
Abstract
BACKGROUND AND PURPOSE: The Woven EndoBridge (WEB) system has established itself as a safe and effective option for managing wide-neck bifurcation aneurysms. Addressing aneurysms with a greater height than width using conventional WEB-sizing methods has proved ineffective due to the inherent configuration of the devices. To overcome this limitation, we propose an intuitive approach that involves swapping the width and height dimensions of the aneurysm to determine the appropriate WEB size.
MATERIALS AND METHODS: A retrospective analysis was conducted on patients undergoing WEB embolization at a single neuroscience center from March 2013 to February 2023.
RESULTS: Twenty-five eligible aneurysms were identified, with the height dimension exceeding the width by an average of 2.33 mm (ranging from 1.4 to 4.5 mm). Of these, 20 cases adhered to the recommended sizing technique, resulting in a 100% success rate of adequate occlusion (14/20 complete occlusion, 6/20 proximal recess filling). In contrast, the outcomes for the remaining 5 cases that did not follow the proposed sizing method were less favorable (P < .05). Among these, 4 cases treated with undersized WEBs showed neck remnants during follow-up, and 1 patient who received an oversized WEB required device replacement during the same procedure.
CONCLUSIONS: The simple sizing method we proposed for treating taller-than-wide aneurysms has demonstrated promising results, allowing the WEB system to address twice the original size range of treatable aneurysms. Further research with a larger sample size is recommended.
ABBREVIATIONS:
- SL
- single-layer
- SLS
- single-layer sphere
- WEB
- Woven EndoBridge
- WOS
- WEB Occlusion Scale
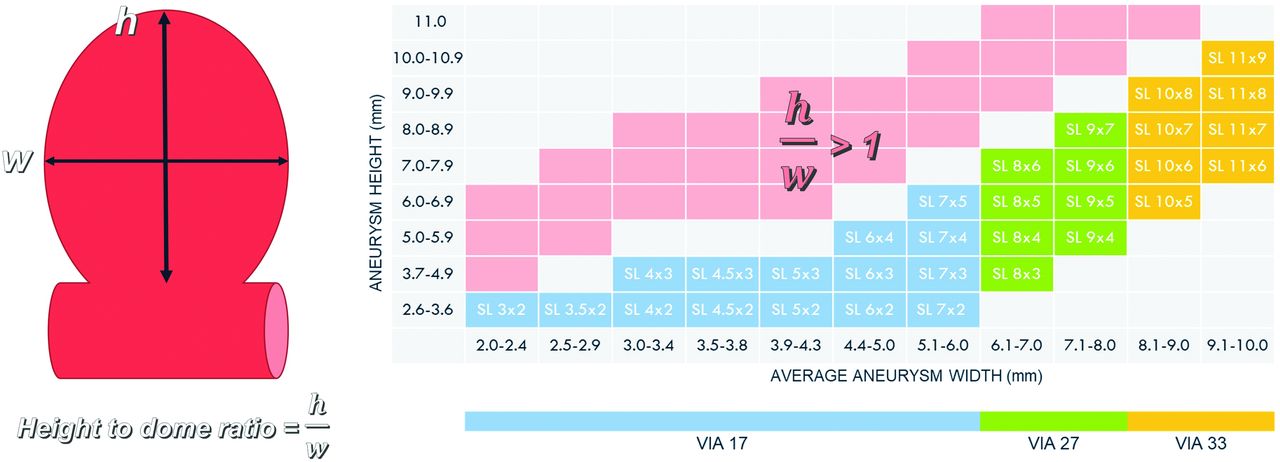
The Woven EndoBridge (WEB; MicroVention) device has emerged as a reliable and effective solution for the treatment of wide-neck intracranial bifurcation aneurysms.1 Accurate device sizing is crucial for achieving favorable angiographic outcomes.2 However, traditional sizing methods like the +1/–1 rule or referencing the manufacturer’s sizing chart may not be able to deliver the necessary height extension to achieve an optimal fit for aneurysms characterized by a high height-to-dome ratio (Fig 1). To address this issue, we introduce an intuitive approach that prompts the device to undergo considerable lateral compression, leading to a substantial increase in its vertical extension. The main purpose of this article was to provide an in-depth exploration of the proposed sizing strategy and highlight its potential in enhancing the clinical utility of the WEB system.

