
Abstract
BACKGROUND AND PURPOSE: Spinal segment variants are highly prevalent and can potentially lead to incorrect spinal enumeration and, consequently, interventions or surgeries at the wrong vertebral levels. Our aim was to assess the prevalence of spinal segment variants and to study the potential association among these variants in a population without histories of spine symptoms.
MATERIALS AND METHODS: Consecutive computed tomography exams of 450 young adults originally evaluated for non-spinal conditions and without a history of spinal diseases from a single institution. In addition to using descriptive statistics for reporting frequencies of spinal segment variants, the association between these variants was studied by calculating odds ratios and their 95% confidence interval. Consecutive CT exams were evaluated to determine the total number of presacral segments, presence of cervical rib, thoracolumbar transitional vertebra, iliolumbar ligament, and lumbosacral transitional vertebra.
RESULTS: The spinal segment distribution variants (an atypical number of presacral segments or an atypical distribution of thoracolumbar vertebrae), cervical rib, thoracolumbar transitional vertebra, and lumbosacral transitional vertebra were reported in 23.8%, 4.2%, 15.3%, and 26.4% of cases in our study population. The presence of a cervical rib or a thoracolumbar transitional vertebra was associated with concurrent lumbosacral transitional vertebra (OR = 3.28; 95% CI, 1.29–8.47 and 1.87; 95% CI, 1.08–3.20, respectively). The inability to visualize the iliolumbar ligament was also associated with the presence of cervical ribs (OR = 3.06; 95% CI, 1.18–7.80).
