
Abstract
BACKGROUND AND PURPOSE: The development of new non–ocular-toxic drugs has enabled infraophthalmic chemotherapeutic infusion. We assessed whether streaming occurs with infraophthalmic, high cervical internal carotid artery (ICA) delivery of chemotherapeutic agents by means of conventional angiographic catheters.
METHODS: Six patients with high-grade gliomas treated with monthly carotid intraarterial chemotherapy were studied. Chemotherapy delivery and distribution was modeled by technetium 99m hexylmethyl-propyleneamine oxine (HMPAO), a first-pass agent. Each patient received 0.5 mCi (18.5 MBq) of 99mTc-HMPAO in 50-mL of saline intraarterially in the ICA at the C1–C2 level. Injections were given twice, at two different injection rates: 0.08 mL/s at one therapeutic session and 6 mL/s a month later. The slow injection rate modeled the slowest rate used in the delivery of chemotherapy into the ICA. The higher rate was selected to avoid any possibility of uneven mixing, by replacing intracarotid blood completely and by using a turbulent injection rate that destroys laminar flow and intraarterial streaming. Single photon emission CT (SPECT) was performed 2 hours after injection. For each patient, the corresponding SPECT sections at the two injection rates were compared.
RESULTS:No differences were noted in 99mTc-HMPAO distribution between the two injection rates in any of the patients. However, some of the rapid injection rate SPECT scans showed extension of the 99mTc-HMPAO uptake into adjacent watershed territories.
CONCLUSION: There was no evidence, in humans, of substantial streaming during slow infraophthalmic intracarotid injections. Slow rates of infusion are as good as high rates for infraophthalmic intracarotid drug delivery. This is of special importance for drugs that are not tolerated at high injection rates. Moreover, infraophthalmic intracarotid chemotherapeutic infusion does not require special injectors or catheters.
Standard treatment for patients with malignant primary brain tumors has long been a combination of surgery and radiation therapy. Repeated surgical excision alone was shown to be ineffective (1), and radiation therapy is potentially harmful to the patient because of delayed complications such as dementia, white matter changes, atrophy, and delayed radiation-induced necrosis of the brain (2, 3). Chemotherapy frequently is added to brain tumor treatment protocols, in which case it can be given systemically (orally or intravenously) and sometimes may be delivered regionally by intraarterial infusion (4). Intraarterial chemotherapy increases tumor uptake of chemotherapeutic drugs (5) and increases plasma concentration of the drug during the first passage through the circulation. Also, intraarterial chemotherapy for brain tumors (intracarotid or intravertebral) was found to have a very low angiographic complication rate (6). Yet, increased tissue drug concentration achieved by intraarterial drug chemotherapy may induce increased occurrences of local toxic reaction (7, 8), one example being eye toxic reaction. The original chemotherapeutic agents available for intracarotid injection were toxic to the eye. Therefore, initial trials of intracarotid delivery of chemotherapy focused on supraophthalmic injections. Avoiding the eye, supraophthalmic injection of chemotherapeutic agents was still associated with substantial brain neurotoxicity. One cause for neurotoxic reaction in the brain was intravascular drug streaming that led to uneven drug distribution, with low concentration of the drug in some regions and undesirably high concentrations in other areas (9). Prerequisites for streaming are an injection rate slower than the flow rate in a stream with laminar flow and short distance from the injection site to the closest downstream branching site (10). The supraophthalmic carotid artery has laminar flow and a short distance to its bifurcation; therefore, injection rate was the only parameter that could be changed to avoid streaming. A few trials that evaluated different injection rates concluded that high injection rates are needed to avoid streaming in supraophthalmic chemotherapeutic delivery (9, 11). Another successful technique to relieve the effect of laminar streaming is diastole-phased pulsed infusion (8, 10, 12, 13).