The manufacturer’s sizing chart for the WEB device does not cover aneurysms with a height-to-dome ratio of >1. Our proposed approach expands the original range of treatable aneurysms to include those shown in the red zone, effectively doubling the spectrum of aneurysms without the need for additional fixed-sized WEB devices.
MATERIALS AND METHODS
We conducted a retrospective review of patients who underwent WEB embolization at our institution from March 2013 to February 2023. We define an aneurysm as taller-than-wide when its height-to-dome ratio surpasses 1, enabling it to qualify for inclusion in the analysis.
Data collection included patient demographics, aneurysm characteristics, device parameters, and angiographic outcomes. Surveillance imaging protocols for individuals who undergo WEB embolization include DSA and MRA at 6-month and 2-year intervals. However, starting from 2020, due to the coronavirus 2019 pandemic and in adherence to local infection-control policies, all cases are exclusively followed up using MRA alone to minimize the risk of viral transmission.
Technical Details
After acquiring both 2D and 3D angiographic images, the target aneurysm is evaluated from 2 orthogonal projections, with one of them typically being the “down-the-barrel” view. After excluding redundant spaces such as daughter sacs and side blebs, the appropriate WEB size can be determined by strategically swapping the height and width dimensions of the aneurysm (Fig 2). For an aneurysm that measures w millimeters in width and h millimeters in height, the recommended WEB size would be h × w mm.

Diagram depicting the proposed sizing strategy for aneurysms with a high height-to-dome ratio. The appropriate WEB size is determined by strategically swapping the height and width dimensions of the aneurysm. For an aneurysm measuring w × h, it is advisable to use a h × w WEB. When fully deployed, the device undergoes significant lateral compression, leading to a substantial increase in its vertical extension, which helps to achieve an optimal fit for the aneurysm.
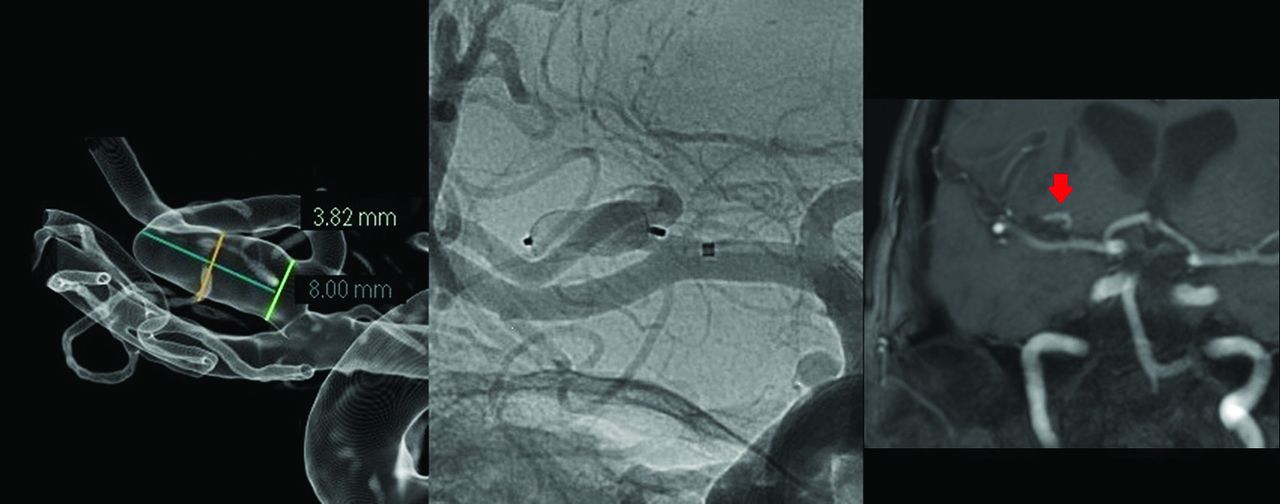
Figure 3 demonstrates a practical application of the suggested sizing technique. A highly elongated cylindrical aneurysm on the right MCA, measuring 3.82 mm in width and 8 mm in height, was under consideration for WEB embolization to safeguard the adjacent temporal branch. On the basis of the size measurements, an 8 × 4 mm WEB single-layer (SL) was selected for the procedure. The device underwent substantial lateral compression, resulting in a reduction of its width from 8 to 4 mm and a similar increase in its height from 4 to approximately 8 mm. This dynamic transformation led to effective occlusion of the aneurysm, which remained stable during subsequent follow-ups.