CONCLUSIONS: In a population of asymptomatic young adults, spinal segment variants are both highly prevalent with a high rate of coexistence. When a spinal segment variant (eg, transitional vertebra) is diagnosed, additional imaging might be considered for accurate spine enumeration before interventions or operations.
ABBREVIATIONS:
- ILL
- iliolumbar ligament
- LSTV
- lumbosacral transitional vertebra
- TLTV
- thoracolumbar transitional vertebra
Spinal segment variants can potentially lead to incorrect identification of vertebral levels and, subsequently, cause wrong-level interventions or operations.1,2 For instance, selective nerve root blocks require administering epidural spinal injections at specific vertebral levels, which can be confounded by spinal segment distribution variants or the presence of a transitional vertebra.
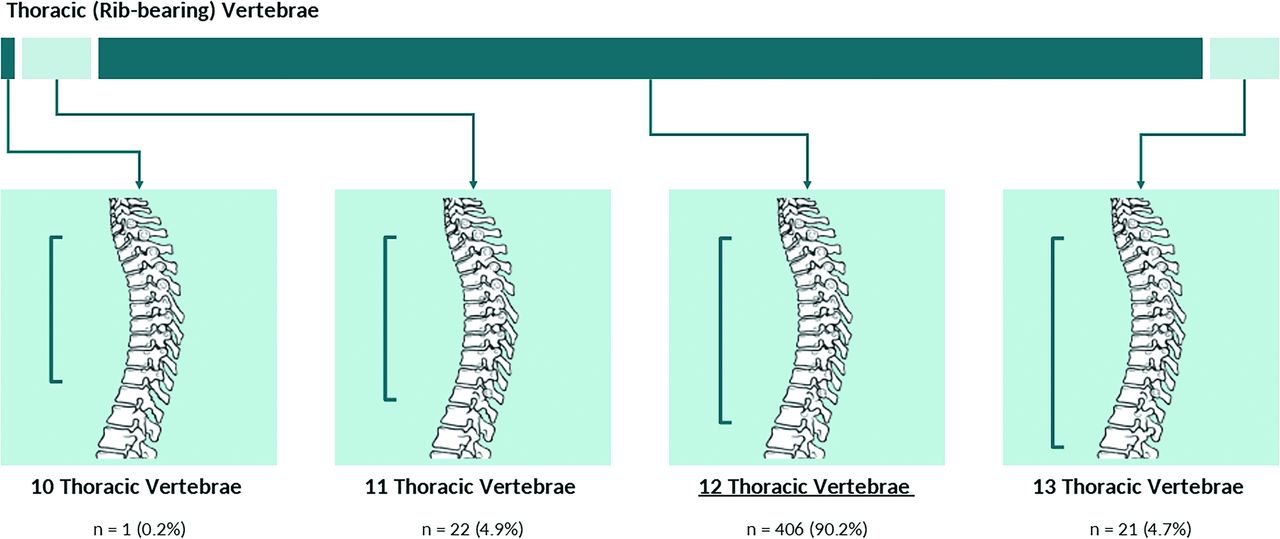
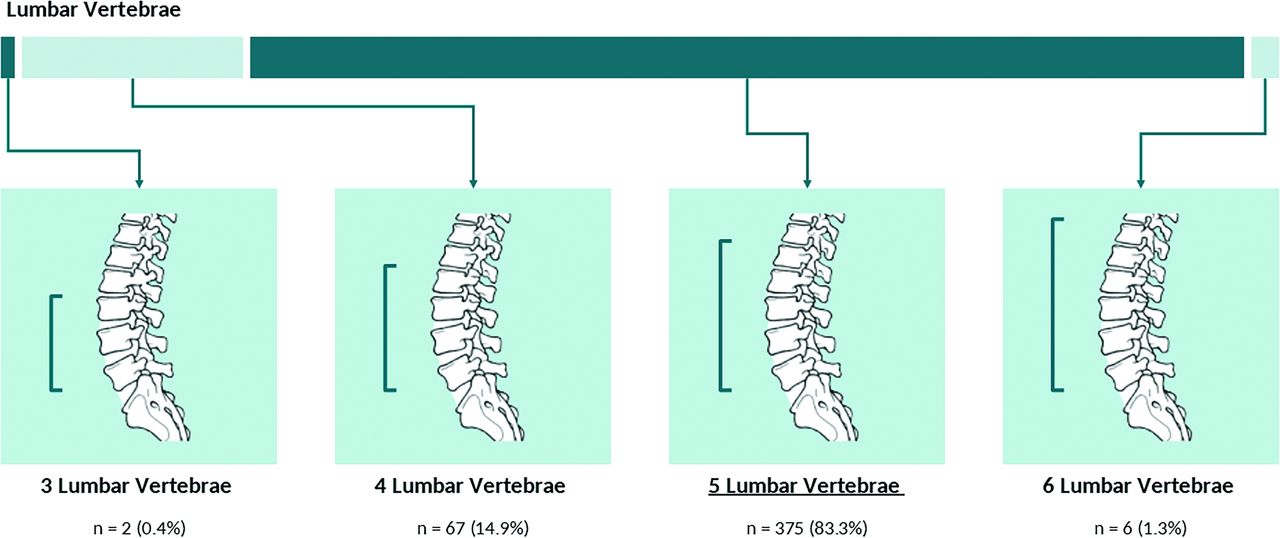
The most prevalent number of presacral segments in the vertebrae is the 24 presacral segments with 7 (non-rib-bearing) cervical, 12 (rib-bearing) thoracic, and 5 (non-rib-bearing) lumbar vertebrae. However, other spinal segment distribution variants with an atypical number of presacral segments (23 or 25 segments) or with atypical distribution of the thoracolumbar vertebrae (11 or 13 thoracic and 4 or 6 lumbar vertebrae) are also common. Other frequently encountered spinal segment variants with relevant clinical implications include cervical ribs and transitional vertebrae, among others.3
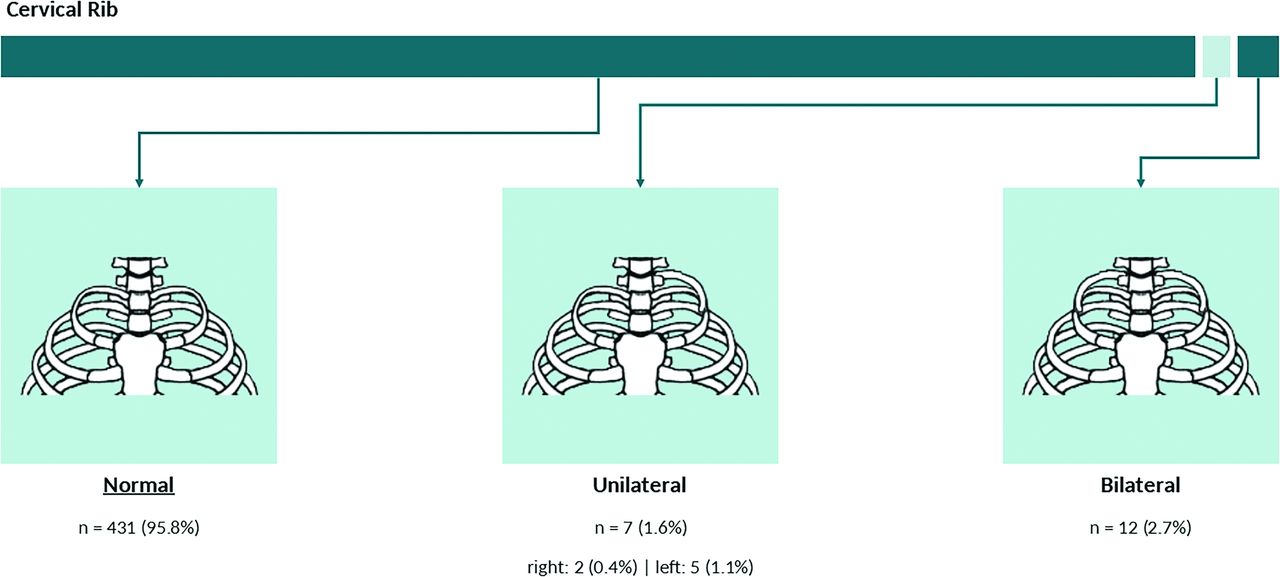
The cervical rib is diagnosed when an additional rib originates from the last cervical segment (ie, the seventh cervical segment or C7).3 The cervical rib may vary in length and may have a fibrous connection to the first rib; however, it can potentially tighten the space between the first rib and the anterior scalene muscle and impinge the nerves and arteries that pass through this space to the upper extremity.4 Therefore, its presence may cause pain, paresthesia, and muscle weakness in the upper extremity on the affected side.
