
Abstract
SUMMARY: We report a rare and unique complication of ventriculoperitoneal (VP) shunt malfunction. A progressively expansile, CSF-containing occipital intradiploic cyst developed in a 15-year-old boy at the site of cystoperitoneal shunt draining a Dandy-Walker cyst; the shunt was placed when the boy was 4 years old. A proposed pathogenesis of the lesion is discussed.
Many complications of ventriculoperitoneal (VP) shunts have been previously described from common complications (eg, tube disconnection/obstruction, infection, and intraperitoneal CSF pseudocyst) to more esoteric ones (eg, bowel perforations, pleural effusions, shunt migration to the heart, and extrusion into or through the anus/vagina/scrotum).1,2 We report the case of a 15-year-old boy with a previous medical history including a diagnosis of a Dandy-Walker cyst with hydrocephalus, which required a VP shunt at age 6 months and a posterior fossa Dandy-Walker cystoperitoneal shunt connecting to the VP shunt through a Y connector at age 4 years. At 15 years old, the boy had an asymptomatic large, expansile, intradiploic occipital cyst containing CSF as a result of a disconnected VP shunt tube in the chest wall and an occluded intracranial catheter of the posterior fossa cystoperitoneal shunt.
Case Report
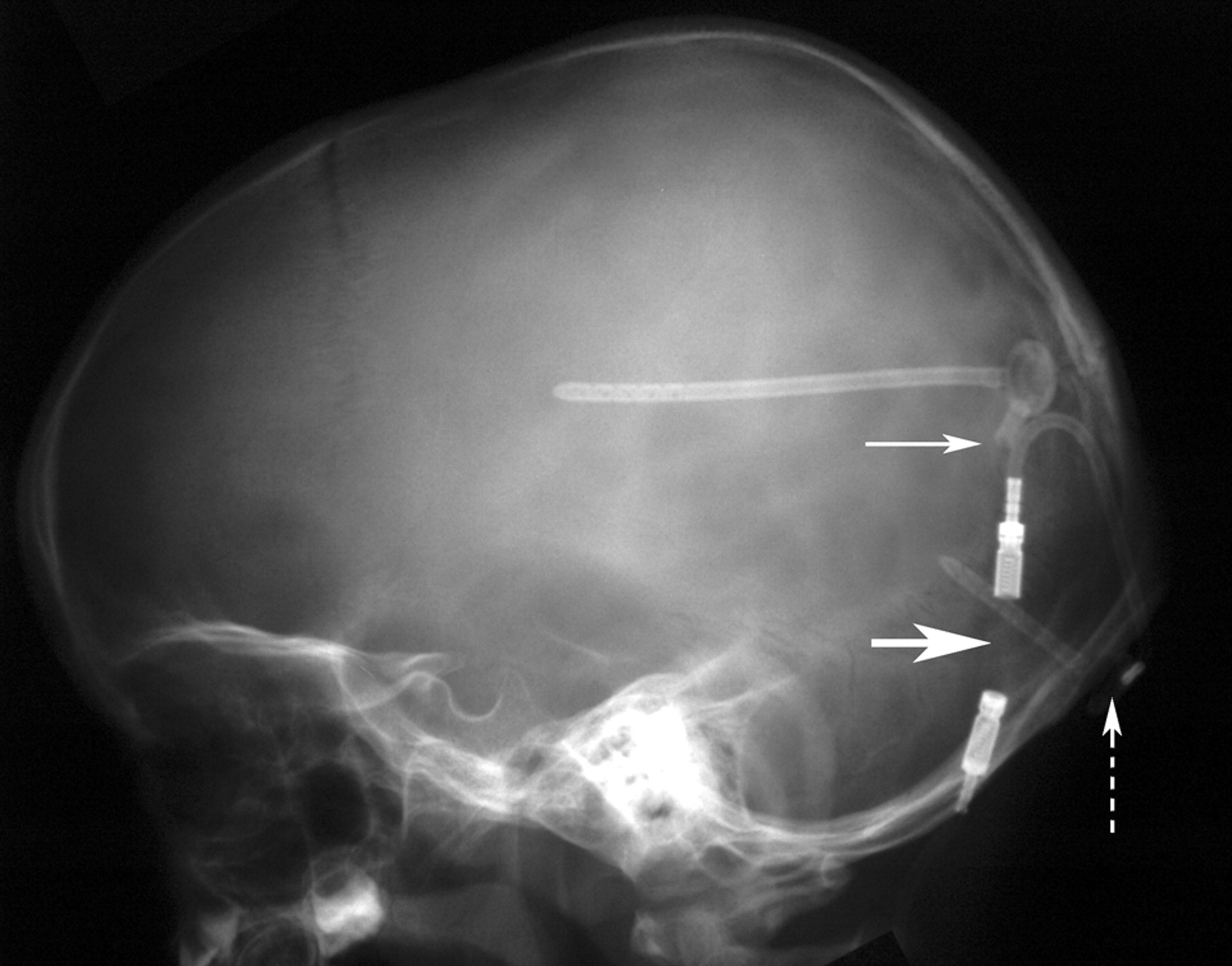
The reported patient is a 15-year-old boy who presented for a VP shunt evaluation before trying out for a football team. At age 6 months, the patient was diagnosed with a Dandy-Walker cyst and had a VP shunt placed for relief of his hydrocephalus. At age 4 years, the patient experienced progressive headaches and projectile vomiting and was found to have a disconnected shunt. MR imaging examination showed an enlarging Dandy-Walker cyst with compression of the brain stem and cerebellum. A cystoperitoneal shunt was placed, which was connected to the repaired VP shunt via a Y connector (Fig 1). At the time of surgery, it was found that the Dandy-Walker cyst was under pressure.