An elective embolization was performed on a right cylindrical MCA aneurysm, with measurements indicating a maximum width of 3.82 mm and a height of 8 mm. An 8 × 4 mm WEB SL device was successfully deployed without impeding the adjacent temporal branch. As a result of intense lateral compression, the base of the SL device assumed a cup-shaped configuration, leaving a small “dog ear” at the neck of the aneurysm. At the 6-month follow-up, the aneurysm continued to show satisfactory results (red arrow).
Sizing of Noncylindrical Aneurysms
The process of choosing the appropriate WEB size for standard cylindrical aneurysms is often straightforward because their shape closely matches that of the recommended device. When dealing with noncylindrical aneurysms, interobserver disparity in image interpretation and aneurysm measurement can result in inconsistent results. To improve sizing consistency, we recommend adding a minor adjustment that involves targeting the maximum height and width of the aneurysm.
Because the actual volume of a noncylindrical aneurysm is inherently smaller in comparison with its cylindrical counterpart with equivalent maximum height and width, it becomes necessary to downsize the selected WEB device by reducing the device height while keeping its width constant. In most cases, a 1-mm reduction in height is adequate to prevent oversizing the WEB implant. However, aneurysms that significantly deviate from the standard cylindrical model may require a 2-mm reduction. In cases in which lowering the device height is not feasible, the width of the device can be reduced as a last resort to decrease the overall volume of the WEB.
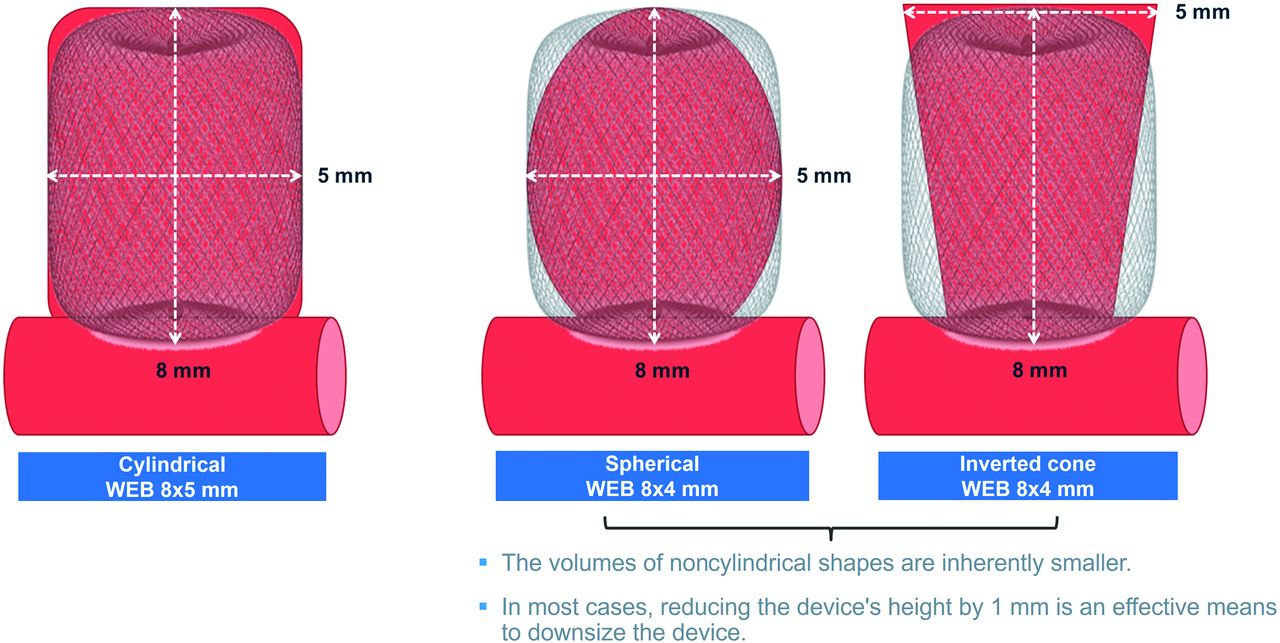