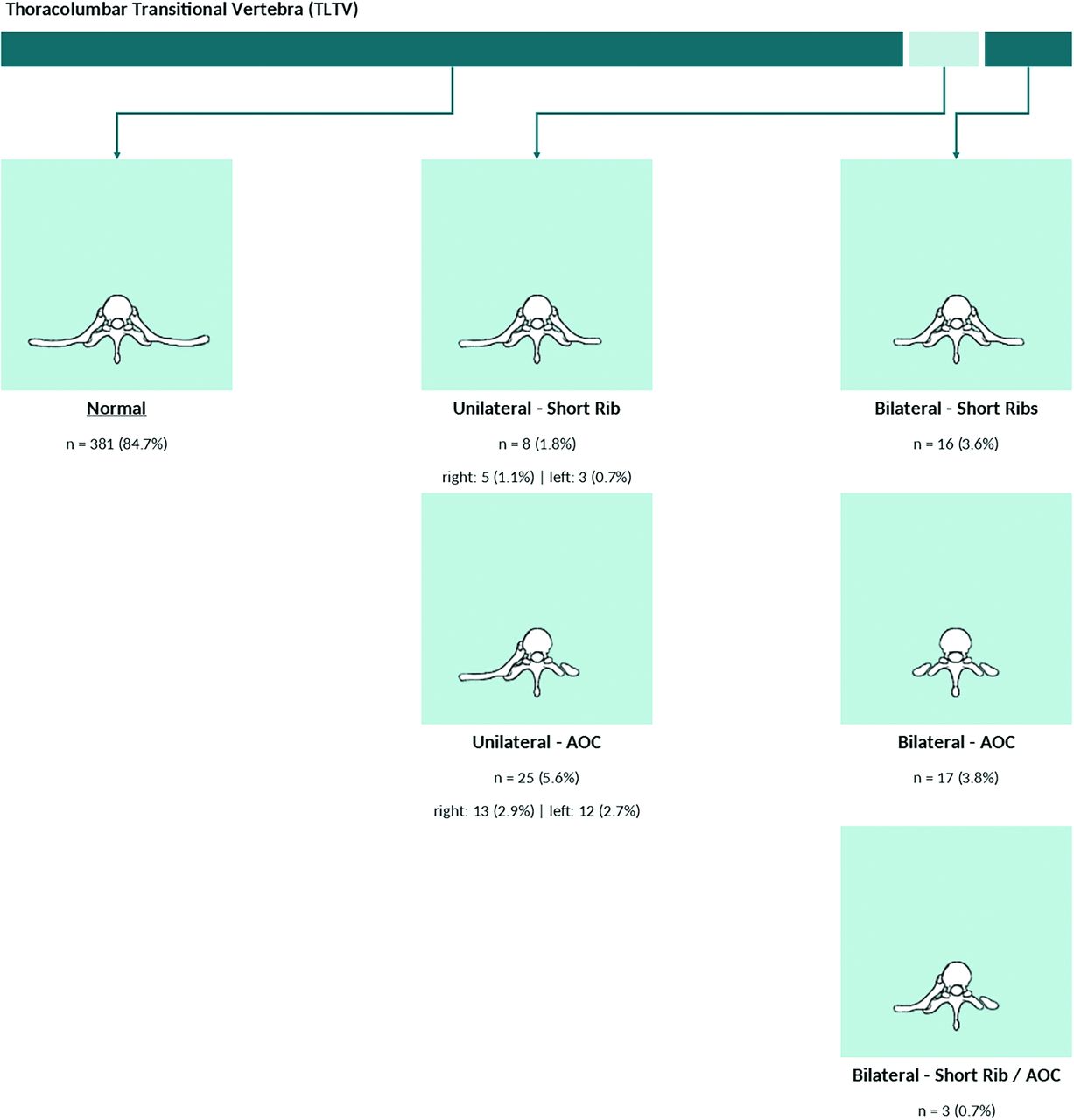
Transitional vertebrae are diagnosed when the segment at the junction of the thoracic, lumbar, or sacral vertebrae has partial characteristics from both upper and lower vertebrae.3 The thoracolumbar transitional vertebra (TLTV), for instance, is diagnosed when the last thoracic (rib-bearing) segment shows features of a non-rib-bearing segment and has hypoplastic ribs.5 Moreover, the lumbosacral transitional vertebra (LSTV) is diagnosed when either the last lumbar segment shows a transition toward the sacral vertebrae (ie, sacralization) or the first sacral segment shows features of the lumbar vertebrae (ie, lumbarization).6 The symptoms associated with TLTV or LSTV are not well-documented; however, the presence of these transitional vertebrae is associated with other spinal segment variants.7 Thus, it is suggested that when a transitional vertebra is diagnosed, additional imaging should be considered to confirm spine enumeration before interventions or operations.8
The prevalence of the spinal segment variants in patients with upper-extremity involvement (for a cervical rib)9 or back pain (for spinal segment distribution variants and transitional vertebra)10 has been reported before. This study aimed to assess the prevalence of these spinal segment variants and investigate the potential association among these variants in a population without histories of neck, dorsum, or low-back pain.
MATERIALS AND METHODS
