
The “hot cross bun” sign refers to pontine cruciform hyperintensity on long TR sequences, which can be observed in multiple-system atrophy, spinocerebellar atrophy types 2 and 3,1 and in parkinsonism secondary to vasculitis.2 It has not been previously demonstrated in variant Creutzfeldt-Jakob disease (vCJD), to our knowledge.
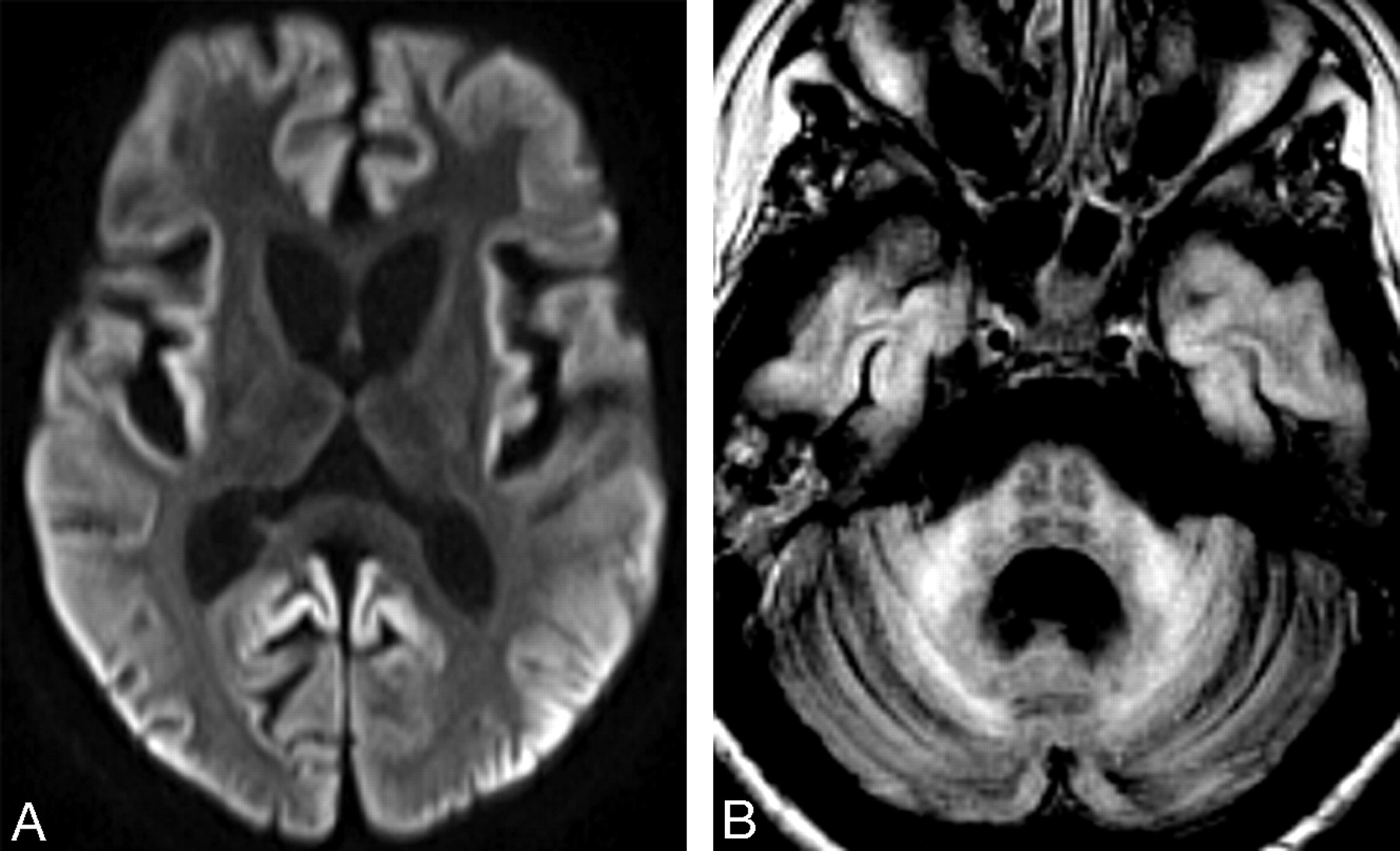
A 16-year-old girl, diagnosed with vCJD at age 14 years and described in detail elsewhere,3 had progressive clinical deterioration, leading to a persistent vegetative state. MR imaging at 18 months after onset of the disease showed global brain atrophy and widespread restricted cortical diffusion (Fig 1A). Pontine cruciform hyperintensity was seen on fluid-attenuated inversion recovery images (Fig 1B).
It is believed that the “hot cross bun” sign results from pontine nuclei neuronal loss and pontocerebellar tract degeneration, with preserved corticospinal tracts. In vCJD, cerebellar involvement is prominent, characterized by marked neuronal loss, astrocytosis, and florid plaques.4 In addition, spongiform changes have been detected in pontine nuclei.4 Secondary degeneration of pontocerebellar tracts is therefore likely to occur, thus supporting our observation. The presented case expands the differential diagnosis of neurodegenerative conditions in which the “hot cross bun” sign can be found.

A, Axial diffusion-weighted image shows symmetric striatal and thalamic atrophy and widespread cortical high signal intensity. Apparent diffusion coefficient maps (not shown) revealed corresponding decreased cortical signal intensity, confirming restricted water diffusion. B, Axial fluid-attenuated inversion recovery image demonstrates pontine “hot cross bun” sign, atrophic and hyperintense middle cerebellar peduncles, global cerebellar atrophy, and cortical temporal lobe high signal intensity.
- Copyright © American Society of Neuroradiology





{kind=link}