Figure 4 provides an example to demonstrate the downsizing procedure. In this visual representation, all 3 aneurysms share the same maximum width and height dimensions of 5 × 8 mm, suggesting that they should be treated with an 8 × 5 mm WEB device according to the recommended sizing method. However, it becomes apparent that the volumes of the 2 noncylindrical aneurysms are, in fact, smaller and would not provide sufficient room for an 8 × 5 mm device. The WEB device can be downsized by reducing the height by 1 mm, making an 8 × 4 mm device a more appropriate choice for these aneurysms to address this issue.

When one deals with aneurysms of noncylindrical shapes, interobserver discrepancies in image interpretation and aneurysm measurement can result in inconsistent results. Aneurysms with noncylindrical shapes generally have smaller actual volumes than their cylindrical counterparts with the same maximum width and height. To ensure an adequate fit within the aneurysms, one must downsize the WEB device by reducing the device height. In this visual representation, all 3 aneurysms share the same maximum width and height dimensions of 5 × 8 mm, suggesting that they should be treated with an 8 × 5 mm WEB device according to the recommended sizing method. However, the actual volumes of the 2 noncylindrical aneurysms are smaller and would not provide sufficient room for an 8 × 5 mm device. The WEB device can be downsized by reducing the height by 1 mm, making an 8 × 4 mm device a more appropriate choice for these aneurysms to address this issue.
With the predetermined range of commercially available WEBs, size adjustments for the device are typically limited to 1-mm increments. Given the general ease of reaching a consensus on the maximum width and height of the aneurysm, the downsizing approach effectively minimizes interobserver variation in size selection to just 1 or 2 options (Fig 5).