Little attention was paid to the possibility of streaming affecting distribution in the brain with infraophthalmic injections (10, 14). Recently, non–ocular-toxic chemotherapeutic agents have become available, and infraophthalmic injections are being used again. This has generated increased interest in infraophthalmic delivery of chemotherapeutic agents without or with disruption of the blood-brain barrier. We assessed, in humans, whether different rates of intraarterial drug injection affect the cerebral distribution of infraophthalmic intracarotid chemotherapy. Our aim was to search for ways to lower the chance of heterogeneous cerebral drug distribution in infraophthalmic chemotherapeutic injections. Homogeneous cerebral drug distribution would prevent subtherapeutic tumor drug concentrations and at the same time minimize neurotoxic reaction in the normal surrounding brain.
Methods
This study was approved by our institutional review board. Six patients (three men and three women; mean age, 46.6 years; range, 29–61 years) participated in our study. All patients had supratentorial tumors diagnosed by surgery or biopsy. Five patients had glioblastoma multiforme, and one patient had an anaplastic oligodendroglioma. Patients were referred for monthly infraophthalmic intracarotid chemotherapy if their tumor recurred after surgery and radiation therapy. Intraarterial chemotherapy was infused through those arteries that supplied the enhanced tumor. All patients selected for this study had tumors supplied by the carotid arteries. Patients participated in the study after providing written informed consent.
The catheter used for infusion was a 4F JB1 Glide hydrophilic that accepts a 38 guide (Terumo, Tokyo, Japan). Chemotherapy was delivered into the carotid artery at the C1–C2 level. The procedure was performed under direct fluoroscopic visualization and with local anesthesia through a femoral approach. Two chemotherapeutic drugs were injected in tandem: carboplatin 400 mg/m2 and etoposide phosphate 300 mg/m2. Each agent was diluted in 200 mL and infused intraarterially over 7 minutes. Chemotherapy delivery and distribution was modeled by technetium 99m hexylmethyl-propyleneamine oxine (HMPAO), a first-pass agent. Immediately after chemotherapeutic infusion, each patient received 0.5 mCi (18.5 MBq) of 99mTc-HMPAO in 50 mL of saline intraarterially through the catheter used for delivery of the chemotherapeutic agents, at two different injection rates: a slow (continuous) injection rate of 0.08 mL/s at one therapeutic session and a rapid (bolus) injection rate of 6 mL/s in another session. The slow injection rate modeled the slowest rate used in the delivery of chemotherapy in the internal carotid artery (ICA). The higher rate was selected to avoid any possibility of uneven mixing, by replacing intracarotid blood completely and by using a turbulent injection rate that destroys laminar flow and intraarterial streaming. Single photon emission CT (SPECT) radionuclide images were obtained within 2 hours, with use of a dual-headed rotating gamma camera system (Helix; Elscint, Haifa, Israel) by using a low-energy high-resolution collimator. Processing included normalization, back-projection, filtering, and reconstruction.
The Statistical Parametric Mapping (SPM99; Wellcome, London, U.K.) software package was used for normalizing and registering the SPECT studies of the two injection rates (15). The images were compared visually. In addition, the SPM99 software was used for subtracting the two registered images and normalizing them by dividing each pixel of the subtracted image by the average pixel value of the rapid injection rate study. The percentage of pixels with more than 20% difference in intensity between the two injection rates was calculated for each patient.
Results
No visibly significant difference was noted in 99mTc-HMPAO distribution between the two injection rates in any of the patients (Figs 1 and 2). In some of the rapid injection rate cases, however, the SPECT scans showed extension of 99mTc-HMPAO uptake into adjacent watershed territories (Figs 1 and 2). Table 1 summarizes the region-of-interest size and the pixel intensity difference between the two injection rates for the six patients. For the six patients, a mean ± SD of 8.4 ± 6.3% of pixels had a greater than 20% difference in intensities between the two injection rates. No complications were noted after the angiographic procedure, including chemotherapeutic and radionuclide injections.
