, though it is important to evaluate the venous anatomy, tortuosity, and presence of venous ectasia to estimate the likeliness of safely obtaining a distal position for embolization.
Limitations of our study included the retrospective nature of the study, which prohibited exhaustive data collection. However, patients were included consecutively, and a consistent treatment approach was used during the study period. Although several larger multicenter studies on endovascular treatment of ACF-dAVFs have been published, these have inconsistencies in treatment approaches, technique, and types of embolic agents used for embolization.3⇓-5,14 Our study is the largest single-center study on transarterial embolization of ACF-dAVFs to date. Prospective registry studies could be used for comparison of treatment strategies of ACF-dAVFs.
CONCLUSIONS
Our study shows that endovascular treatment using transarterial embolization with n-BCA as a first-line approach is a safe and feasible treatment strategy for ACF-dAVF. Although copolymers have seen increased usage compared with n-BCA, we recommend maintaining experience with n-BCA for specific indications such as ACF-dAVF.
| Variable | Value (%) (No.) |
|---|---|
| Primary endovascular treatment | 100% (14/14) |
| Transarterial | 86% (12/14) |
| Transvenous | 7% (1/14) |
| Combined | 7% (1/14) |
| Secondary surgery after failed endovascular treatment | 21% (3/14) |
| Endovascular outcome | |
| Complete occlusion | 79% (11/14) |
| Partial occlusion | 7% (1/14) |
| No embolization attempt | 14% (2/14) |
| Clinical outcomea | |
| Asymptomatic | 29% (4/14) |
| Improvement of symptoms | 71% (10/14) |
| Worsening of symptoms | 0% (0/14) |
| Death | 0% (0/14) |
| Procedural complications | |
| Endovascular treatment | 0% (0/14) |
| Surgery | 67% (2/3) |
| Seizure | 33% (1/3) |
| Anosmia | 33% (1/3) |
↵a This concerns symptoms attributed to the dAVF.
Treatment characteristics
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received August 11, 2023.
- Accepted after revision November 2, 2023.
- © 2024 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}