This retrospective observational study was reviewed and approved by the institutional review board of The Johns Hopkins University to be compliant with the Health Insurance Portability and Accountability Act (this study was exempted from the informed-consent requirements).
Study Population
The integrated PACS of The Johns Hopkins Hospital was searched for records of young adults or older patients (17 years of age or older) who had undergone cross-sectional CT examinations of the whole spine in an inpatient or outpatient setting for indications such as trauma or oncologic surveys, during 4 years.
Cases with incomplete scans, with significant artifacts, and with inadequate visualization of the spine were excluded, and a total of 450 consecutive patients (sex: 62.0% [n = 279] women and 28.0% [n = 171] men; mean age, 31.2 [SD, 8.4] years; range, 17–45 years) evaluated for nonspinal conditions without a history of spinal diseases were included in this study.
Image Acquisition
CT examinations were obtained using the 16-section multidetector row CT scanner (Somatom Sensation 16; Siemens). Examinations were performed following the institutional protocol (voltage of 120 kV[peak] and the effective current setting based on the body mass index and indication). Examinations were reconstructed at 3.0 mm.
Image Interpretation
Several characteristics and features of vertebrae were extracted from each CT examination. The total number of presacral segments was documented by counting the vertebrae downward from C2. The cervical vertebrae included the reliable number of 7 segments,8,11 and the following rib-bearing segments downward were counted as thoracic vertebrae. The non-rib-bearing segments following the thoracic vertebrae were counted as the lumbar vertebrae.