Lateral skull radiograph performed in our patient at age 4 years shows cystoperitoneal shunt connected to a VP shunt via a Y connector (dashed arrow, reservoir of cystoperitoneal shunt; small arrow, Y connector; large arrow, unidirectional valve).
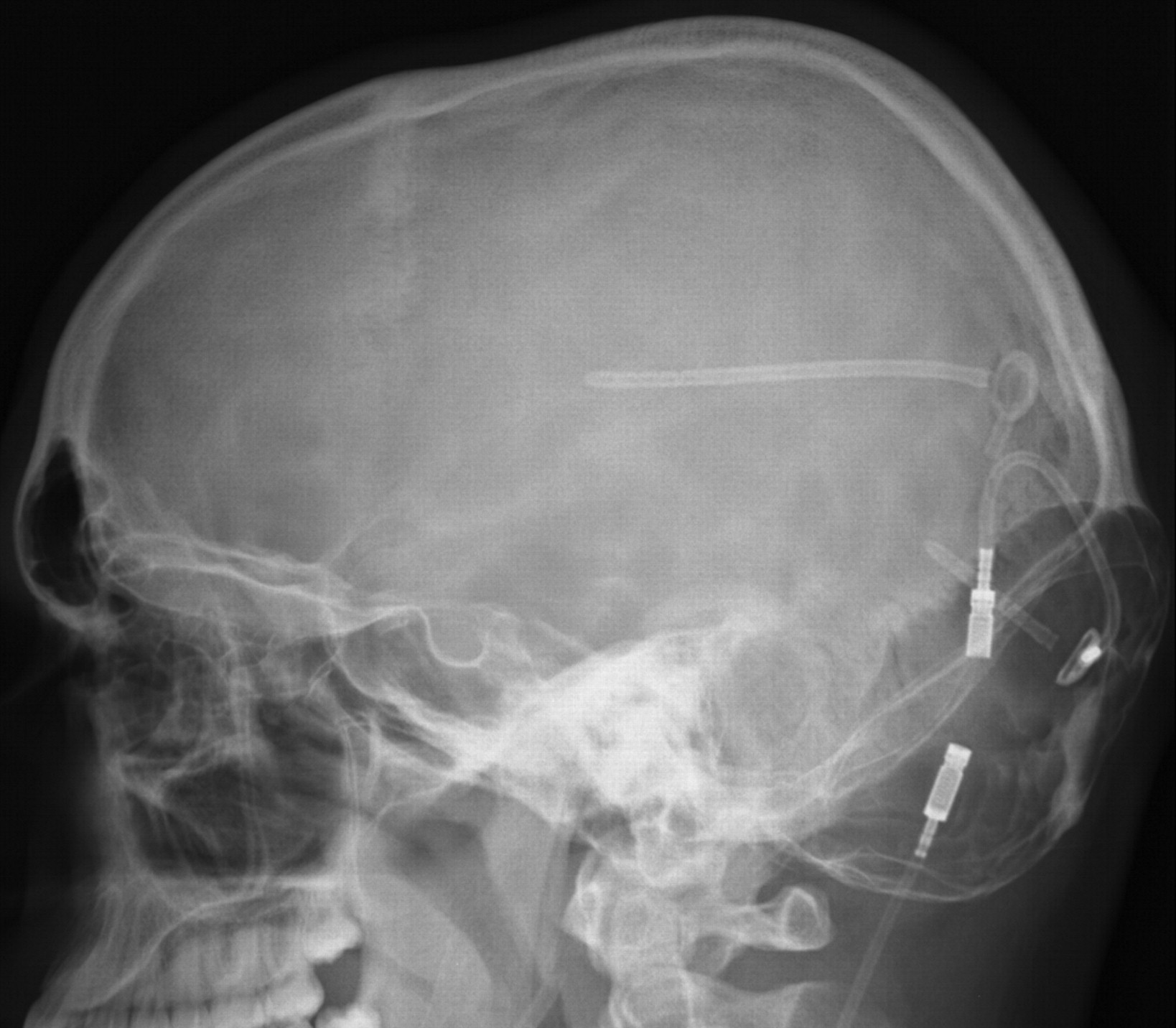
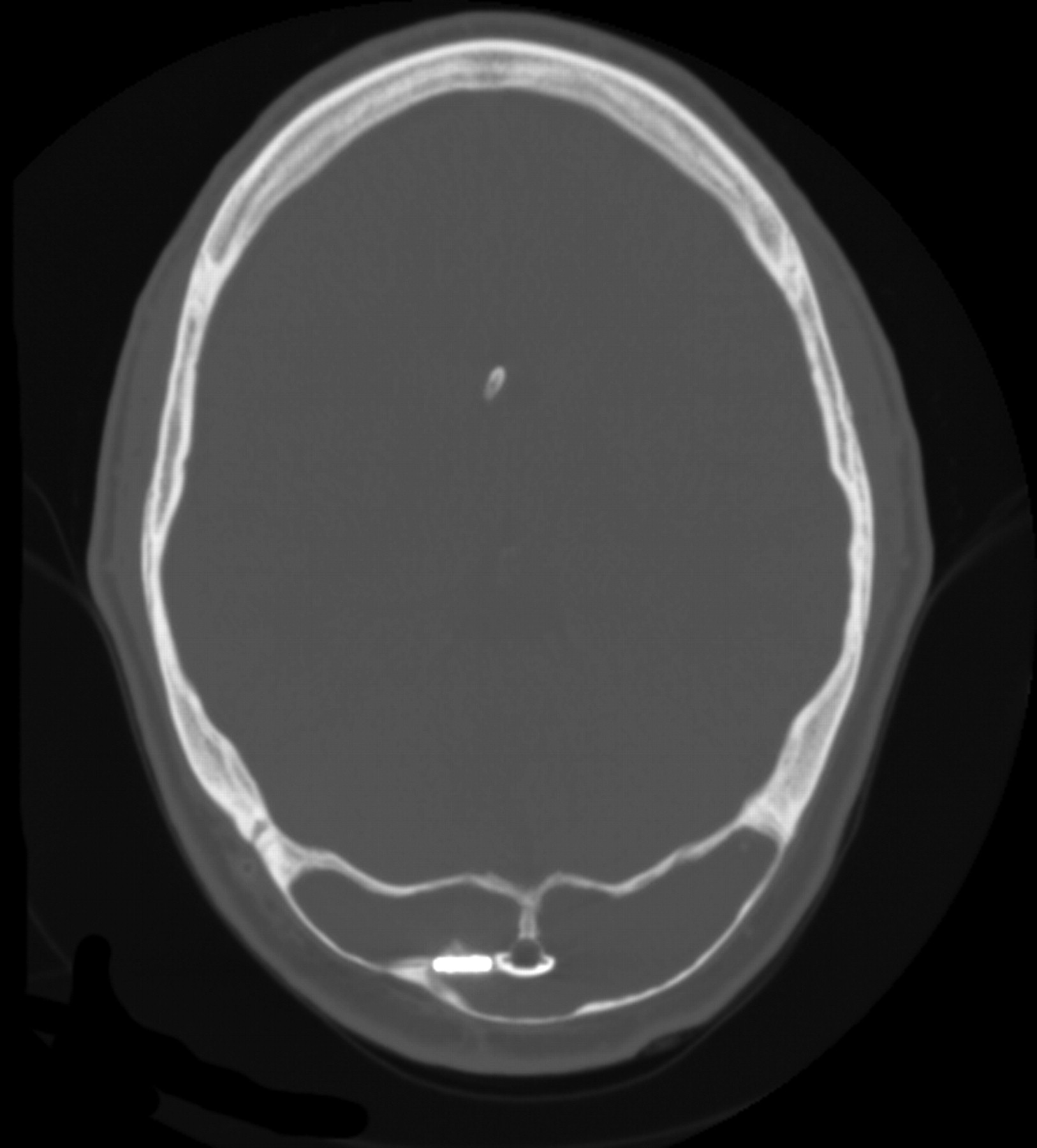
When the patient presented for a football pregame check-up at age 15 years, he was asymptomatic and denied any signs or symptoms of shunt malfunction. Plain radiographs revealed a break in the shunt catheter at the level of the right upper chest. Skull radiographs showed a cystic expansion of the occipital diploic space measuring 10 × 10 × 5 cm in the transverse, superoinferior, and anteroposterior dimensions, respectively (Fig 2). The reservoir of the posterior fossa cystoperitoneal shunt had migrated into the enlarged diploic space. Head CT examination confirmed the intradiploic location of the reservoir and the expansion of the diploic space extending from the supraoccipital into the basioccipital part of the occipital bone, including the occipital condyle and lower clivus (Fig 3).