Discussion
Blacklock et al (9) were the first, to our knowledge, to suggest, in 1986, that a possible cause of focal toxic reaction induced by intraarterial injection of chemotherapeutic agents to brain tumors is nonuniform drug delivery owing to intravascular drug streaming. To investigate this phenomenon, this group examined the distribution of drug delivery after cervical ICA infusion in rhesus monkeys. They used carbon 14–labeled iodoantipyrine (IAP) delivered at a slow infusion rate (1–2% of ICA flow) or a fast infusion rate (20% of ICA flow) and found striking nonuniformity of drug delivery in the slow ICA infusion group. They concluded that drug administration at the slow infusion rate results in drug streaming, with markedly heterogeneous drug deposition in the perfused hemisphere. This may cause suboptimal drug levels in the tumor and toxic levels at other sites within the perfused hemisphere.
A few years later, still in animals, Saris et al (11) checked if streaming that occurs during ICA infusions could be eliminated in rats, with a fast retrograde infusion. In this study, 14C-IAP was infused retrograde through the external carotid artery into the common carotid artery by using three different rates: 0.45 mL/min (slow), 1.5 mL/min (medium), and 5.0 mL/min (fast). Streaming phenomenon was observed at the slow and medium rates of intraarterial infusion. The fast intracarotid infusion resulted in uniform isotope distribution.
Junck et al (16) were the first, to our knowledge, to attempt to determine whether the results in animals apply to humans. They injected oxygen 15 H2O through an infusion pump connected to a catheter terminating at the carotid bifurcation and then performed positron emission tomography (PET). Their conclusion was that mixing in the human carotid artery is complete or nearly complete over a wide range of infusion rates when injecting at the carotid bifurcation.
Saris et al (10) addressed the problem again in 1991, this time in 10 patients with malignant gliomas. They used H215O and PET with either continuous infusion or diastole-phased pulsatile infusion. They were surprised to discover (as did Junck et al [16]) that, as opposed to infraophthalmic ICA injections in animals, little or no streaming was demonstrated during infusion into the cervical portion of the ICA in humans. Saris et al thought of a few possible explanations for the difference between rats or monkeys and humans: 1) Larger vessel diameter in humans leads to greater turbulence and mixing in the human carotid artery, 2) greater vessel tortuosity and irregularity in humans increases mixing, and 3) there is a greater distance between the infusion site and distal branches in humans. Another explanation may be the possibility that PET, having a lower in-plane resolution than that of 14C autoradiography, made it difficult to document streaming even if it actually existed.
A couple of years later, Kosuda et al (14) performed a similar study by using 99mTc-HMPAO and SPECT imaging. With infraophthalmic continuous infusion, almost all injections yielded homogeneous distribution.
In the current study using SPECT, we demonstrated no evidence of substantial streaming or heterogeneous brain distribution of chemotherapy with infraophthalmic injections at a slow or fast rate. Our results support the findings by Kosuda et al and Saris et al and diminish the suspicion by Saris et al that PET, because of its low resolution (at that time), did not reveal actual streaming. Hence, we believe there is now enough evidence suggesting that there is no streaming in infraophthalmic ICA injections and no need for fast infusions or diastole-phased pulsatile infusions when using this technique for chemotherapeutic infusion, especially when experience indicates that supraophthalmic drug infusions are more toxic to brain tissue than are infusions into the cervical portion of the ICA (10).
Conclusion
Slow infusion rates are as good as high rates for infraophthalmic intracarotid drug delivery. With some drugs, slow rates are more tolerable to the patients, without the risk of inhomogeneous drug distribution and brain toxic reaction. Moreover, infraophthalmic intracarotid chemotherapeutic infusion does not require special injectors or catheters.