The cervical ribs on CT examinations were identified using the following criteria: 1) must be attached to the C7 vertebral process, 2) must have no connections to the manubrium of the sternum, though it may form synostosis with the first rib (which differentiates it from a rudimentary first rib), and 3) must be separate from, though it may articulate with, the transverse process of C7 (if fused with the segment, it was classified as an elongated cervical process).3,12 The elongated C7 transverse processes were classified as any C7 transverse process longer than the T1 (first thoracic vertebra) transverse process.
The TLTV was identified as the segment with hypoplastic ribs (unilateral or bilateral, ribs with lengths of <3.8 cm) or accessory ossification centers8 on the lowest rib-bearing segment. The iliolumbar ligament (ILL) was identified and visualized as the structure extending from the transverse process of a vertebra to the posteromedial iliac crest on the axial view of CT examinations. The LSTV was identified and classified using the Castellvi classification.6 Table 1 shows the criteria used for LSTV classification.
The Castellvi classification for LSTV
The image interpretation was performed by 2 readers (G.K.T., radiology research fellow, and J.A.C., senior musculoskeletal radiologist) in consensus.
Statistical Analysis
Descriptive statistics were used for assessing frequencies and distributions of spinal segment variants. The frequencies of these variants in women and men were compared using the χ2 test (reporting P value).
The potential correlation between spinal segment variants was assessed using correlation studies reporting the Spearman ρ with 95% CIs (calculated by using the bootstrapping method with 1000 replicates) and P values. Results of the correlation studies are presented using a correlation matrix. Moreover, the potential association between these variants was studied using logistic regression models reporting ORs with 95% CIs and P values.
In this study, P < .05 was statistically significant. All statistical analyses were performed in the R platform (http://www.r-project.org/).
RESULTS
Among the 450 cases included in our study, frequencies of spinal segment distribution variants were as follows: 0.2% (n = 1) of cases had twenty-two, 1.8% (n = 8) had twenty-three, 93.3% (n = 420) had 24, and 4.7% (n = 21) had 25 presacral segments. Figures 1 and 2 show the spinal segment distribution variants in the thoracic (Fig 1) and lumbar vertebrae (Fig 2) in our study.

Allocation of spinal segment distribution variants in thoracic (rib-bearing) vertebrae.

Allocation of spinal segment distribution variants in lumbar vertebrae.
Overall, 23.8% (n = 107) of cases in our study had a spinal segment distribution variant (an atypical number of presacral segments or an atypical distribution of thoracolumbar vertebrae). The frequency of spinal segment distribution variants in women (25.4% [n = 71]) was similar to that in men (21.1% [n = 36], P value = .343, Table 2).
Comparative distribution of spinal segment variants
Cervical Rib
Of the 450 included cases, 4.2% (n = 19) had unilateral (1.6% [n = 7]) or bilateral (2.7% [n = 12]) cervical ribs (Fig 3). The frequency of cervical ribs in women (4.7% [n = 13]) was slightly higher compared with men (3.5% [n = 6]) in our study, though the difference was not statistically significant (P value = .728, Table 2).

Frequency and distribution of the cervical rib.
TLTV
A TLTV was present in 15.3% (n = 69) of cases in our study (unilateral: 7.3% [n = 33], bilateral: 8.0% [n = 36], Fig 4). Frequencies of the TLTV in women (12.9% [n = 36]) and men (19.3% [n = 33]) were similar (P value = .091, Table 2).

Frequency and distribution of the TLTV. AOC indicates accessory ossification center.
