
Abstract
BACKGROUND AND PURPOSE: Some Woven EndoBridge devices present a persistent intradevice opacification at imaging follow-up, described as the Bicêtre Occlusion Scale Score 1 (BOSS 1) phenomenon. The clinical implications remain unknown. We aimed here to analyze the factors influencing this occurrence and to precisely describe the evolution of BOSS 1 with time using conebeam CT.
MATERIALS AND METHODS: We retrospectively analyzed a prospectively maintained Woven EndoBridge database at our tertiary center and included all patients with isolated BOSS 1 and BOSS 1 associated with small neck remnant (BOSS 1 + 2).
RESULTS: Two hundred sixty-seven aneurysms were treated with a Woven EndoBridge device between July 2012 and December 2021. Follow-up with DSA was available for 220 aneurysms (median, 5 months), among which BOSS 1 and 1 + 2 were found in 9.1% (20/220) (95% CI, 5.5%—12.7%). A second DSA follow-up (median, 17 months) was performed in 15 of these 20 aneurysms, which revealed that 40% had evolved to complete Woven EndoBridge occlusion, 33% showed a decreased persistent opacification, and 27% remained stable. BOSS 1 was significantly associated with postoperative antiplatelet medication, a lower aneurysm aspect ratio, and the use of the Woven EndoBridge 17 (P < .05). The average Woven EndoBridge shape modification was less pronounced in the BOSS 1 population (P < .02). None of the BOSS 1 or 1 + 2 aneurysms required retreatment or were associated with hemorrhage occurrence.
CONCLUSIONS: Isolated persistent flow inside the Woven EndoBridge device at follow-up is rare and notably associated with antiplatelet prescription. It seems to present a benign course in most cases.
ABBREVIATIONS:
- BOSS 1
- Bicêtre Occlusion Scale Score 1
- CBCT
- conebeam CT
- FU
- follow-up
- WShM
- WEB shape modification
- WEB
- Woven EndoBridge
The Woven EndoBridge (WEB; MicroVention) has been used in the treatment of wide-neck intracranial ruptured and unruptured aneurysms for >10 years.1⇓-3 Once implanted within the aneurysmal sac, this device induces progressive thrombosis by disrupting the blood flow at the level of the neck. Flow decrease and stagnation of blood then trigger the thrombosis cascade inside the WEB, leading to aneurysm healing on endothelialization of the WEB struts.
In a small proportion of patients, this process appears either inhibited or very much delayed.4,5 Evidence of contrast filling inside the WEB at follow-up (FU) of such patients reflects a persisting blood flow, yet the underlying mechanisms of this incomplete thrombosis remain unclear.
Such isolated persistent intra-WEB opacification is described as Bicêtre Occlusion Scale Score 1 (BOSS 1) (Fig 1).6 While this phenomenon appears in a relatively small number of cases,4,5 its immediate clinical impact or long-term evolution remains undetermined. In the literature, such cases have been referred to as adequate occlusion4⇓-6 or sometimes as an aneurysm remnant.7,8 Our unique systematic use of conebeam CT (CBCT)9 during FU allowed us to conduct a precise analysis of this phenomenon.

A saccular aneurysm of the right ICA terminus was treated with a WEB device (A and D). The 4-month DSA and VasoCT FU demonstrated a persistent intra-WEB opacification ie, BOSS 1 (B and E). The 1-year FU revealed complete occlusion of the aneurysm (F). Illustration of the BOSS 1 phenomenon (C).
MATERIALS AND METHODS
Ethical Statement
The French Ethical Committee for Research in Medical Imaging (CERIM) approved this study (institutional review board No. CRM2101–127). Informed consent was obtained for every patient.
Study Design and Population
We retrospectively analyzed demographic, clinical, and imaging data from patients prospectively included between July 2012 and December 2021 in a prospectively maintained WEB database.
Inclusion criteria were the following: patients with intracranial unruptured or ruptured aneurysms treated with a WEB device and who had at least 1 FU cerebral DSA, including CBCT, with 1 of the 2 following imaging features at first FU: an isolated residual opacification inside the WEB device (BOSS 1) or a small neck remnant + residual opacification inside the WEB device (BOSS 1 + 2).
All patients presenting with an aneurysm remnant + residual opacification inside the WEB device (BOSS 1 + 3) were excluded from the study.
Embolization Procedure and Medication Protocols
Each elective patient scheduled for embolization with the WEB was premedicated with dual antiplatelet therapy,10 for which the most frequently used combination was ticagrelor (90 mg twice daily) and aspirin (160 mg daily) on the day before the intervention. Ruptured aneurysms were not premedicated.
