
This article requires a subscription to view the full text. If you have a subscription you may use the login form below to view the article. Access to this article can also be purchased.
Graphical Abstract

Abstract
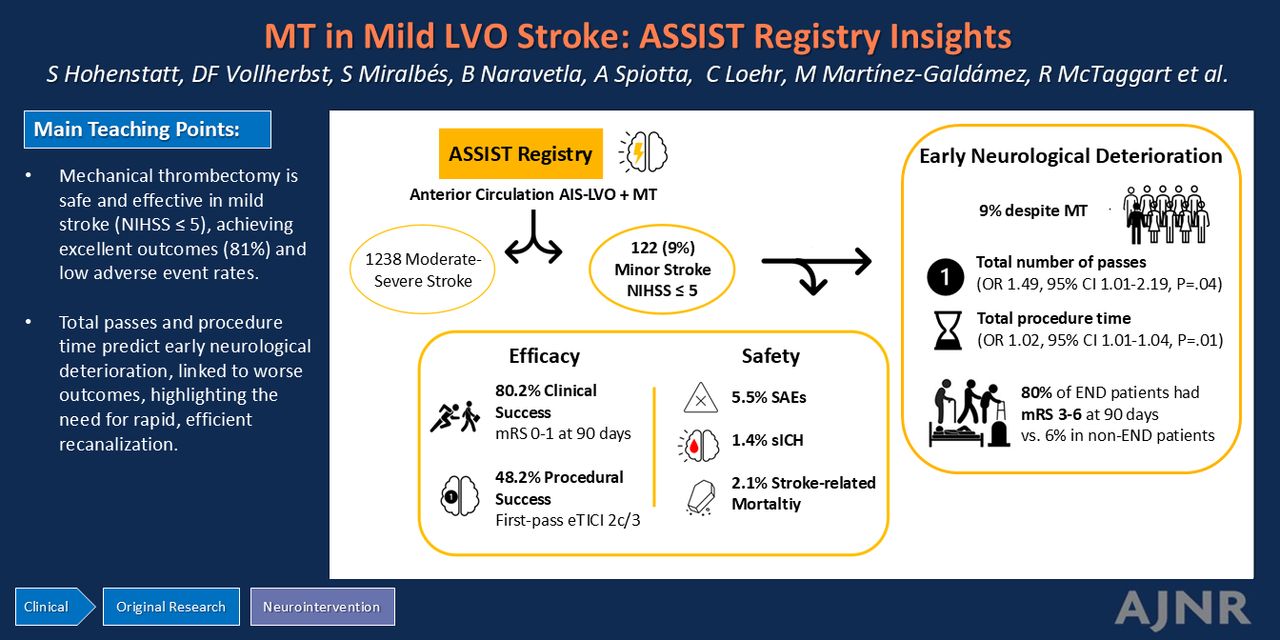
BACKGROUND AND PURPOSE: Mechanical thrombectomy (MT) is effective for acute ischemic stroke, yet its indication in mild stroke remains unclear. This study evaluates the effectiveness and safety of MT in patients with low NIHSS scores and assesses the impact of different MT strategies on procedural success and clinical outcomes.
MATERIALS AND METHODS: Data from the ASSIST Registry were analyzed. We categorized patients with large-vessel occlusion of the anterior circulation into mild (NIHSS ≤5) and moderate-severe (NIHSS >5) stroke groups. Baseline characteristics, procedural parameters, angiographic and imaging outcomes, clinical outcomes, and safety end points were compared. Within the mild stroke subgroup, outcomes were compared between different MT techniques.
RESULTS: Among 1360 patients with large-vessel occlusion, 122 had minor ischemic strokes (9%). Patients with mild stroke had high rates of excellent functional outcomes (mRS 0–1) at 90 days (77.1%) and functional independence (mRS 0–2) (85.7%). Procedural success rates were similar between NIHSS groups, while safety outcomes, except mortality, were comparable. No statistically significant differences were observed in treatment techniques within the mild stroke subgroup. Significant predictors of early neurologic deterioration (END) in patients with mild stroke were the total number of passes (OR, 1.49; 95% CI, 1.01–2.19; P = .04) and total procedural time (OR, 1.02; 95% CI, 1.01–1.04; P = .01). Patients with END were more likely to have an unfavorable functional outcome (mRS 3–6) at 90 days (89% versus 6%, P < .001).
CONCLUSIONS: MT is effective and safe in patients with mild stroke. Procedural success did not vary among MT techniques in mild stroke. The total number of passes predict END, which suggests a causal pathway that requires further exploration.
ABBREVIATIONS:
- AIS
- acute ischemic stroke
- BMT
- best medical treatment
- DA
- direct aspiration
- END
- early neurologic deterioration
- eTICI
- Expanded Thrombolysis in Cerebral Infarction
- EVT
- endovascular treatment
- IQR
- interquartile range
- LVO
- large-vessel occlusion
- MT
- mechanical thrombectomy
- sICH
- symptomatic intracranial hemorrhage
- SR
- stent retriever
Footnotes
M.A. Möhlenbruch and A. Tessitore contributed equally to this work.
The ASSIST Registry was sponsored and funded by Stryker Neurovascular, Clinicaltrials.gov (No. NCT03845491). Although the sponsor was involved in the design, collection, analysis, interpretation, and fact-checking of information, the content of this article and its ultimate interpretation, along with the decision to submit it for publication, was made independently by the authors.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
- © 2025 by American Journal of Neuroradiology
Log in using your username and password
Log in through your institution




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.