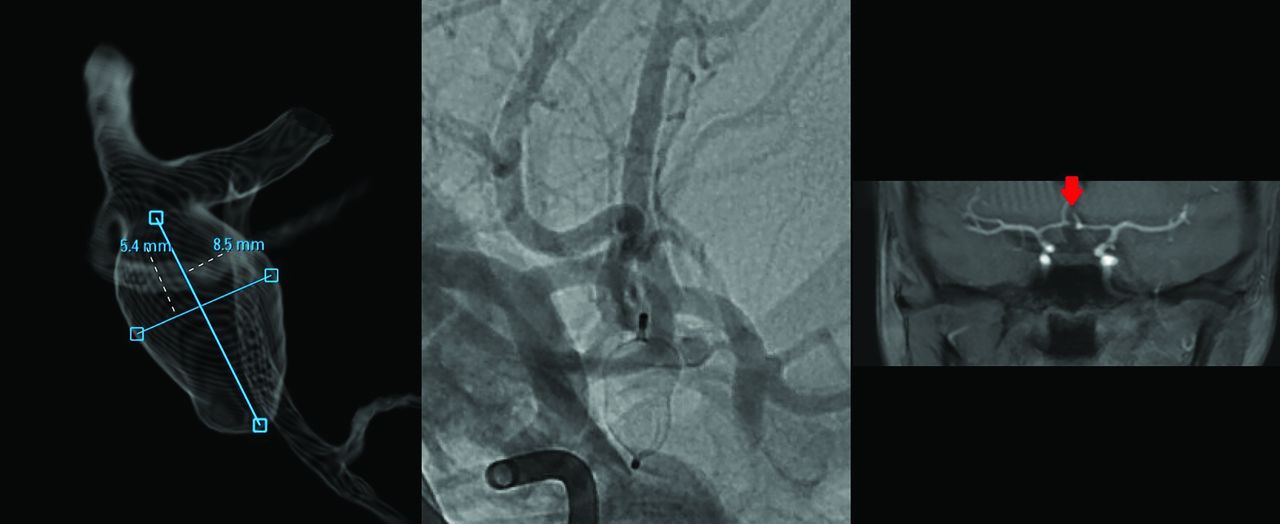
WEB embolization of an acute anterior communicating artery aneurysm, characterized by a maximum width of 5.4 mm and a height of 8.5 mm. A strategic downsizing was performed due to the noncylindrical shape of the aneurysm. Instead of using an 8 × 5 mm device, an 8 × 4 mm WEB SL was selected for the procedure. A follow-up at 6 months showed that the aneurysm remained fully occluded (red arrow).
RESULTS
A total of 25 cases were identified of 315 WEB embolization procedures during a 10-year period. The average age of the patients was 61.8 (SD, 13) years, with 68% being women. Among the cases, 76% presented with acute SAH, while the remaining cases were elective procedures.
The heights of treated aneurysms surpassed their widths by a range of 1.4 to 4.5 mm, with an average difference of 2.33 mm. Approximately 44% of the aneurysms were located at the anterior communicating artery; 40% were found at the MCA bifurcation or M1 segment; 8%, at the ophthalmic segment of the ICA; 4%, at the pericallosal artery; and 4%, at the anterior choroidal artery. The average aneurysm width was 5.04 mm (range, 3.32–8.20 mm), and the average aneurysm height was 7.38 mm (range, 5.24–11.39 mm). The WEB devices underwent an average lateral compression of 2.03 mm (range, 0.03–4.00 mm) following full deployment. All patients underwent surveillance studies at 6 months, and imaging follow-up at the 2-year interval was available for 60% of the cases.
Angiographic Occlusion Rates
To evaluate the effectiveness of the proposed sizing method, we divided the patient cohort into 2 categories: group A consisted of individuals whose devices adhered to the recommended sizing technique, whereas group B included those whose devices deviated from it (Table and Online Supplemental Data).
In all 20 cases within group A, a single WEB device was effectively deployed without the need for subsequent replacement arising from sizing errors. Angiographic surveillance shows that 70% (14/20) of the aneurysms exhibited complete occlusion (WEB Occlusion Scale [WOS], grade A), while the remaining 30% (6/20) had proximal recess filling (grade B). No incidence of persistent neck remnant (grade C) or aneurysm remnant (grade D) was observed.
The remaining 5 patients in group B underwent treatment with WEB devices that were selected without adhering to the recommended sizing strategy. These cases predominantly occurred during the initial phase of introducing the WEB system, preceding widespread acceptance of the recommended sizing strategy in our department. Among these patients, 4 were treated with WEB devices that were smaller than what was advised, resulting in aneurysm neck recurrence (grade C) in all 4 cases and 1 patient undergoing additional treatment with a flow-diverting stent. The last patient in this group received a WEB device larger than necessary, which was replaced with a smaller device during the same procedure, and subsequent follow-up examinations demonstrated complete aneurysm occlusion at the 2-year interval.