Following the intervention, only in cases of important WEB protrusion or adjuvant stent deployment was antiplatelet therapy prescribed at the operator’s discretion.
DSA FU and Analysis
We systematically used both DSA and CBCT (SmartCT Vaso; Philips Healthcare) as imaging methods to assess the aneurysmal occlusion and intra-WEB opacifications.9 In general, the first follow-up DSA for ruptured aneurysms was performed 3 months after treatment, while for unruptured aneurysms, it was performed 6 months postembolization. Images were analyzed by 2 neuroradiologists, and discrepancies were resolved by discussion and agreement. Angiographic outcome was assessed on the basis of the BOSS scale.
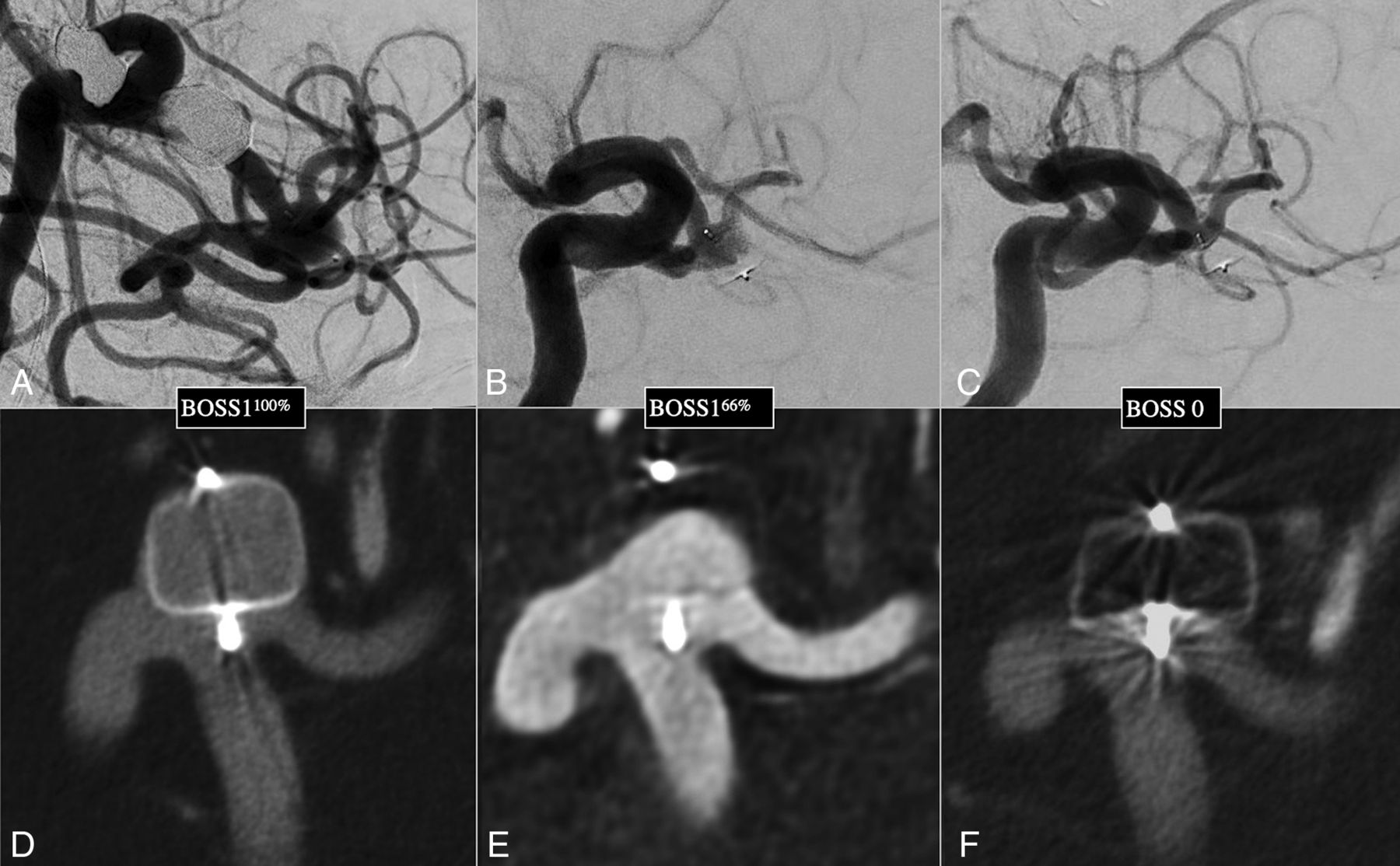
For the purpose of this study, the BOSS 1 category was subdivided into 3 subtypes: BOSS 133%, referring to opacification of 1%–33% of the WEB device; BOSS 166% for 34%–66%; and BOSS 1100% for 67%–100% at FU (Fig 2).