LSTV
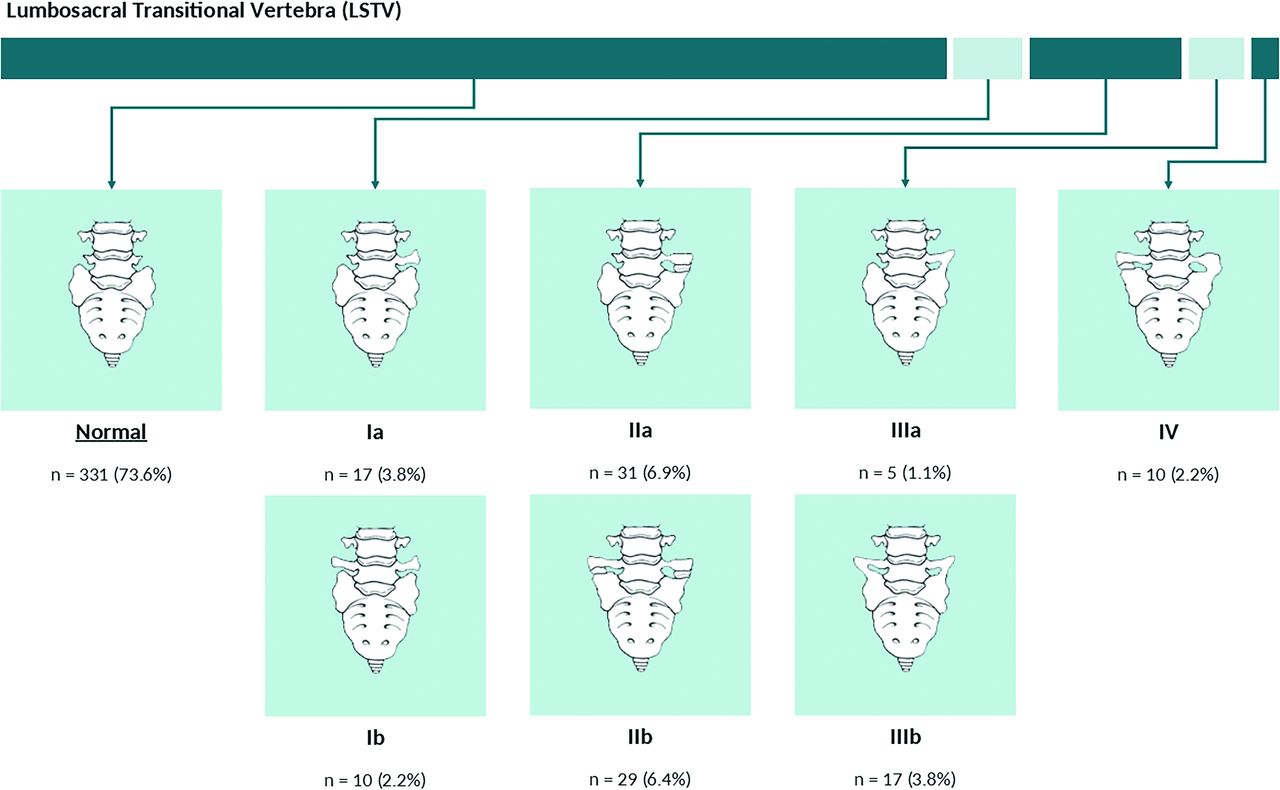
ILL was identified in 95.8% (n = 431) of cases (partially visualized: 12.4% [n = 56], definitely visualized: 83.3% [n = 375]). Of the 450 included cases, 26.4% (n = 119) had LSTV, of which 6.0% (n = 27) of cases had LSTV type I, 13.3% (n = 60) of cases had LSTV type II, 4.9% (n = 22) of cases had LSTV type III, and 2.2% (n = 10) of cases had LSTV type IV. Figure 5 shows the frequency and distribution of LSTVs in our study. LSTV was less frequent in women (21.5% [n = 60]) compared with men (34.5% [n = 59], P value = .003, Table 2).

Frequency and distribution of the LSTV.