DISCUSSION
A recently published meta-analysis revealed that an aspect ratio of ≥1.5 increased the risk of rupture, independent of the aneurysm size.3 While these aneurysms can often be treated with coil embolization alone, a subset of cases with a neck size exceeding 4 mm may still pose significant challenges.4 Designed to function as a stand-alone device, the WEB system provides a safe and effective treatment option without the need for additional assistance devices. The WEB is typically oversized by 1–2 mm from the average diameter of the aneurysm in 2 perpendicular planes. To accommodate the vertical extension resulting from lateral compression, its height is reduced by 1–2 mm in comparison with the aneurysm height.5 However, due to the inherent wider-than-tall design of WEB devices, this sizing approach often proves ineffective for addressing elongated aneurysms. For example, adjusting the width and height of the device by 1–2 mm for a 5 × 8 mm aneurysm would result in the choice of a 6 × 7 or 7 × 6 mm SL device, both of which are commercially unavailable.
The strategy we put forward offers a simple approach that can be readily implemented in everyday practice. Through the interchange of width and height dimensions, all patients in the compliant group achieved adequate aneurysm occlusion during subsequent surveillance. In contrast, those who deviated from the proposed sizing method experienced significantly less favorable angiographic outcomes (P < .05). Furthermore, a substantial degree of lateral compression greatly enhances the resistance of the device to delayed compaction in the compliant group, possibly contributing to the high occlusion rate observed in surveillance imaging.6
The Clinical Assessment of WEB device in Ruptured Aneurysms (CLARYS) trial demonstrates promising outcomes in the application of the WEB for treating ruptured aneurysms, with protection against early and mid-late rebleeds.7 Seventy-six percent of patients in our small series presented with ruptured aneurysms. On the basis of our limited experience, there appears to be no significant increase in the risk of aneurysmal wall injury attributed to elevated wall tension, potentially underscoring the high compliance of the WEB system.
Clinical Applications