An MCA bifurcation aneurysm was treated with a WEB device. A progressive occlusion was depicted, from BOSS 1100%, opacification of 67%–100% of the WEB volume (A and D), to BOSS 166%, opacification of 33%–66% of the WEB volume (B and E), and then BOSS 0, complete occlusion (C and F).
As previously described,11 WEB shape modification (WShM) was quantitatively defined as a ratio (percentage) and was obtained by standardized measuring of the distance between the proximal and distal WEB markers on cross-sectional images obtained with conebeam CT performed after WEB detachment and again at last FU.
Statistical Analysis
Continuous variables were reported as the mean ± standard deviation (SD) if normally distributed, or as the median (interquartile range), while categoric variables were expressed as a frequency (%). Confidence intervals were based on the Wald statistic. As appropriate, a χ2 or Fisher exact test was used to evaluate qualitative factors, and a Student t test or Wilcoxon U test to assess quantitative variables. P values < .05 were considered statically significant. All statistical analyses were performed using R 3.6.1 for Windows (https://cran.r-project.org/bin/windows/base/old/3.6.1/).
RESULTS
BOSS 1 Assessment
A total of 267 aneurysms were treated with a WEB device between July 2012 and December 2021 (Table). A cerebral DSA FU was available in 220 of these cases (82%), 27.4% of which were ruptured aneurysms.
Characteristics of patients, aneurysms, and treatments according to the initial angiographic follow-upa
The BOSS 1 phenomenon was found in 20 cases (9.1%; 95% CI, 5.5%–12.7%) at first DSA FU (median, 5 months; interquartile range, 3–6 months). These were subdivided into BOSS 133% for 15%, BOSS 166% for 25%, and BOSS 1100% for 60% (Fig 3).

Evolution of the degrees of WEB volume opacifications (in percentages) for all BOSS 1 aneurysms at early FU (median, 5 months) and at last follow-up (median, 17 months).
More than 1 DSA was available for 75% of cases presenting with the BOSS 1 phenomenon (15/20). At the last FU (median, 16.9 months; interquartile range, 7–20 months), 40% of these BOSS 1 cases had evolved to complete WEB occlusion; BOSS 1 persisted in the remaining 60% (9/15), though the level of intradevice opacification had decreased in 60% (5/9) of these compared with the initial FU. At the last FU, persistent opacifications were subdivided into BOSS 133% for 44%, BOSS 166% for 33%, and BOSS 1100% for 22%.
Factors Associated with BOSS 1 Persistence
Fifteen of the 20 patients (75%) presenting with the BOSS 1 phenomenon received an antiplatelet medication for at least 1 month after the intervention (11 single and 4 dual antiplatelet therapies). BOSS 1 was significantly associated with postoperative antiplatelet medication (OR = 3.52; 95% CI, 1.31–11.16; P < .02).
BOSS 1 phenomenon was also associated with use of the WEB 17 generation (OR = 3.33; 95% CI, 1.07–14.59; P < .05) and with the aneurysm aspect ratio (OR = 0.23; 95% CI, 0.06–0.75; P < .02).
The average WShM of 30% (95 CI, 9%–36%) at last FU was lower in the BOSS 1 and 1 + 2 scores compared with the 39% (95 CI, 21%–52%) in the other scores (P < .02).
None of the aneurysms presenting with BOSS 1 or 1 + 2 required retreatment, and no hemorrhage occurred during the FU period.
DISCUSSION
Here we have highlighted the unique capacity of VasoCT to analyze the BOSS 1 phenomenon; we believe it should be used systematically as the criterion standard technique to assess WEB treatment success.
Persistent filling of the WEB device cannot be assessed using MR imaging,12 and the assessment is impossible in most cases with CT.13 Differentiating between aneurysm remnants and BOSS 1 is sometimes disputable, even using projection imaging (DSA), yet this distinction is fundamental to allow the correct management. Indeed, a retreatment should probably be considered in cases in which blood flow is depicted in the sac around the WEB. CBCT also allowed a precise quantitative assessment of intradevice opacification.9
Our series shows a relatively rare occurrence of the BOSS 1 phenomenon at early follow-up, with a rate of 9.1% (95% CI, 5.5%–12.7%). Previous smaller series have reported 6.3%–16% BOSS 1 rates at midterm FU.4,5
Favorable Angiographic Evolution of BOSS 1
We observed a reduction in persistent opacification inside the WEB device between the first and last FU in 73% of cases, demonstrating a progressive thrombosis with time.