Correlation and Association between Spinal Segment Variants
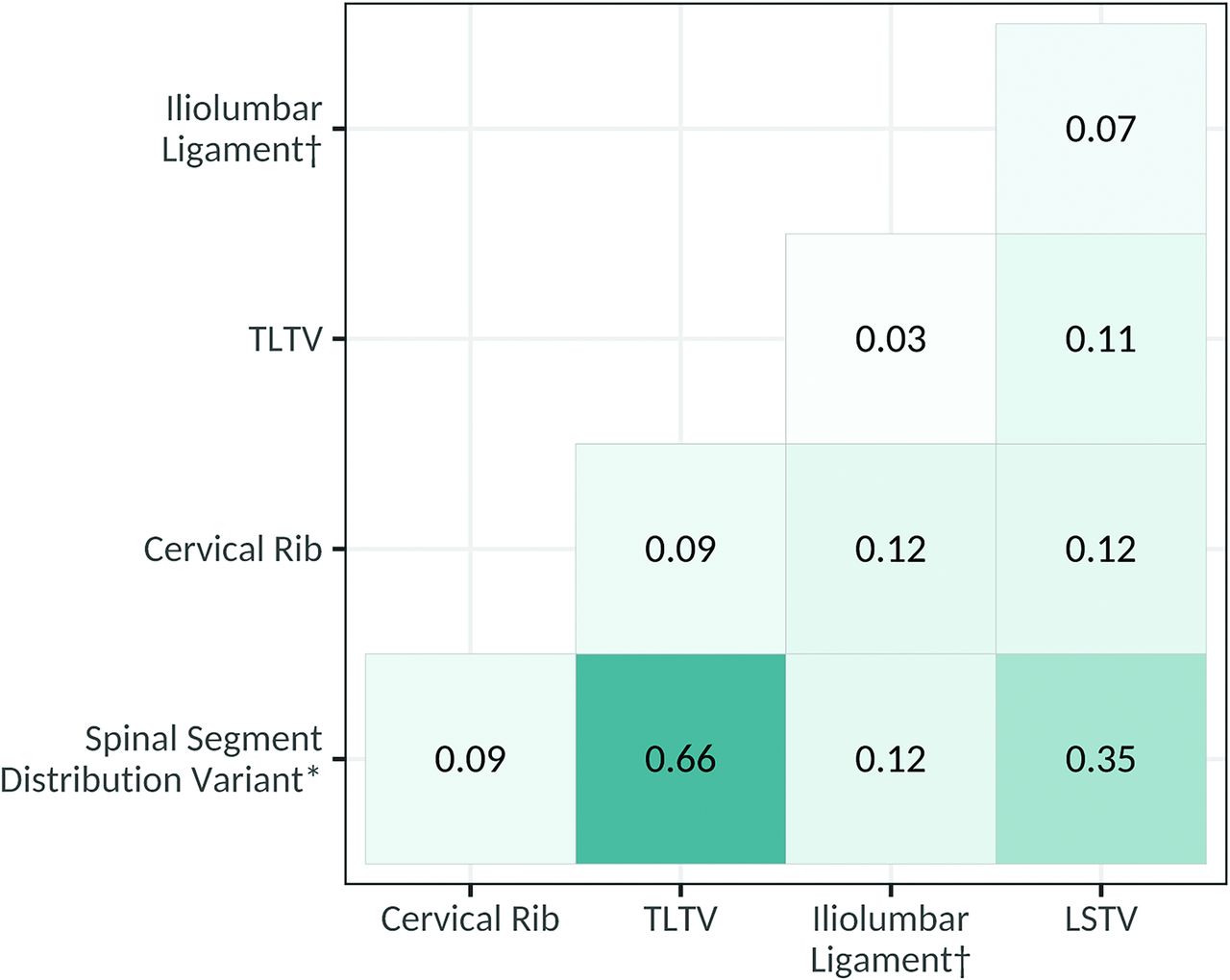
In our study, spinal segment distribution variants (an atypical number of presacral segments or an atypical distribution of thoracolumbar vertebrae) were correlated and associated with the presence of a concurrent TLTV (OR = 66.13; 95% CI, 30.34–166.85; P value =.001), an inability to visualize the ILL (OR = 3.06; 95% CI, 1.18–7.80; P value = .018), and a concurrent LSTV (OR = 5.47; 95% CI, 3.43–8.80; P value < .001, Fig 6 and Table 3).

Correlation between spinal segment variants. The asterisk indicates an atypical number of presacral segments or an atypical distribution of thoracolumbar vertebrae; dagger, the inability to visualize the ILL.
Association among spinal segment variants
The presence of a cervical rib was correlated and associated with the inability to visualize the ILL (OR = 4.86; 95% CI, 1.06–716.54; P value = .020) and a concurrent LSTV (OR = 3.28; 95% CI, 1.29–8.47; P value = .012). Moreover, the presence of a TLTV was correlated and associated with a concurrent LSTV (OR = 1.87; 95% CI, 1.08–3.20; P value = .023, Fig 6 and Table 3).
An inability to visualize the ILL was not associated with the presence of TLTV or LSTV (Fig 6 and Table 3).
An example of both a thoracolumbar and lumbosacral transitional anatomy is given in Fig 7.