Conventional sizing methods such as the +1/–1 rule and the official sizing chart restrict each individual device to a narrow range of treatable aneurysms. As a result, expanding the use of the WEB to treat a broader spectrum of aneurysms will require adding new device sizes, which may increase the complexity in inventory management. The sizing method we proposed has the potential to double the original range of treatable aneurysms, all without the need for additional fixed-sized WEB implants (Fig 1). The concept of enhancing the clinical versatility of the WEB device through lateral-compression manipulation is relatively underexplored and merits further investigation.
Impacts of Extreme Lateral Compression
In instances in which the height of an aneurysm markedly surpasses its width, an extreme level of lateral compression is unavoidable on the full deployment. This can cause a significant morphologic transformation of the WEB device, which may impact its intended deployment.
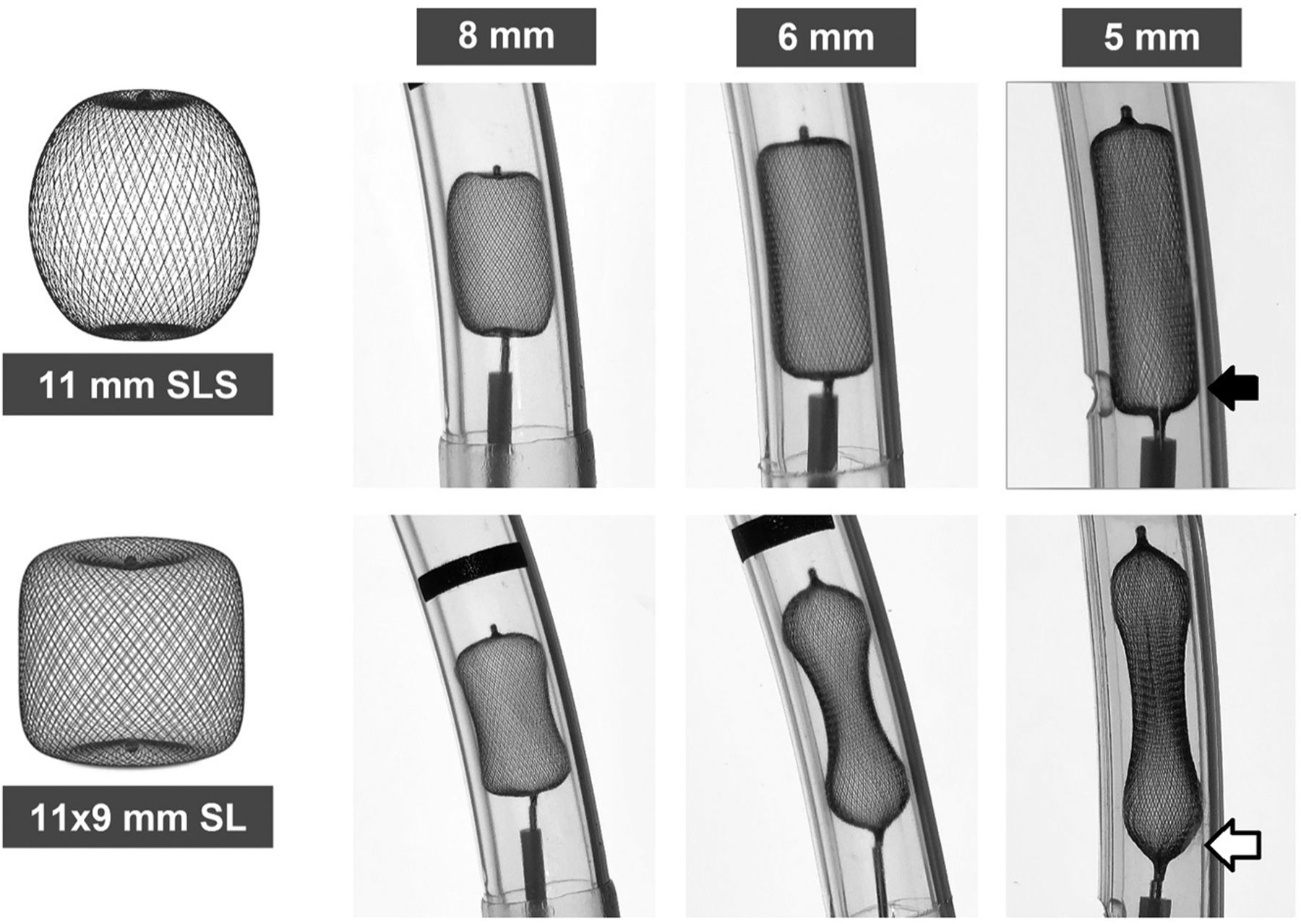
In the case of the WEB SL, the corners of the device typically generate the greatest radial forces, while the waist is more susceptible to external compression. When subjected to extreme lateral compression, the WEB SL device tends to assume a characteristic “hourglass” shape. In contrast, the WEB single-layer sphere (SLS) with its initially broader waist diameter is more likely to take on a cylindrical configuration (Fig 6).

When subjected to extreme, lateral compression, the WEB SL device tends to assume a characteristic hourglass shape, while the WEB SLS is more likely to take on a cylindrical configuration. As a result, the base of the WEB SL device frequently adopts a concave, cup-shaped appearance (open arrow), whereas the WEB SLS device tends to create a flat base (solid arrow). This inversion of configurations can potentially affect the neck coverage during the treatment of the aneurysm.
Consequently, the base of the WEB SL device, which covers the aneurysm neck, frequently adopts a concave, cup-shaped appearance, while the proximal recess of the WEB SLS device tends to form a flat surface. Under extreme lateral compression, the 2 models essentially switch roles to accommodate aneurysm configurations that deviate from their originally intended targets. This role reversal can potentially affect the neck coverage during the treatment of the aneurysm (Fig 3). It is, therefore, important to anticipate the impact of role reversal on the performance of the device.