BOSS 1 remained at last FU in 60% of cases, but no patient experienced a worsening of angiographic status (ie, no evolution to BOSS 3) or aneurysmal rupture, and no BOSS 1 or 1 + 2 aneurysms required retreatment during the FU period. This result would suggest a benign course for this angiographic phenomenon.
Impact of Antiplatelet Therapy on BOSS 1
While the use of antiplatelet medication after WEB implantation has already been hypothesized to favor persistent opacification,7 here we have provided the first evidence of prolonged antiplatelet therapy (>1 week after the intervention) being significantly associated with an increased risk of BOSS 1 aneurysms at FU (OR = 3.52; 95% CI, 1.31–11.16). We believe that antiplatelet drugs can be responsible for delayed aneurysm thrombosis and neck endothelialization.
In our study, 75% of patients with BOSS 1 received an antiplatelet medication for at least 1 month after WEB placement (versus 45% in the control group). Concordantly, Nguyen et al4 reported dual antiplatelet therapy intake for at least 1 month postintervention in 7 of 8 patients with BOSS 1, and Nawka et al5 reported antiplatelet therapy for at least 6 weeks in all patients with BOSS 1.
With the oversizing paradigm,11 moderate WEB protrusions in the parent artery are more common, and operators tended to prescribe postoperative antiplatelet medications in those situations. Operators should, however, also consider the potential delay in aneurysmal thrombosis and endothelial repair caused by the antiplatelet therapy.14,15
Other Predictive Factors of BOSS 1
Web 17 Generation.
The latest generation of the WEB device (WEB 17) can be delivered through 0.017-inch microcatheters.16 The smaller-sized devices were achieved by reducing the number of wires used in braiding. While this change in design does not seem to modify the “adequate occlusion” rates,17 the higher porosity at the level of the neck could be responsible for higher BOSS 1 rates. In our series, this last generation of WEB was significantly associated with BOSS 1 occurrence, and 85% of BOSS 1 corresponded to WEB 17 devices.
Aspect Ratio.
The aneurysm dimensions and conformation play an important role in BOSS 1 occurrence. In our study, lower aspect ratio aneurysms (ie, shallow aneurysms) were significantly associated with BOSS 1 at FU. We hypothesized that these aneurysms were more likely to have a delayed intra-aneurysm thrombosis due to the larger surface area of the WEB, requiring endothelial cell covering in the neck region, similar to that observed with the negative impact of larger neck size on the angiographic outcomes of flow-diverter stents.18
Ruptured Aneurysms.
We found no significant differences in terms of BOSS 1 occurrence between ruptured and unruptured aneurysms.19
WShM and BOSS 1
The mechanisms behind WShM are not well-understood, though clot retraction is suspected to be a major cause,20 with a water hammer effect potentially acting as a minor associated cofactor.21
The thrombosis process inside the WEB is initially induced by flow disruption. After endothelialization of the WEB surface, the aneurysm is completely excluded from the circulation, and progressive collagen deposition and subsequent contraction occur.22
We observed a significantly lower WShM among the BOSS 1 population compared with other categories, supporting the notion of an impact of clot formation on WEB retraction; the lower intra-WEB thrombus volumes could be hypothesized to lead to less retraction.
Limitations
We acknowledge some limitations in our study, the first being its retrospective and monocentric nature; however, we believe that our unique systematic use of VasoCT was mandatory to conduct the precise analysis presented. Second, the number of patients could be viewed as limited; however, we present here one of the largest series of patients presenting with the BOSS 1 rare phenomenon. Finally, the lack of very long-term FU prevents us from drawing any definite conclusions on the outcome of all patients with BOSS 1; however, our data provide evidence in favor of the progressive evolution toward occlusion.
CONCLUSIONS
Isolated persistent flow inside the WEB device at follow-up is rare and notably associated with antiplatelet prescription; it seems to present a benign course in most cases.
Footnotes
J. Caroff and S.D. Popescu contributed equally to this work.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received October 26, 2022.
- Accepted after revision January 3, 2023.
- © 2023 by American Journal of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Neck apposition is a key factor for aneurysm occlusion after Woven EndoBridge device embolization
- The Artisse intrasaccular device for the treatment of cerebral aneurysms: initial experience from three Austrian neurovascular centers
- WEB shape modifications: angiography-histopathology correlations in rabbits
- WEB shape modifications: angiography-histopathology correlations in rabbits