Example of thoracolumbar and lumbosacral transitional anatomy. Coronal MIP CT image of the lumbar spine demonstrates thoracolumbar and lumbosacral anatomy with an accessory ossification center on the right at T12 (open arrow) as well as a partially sacralized L5 vertebral body with an unfused left transverse process (closed arrow).
DISCUSSION
Our study confirms that the prevalence of spinal segment variants, even in asymptomatic young adults, is relatively high. The spinal segment distribution variants (an atypical number of presacral segments or an atypical distribution of thoracolumbar vertebrae), the cervical rib, TLTV, and LSTV, affected 23.8%, 4.2%, 15.3%, and 26.4% of our study population. We also showed that the presence of a TLTV and LSTV is associated with higher odds of concurrent spinal segment distribution variants. Although not associated with the presence of TLTV and LSTV, the inability to visualize the ILL was also associated with the spinal segment distribution variants (atypical number of presacral segments or atypical distribution of thoracolumbar vertebrae) and the presence of a cervical rib.
The most prevalent number of presacral segments is 24 with 12 (rib-bearing) thoracic and 5 lumbar vertebrae. However, other spinal segment distribution variants are also common. The prevalence of atypical numbers of presacral segments was estimated to be as high as 8.2% (adults in an American population),8 7.9% (asymptomatic adults in a Chinese population),13 or 10.0% (adolescents with idiopathic scoliosis in an American population).14 In our study, atypical numbers of presacral segments were seen in 6.7% of cases, while 23.8% of cases were diagnosed with spinal segment distribution variants. Moreover, the pooled prevalence of a cervical rib is estimated to range from 1.1% (in adults without thoracic outlet syndrome) to 29.5% (in adults with thoracic outlet syndrome),9 depending on race/ethnicity, sex, or symptoms of the population, while in our study, this number was estimated as 4.2%. Among the other frequently encountered spinal segment variants, transitional vertebrae are estimated to be present in 11.2% (for TLTV)15 to 29.0% (for LSTV).16 Similar to other spinal segment variants, the prevalence of transitional vertebrae varies across subgroups of race/ethnicity and sex, and in our study on asymptomatic adults, the prevalence of transitional vertebra was on the order of 15.3% (for TLTV) and 26.4% (for LSTV).
It is estimated that the rate of wrong-level spine surgery is about 0.1%–2.1%,17 and considering the relatively high prevalence of spinal segment variants, several reports cited spinal segment variants (eg, spinal segment distribution variant or transitional vertebrae) as contributors to the wrong-level spine interventions or operations.1,2 Although few anatomic landmarks have been suggested for the identification of vertebral levels, the unreliability of these landmarks limits their clinical use.18⇓-20 For instance, conus medullaris, dural sac termination (among the intradural landmarks), and abdominal vasculature (eg, the origin of major blood vessels like renal or common iliac arteries) location may change with aging,21 and the accuracy of using the ILL for identifying L5 (fifth lumbar vertebra) is shown to be insufficient.8
In our study, we showed an association between transitional vertebrae or an inability to visualize the ILL with a spinal segment distribution variant. In other words, when a transitional vertebra is seen on imaging or the reader is unable to visualize the ILL, additional imaging should be considered to avoid wrong-level spine interventions or operations.
The findings of our study may have been tempered by a few, albeit important, limitations. First, the single-center design of our work and the lack of race/ethnicity diversity may limit the generalizability of our findings. Second, the use of CT examinations for assessing spinal segment variants (cervical rib, TLTV, or LSTV) has acceptable accuracy. However, compared with MR imaging, the CT examinations might not be the most accurate imaging technique for studying the ILL. Therefore, the frequency reported for the inability to visualize the ILL in our study may be an overestimate of the correct frequency in the clinical setting.
CONCLUSIONS
Our study shows that spinal segment variants are highly prevalent, ranging from 4.2% (cervical rib) to 26.4% (LSTV), even in a population of asymptomatic young adults. We showed that these variants are associated with each other, and for instance, the presence of TLTV or LSTV increases the odds of concurrent spinal segment distribution variants. These findings emphasize the previous suggestion by Carrino et al8 that when a spinal segment variant (eg, transitional vertebra) is diagnosed, additional imaging should be considered for spine enumeration before interventions or operations.8
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received August 22, 2023.
- Accepted after revision October 19, 2023.
- © 2024 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.