Study Limitations
There are several limitations to our study. Due to the limited sample size, inherent variations (such as ruptured status, WEB models, and larger device/aneurysms) between the 2 groups could influence the statistical difference in treatment outcomes.8 Its retrospective design may introduce inherent biases associated with the use of historical data. Additionally, being conducted at a single neuroscience center may limit the applicability of the results to wider populations.
Despite recent progress in neurovascular device manufacturing, MR imaging of a WEB device remains difficult due to a combination of magnetic susceptibility artifacts and the Faraday cage effect. The low sensitivity of 3D TOF-MRA for the detection of aneurysm remnants suggests that DSA remains the criterion standard for follow-up.9 The use of site interpretation rather than core laboratory assessment of angiographic outcomes may render the result susceptible to observer bias.
Further illustrative cases are available in the Online Supplemental Data, including an irregularly-shaped aneurysm a noncompliant case, and an atypical location.
CONCLUSIONS
Our proposed approach for sizing WEB devices to address taller-than-wide aneurysms has shown promising results. The intuitive strategy, which involves the interchange of width and height dimensions of the aneurysm, presents a simple and practical solution to the limitations of conventional sizing methods. Further investigation with a larger sample size is recommended to evaluate the applicability of this sizing approach across diverse aneurysm configurations.
| Group A | Group B | P Value | |
|---|---|---|---|
| Patient demographics | |||
| No. (total =25) | 20 | 5 | |
| Age (mean) (yr) | 63.8 (SD, 11.2) | 58.6 (SD, 14.5) | |
| Sex (female/male) | 13:7 (65.0%) | 4:1 (80.0%) | .642 |
| Rupture status | .289 | ||
| Acute SAH | 14 (70%) | 5 (100%) | |
| Elective | 6 (30%) | ||
| Location of aneurysm | |||
| MCA | 7 (35%) | 3 (60%) | |
| AcomA | 11 (55%) | ||
| Ophthalmic ICA | 1 (5%) | 1 (20%) | |
| Pericallosal | 1 (20%) | ||
| Anterior choroidal | 1 (5%) | ||
| Morphology of aneurysm | |||
| Cylindrical | 6 (30%) | ||
| Teardrop | 1 (5%) | 1 (20%) | |
| Spindle | 2 (10%) | ||
| Irregular | 11 (55%) | 4 (80%) | |
| Aneurysm dimensions (mean, range) | |||
| Width | 4.95 mm (3.32–8.40 mm) | 5.40 mm (3.55–7.73 mm) | |
| Height | 7.11 mm (5.24–10.60 mm) | 8.44 mm (6.60–11.39 mm) | |
| Neck | 3.70 mm (2.36–6.00 mm) | 3.81 mm (2.36–4.70 mm) | |
| Degree of lateral compression | 2.05 mm (1.4–4.0 mm) | 2.00 mm (0.03–3.27 mm) | |
| 2-Year imaging follow-up | 10 (50%) | 5 (100%) | .061 |
| Occlusion rate | .001 (<.05) | ||
| WOS grade A | 14 (70%) | 1 (20%)a | |
| WOS grade B | 6 (30%) | ||
| WOS grade C | 4 (80%) | ||
| Operative procedure | |||
| WEB sizes (width) | .822 | ||
| 3–7 mm | 14 (70%) | 3 (60%) | |
| 8–9 mm | 4 (20%) | 1 (20%) | |
| 10–11 mm | 2 (10%) | 1 (20%) | |
| WEB models | .012 (<.05) | ||
| SL/SLS | 18 (90%) | 2 (40%) | |
| SL/SLS 17 | 2 (10%) | 3 (60%) |
Note:—AcomA indicates anterior communicating artery.
↵a Successful replacement of an oversized WEB device conducted during the same procedure resulted in complete angiographic occlusion on subsequent follow-up.
Comparison of patient demographics and details of operative procedures between group A, which adhered to the proposed sizing method, and group B, which did not
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received November 21, 2023.
- Accepted after revision January 16, 2024.
- © 2024 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.