Lateral skull radiograph performed in our patient at age 15 years shows development of intradiploic cyst of the occipital bone.

CT image shows expansile loculation in the occipital bone. The reservoir of the cystoperitoneal shunt has migrated in the diploic space.
The patient was taken to the operating room, where it was found that the protruded occipital outer table was paper thin and the expanded diploic space contained CSF under pressure. The intracranial catheter of the cystoperitoneal shunt was found to be occluded. The intracranial cystoperitoneal shunt catheter was replaced, and the VP shunt was revised.
Discussion
Occipital intradiploic expansile cysts containing CSF have been described as a rare entity, and only 14 cases have been previously reported under various search terms including “intradiploic arachnoid cyst,” “intraosseous leptomeningeal cyst,” and “intradiploic growing skull fracture.”3-8 To the best of our knowledge, no cases of intradiploic expansile CSF cysts as a complication of shunt procedures have been reported in the literature.
The clinical presentation of previously reported patients may include a palpable mass, headache, ataxia, and visual field defects. Most cases of occipital intradiploic CSF cysts have been reported in the adult population. Almost all of these patients have had a previous history of head trauma with or without occipital fracture. The history of head injury ranges from very recent to as much as 50 years previously. Radiographic, CT, and MR imaging findings of previously reported cases include expansile, intradiploic, CSF-containing cysts that may be unilocular or multilocular. The expanded outer table is generally maintained without interruption, but the inner table may be interrupted with continuation of the posterior fossa subarachnoid space to the intradiploic cyst. In some cases, communication of the cyst to the posterior fossa subarachnoid space was demonstrated by pneumoencephalography or nuclear cisternography.3,4
This entity seems to be independent from so-called growing skull fractures (leptomeningeal cysts), which develop as sequelae of diastatic fractures with disruption of the dura mater as well as the inner and outer tables, most often involving the vertex of the calvaria (membranous calvaria). These injuries are almost exclusively seen in infants younger than age 3 years.9 Intradiploic CSF-containing cysts occurring in the calvaria other than the occipital bone are extremely rare.6,10
The pathogenesis of the occipital intradiploic cyst has been hypothesized as originating from insinuation of the arachnoid membrane into the occipital diploic space through the traumatic lent of the dura mater and inner table and subsequent intradiploic expansion by CSF pulsation.5 Expansile driving forces such as coexisting hydrocephalus, brain edema, or an actively growing child's brain were thought to facilitate the growth of the cyst.6 Among the cases in which a history of a traumatic injury was absent, extension of the arachnoid diverticulum into the diploic space through a small congenital defect of the dura mater was hypothesized as the cause.11 The thick musculature covering the occiput was thought to prevent the erosion of the outer table, allowing considerable expansile growth.7
In our case report, our hypothesis is that CSF communication was established between the Dandy-Walker cyst to the occipital diploic space through the surgically created dural and inner table defect. The disconnected VP shunt resulted in increased pressure on the Dandy-Walker cyst as well as in the ventricular system, facilitating the egress of CSF around the occluded catheter of the cystoperitoneal shunt into the diploic space and increasing cyst growth.
We also believe that the occipital predilection of this entity is explainable by the unique embryogenesis of the occipital bone. The supraoccipital portion of the occipital bone between the mendosal suture and the foramen magnum is cartilaginous in origin, similar to the basioccipital portion, contrary to the membranous origin of the rest of the calvaria.12 The thicker inner and outer table and more capacious diploic space of the occipital bone allow the growth of a large, intradiploic fluid collection.
In summary, we reported a rare and unique complication of a VP shunt. A progressively expansile, CSF-containing occipital intradiploic cyst developed at the site of a cystoperitoneal shunt draining a Dandy-Walker cyst in a 15-year-old boy.
Footnotes
Paper previously presented at: Annual Meeting of the American Society of Neuroradiology, June 3, 2008; New Orleans, La.
References
- Received August 4, 2008.
- Accepted after revision August 13, 2008.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.