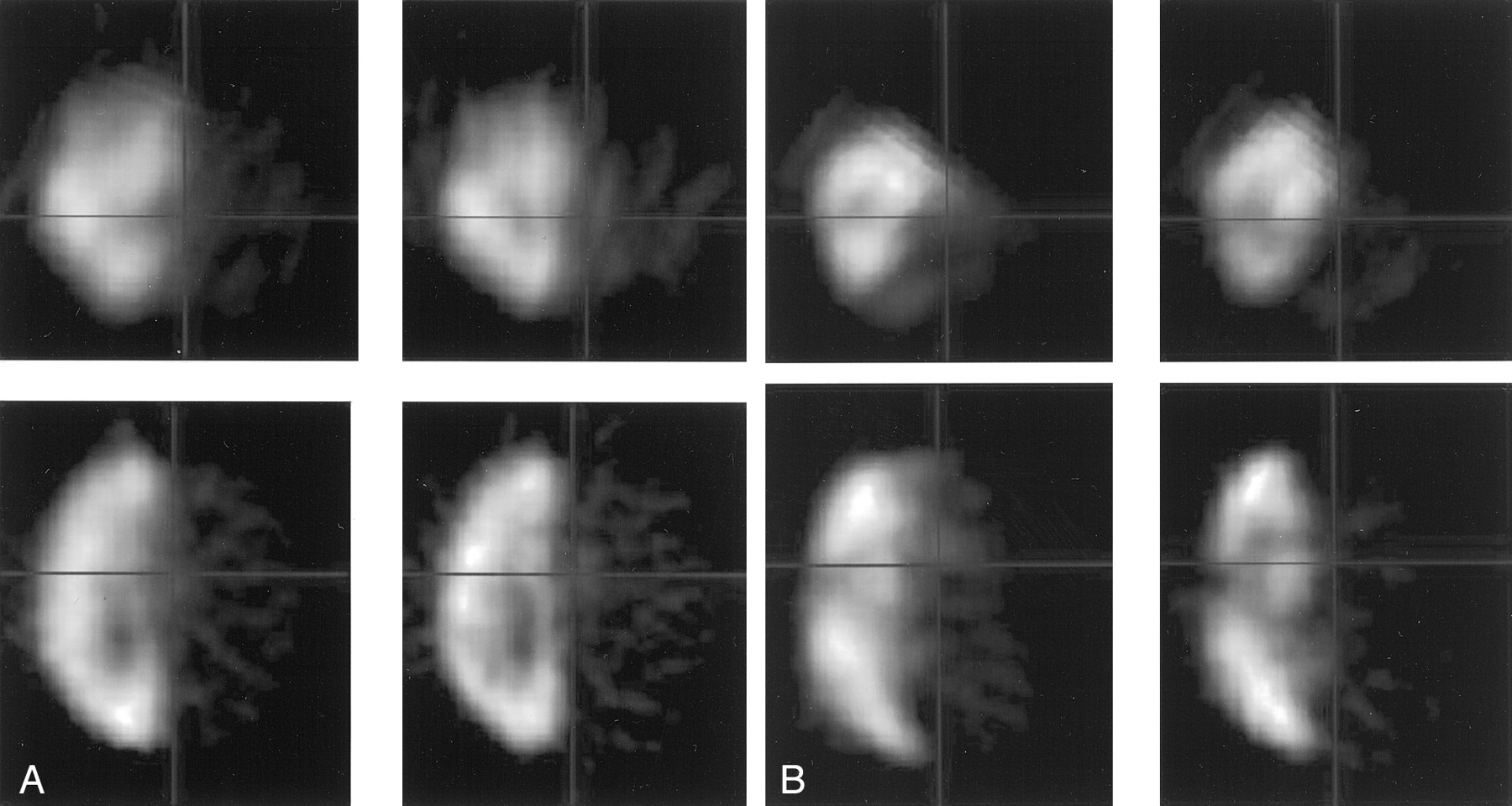
A and B, Registered and normalized 99mTc-HMPAO images at the two injection rates in two different patients (A and B) in coronal (top) and axial (bottom) planes. For each patient, the images on the left are after a rapid bolus injection and those on the right are after slow continuous injection. There is no visible difference between the two rates of injection, with the exception of minimal cross-flow to the contralateral frontal area on the bolus injection images in the second patient (B).

A selection of subtracted and normalized axial 99mTc-HMPAO SPECT images of the patient in Fig 1A highlights a subtle increased distribution of radionuclide in the occipital region. This is due to increased cross-flow from the carotid to the posterior circulation in the rapid bolus injection.
Summary of the region-of-interest size and the difference in uptake between the two injection rates for the six patients
Footnotes
Presented in part at the annual meeting of the Radiological Society of North America, Chicago, IL, November 26–December 1, 2000.
References
- Received June 21, 2001.
- Accepted after revision June 17, 2002.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.