
Abstract
BACKGROUND AND PURPOSE: Restenosis is an important determinant of the long-term efficacy of carotid endarterectomy. Our aim was to assess the role of high-resolution vessel wall MR imaging for characterizing restenosis after carotid endarterectomy.
MATERIALS AND METHODS: Patients who underwent vessel wall MR imaging after carotid endarterectomy were included in this study. Restenotic lesions were classified as myointimal hyperplasia or recurrent atherosclerotic plaques based on MR imaging features of lesion compositions. Imaging characteristics of myointimal hyperplasia were compared with those of normal post-carotid endarterectomy and recurrent plaque groups. Recurrent plaques were matched with primary plaques by categories of stenosis, and differences in plaque features were compared between the 2 groups.
RESULTS: Twenty-two recurrent lesions from 18 patients (14 unilateral and 4 bilateral) were classified as myointimal hyperplasia or recurrent plaque. Myointimal hyperplasia showed no difference in enhancement compared with normal post-carotid endarterectomy vessels (5 unilateral) but showed stronger enhancement than recurrent plaques (80.10% [SD, 42.42%] versus 56.74% [SD, 46.54%], P = .042). A multivariate logistic regression model of plaque-feature detection in recurrent plaques compared with primary plaques adjusted for maximum wall thickness revealed that recurrent plaques were longer (OR, 4.27; 95% CI, 1.32–13.85; P = .015) and more likely to involve a flow divider and side walls (OR, 6.96; 95% CI, 1.37–35.28; P = .019). Recurrent plaques had a higher prevalence of intraplaque hemorrhage (61.5% versus 30.8%, P = .048) by a χ2 test, but compositional differences were not significant in the multivariate model.
CONCLUSIONS: Vessel wall MR imaging can distinguish recurrent plaques from myointimal hyperplasia and reveal features that may differ between primary and recurrent plaques, highlighting its value for evaluating patients with carotid restenosis.
ABBREVIATIONS:
- CEA
- carotid endarterectomy
- CCA
- common carotid artery
- IPH
- intraplaque hemorrhage
- MH
- myointimal hyperplasia
- VWMRI
- vessel wall MR imaging
Stroke-risk reduction by carotid endarterectomy (CEA) remains the standard-of-care treatment for high-grade stenosis,1,2 and postsurgical restenosis is an important determinant of its long-term efficacy, affecting 1%–36% of patients who undergo CEA.3⇓-5 Histologic studies revealed that recurrent carotid stenosis is mainly attributed to myointimal hyperplasia (MH) in the early postoperative period (within 2 years) and recurrent atherosclerosis thereafter.6,7 Although MH occurs more commonly early on, time intervals are broad, with substantial overlap with recurrent atherosclerosis.8
Recurrent plaque and MH have distinct pathologic compositions that may help guide management strategies. MH varies little in composition along the wall, consisting of mainly smooth-muscle cells and collagen.9 These lesions are not prone to ulcerate or progress to hemorrhage and embolism, so repeat CEA for MH may have less benefit than for recurrent plaque. Noninvasive surveillance may be preferable for these patients if they remain asymptomatic and without high-grade stenosis.10 In contrast, recurrent plaque may be prone to embolization and incident cerebrovascular events if high-risk features such as lipid cores or intraplaque hemorrhage (IPH) are present, necessitating surgical management.10 Therefore, preoperative characterization of carotid restenosis is necessary for determining the optimal therapeutic approach.
Risk assessment of carotid atherosclerotic plaque based on its composition characterization is well-established using high-resolution vessel wall MR imaging (VWMRI).11⇓-13 Histologic studies have demonstrated differences in composition between recurrent post-CEA plaque versus primary atherosclerotic lesions.9 The ability to identify unique compositional features of recurrent plaques may help drive therapies for these lesions. Our aim was the following: 1) to identify the distinct imaging appearances of recurrent lesions following CEA using VWMRI, and 2) to compare the imaging features of recurrent plaques with those of primary asymptomatic plaques.
MATERIALS AND METHODS
Study Population
We retrospectively included patients who underwent VWMRI after CEA at Johns Hopkins Hospital from 2008 to 2018. Reasons for patient referrals for VWMRI included the following: 1) post-CEA restenosis detected on routine sonography, MRA, or CTA; 2) post-CEA follow-up evaluation; and 3) evaluation of contralateral carotid stenosis in patients with a history of CEA. Patients with primary asymptomatic carotid plaques matched by category of stenosis (<50%, 50%−69%, 70%−99%) were included for comparisons. The institutional review board approved this Health Insurance Portability and Accountability Act−compliant study and provided an exemption to allow the inclusion of de-identified data for patients from whom we did not receive written consent.
Imaging Protocol
All patients underwent a contrast-enhanced VWMRI examination on a 3T MR imaging scanner (Achieva; Philips Healthcare) using an 8-channel phased-array carotid coil (Chenguang Medical Technologies Co). A standard VWMRI protocol was used for all examinations, which included pre- and postcontrast T1-weighted VWMRI and 3D TOF-MRA sequences.14 The 3D TOF-MRA sequence was used to localize the carotid bifurcations (acquired resolution, 0.55 × 0.55 × 1.1 mm3), and VWMRI was acquired using a 2D electrocardiogram-gated double inversion recovery turbo spin-echo sequence with the following parameters: TR/TE/echo-train length, 1 RR/9 ms/10; FOV, 140 × 105 mm; matrix, 400 ×300; section thickness, 2 mm; in-plane resolution, 0.35 × 0.35 mm2. Serial VWMRI slices were acquired perpendicular to the carotid lesion with 1 or 2 additional slices showing lesion-free segments. An additional 2D VWMRI was acquired if the lesion was too long to be covered by 11 slices. VWMRI was repeated 5 minutes after the intravenous injection of gadobutrol (Gadavist; Bayer Schering Pharma; 0.1 mmol/kg).
Image Analysis
Lesion Classification.
All VWMRI and MRA images were de-identified and interpreted by 2 experienced readers (Y.Q. and G.O., with 15 and 3 years of experience in carotid plaque imaging, respectively) who were blinded to the clinical and surgical history. A carotid lesion was defined as wall thickening with or without luminal narrowing. Readers were provided precontrast MR images (ie, TOF-MRA and VWMRI sequences) to determine the presence of carotid lesions and their types (ie, MH or atherosclerosis). MH consists almost entirely of smooth-muscle cells and an extracellular matrix and typically appears as concentric, whereas atherosclerotic lesions are characterized by lipid accumulation, abundant collagen, IPH, and calcium deposits and are eccentric.9,15 Therefore, on the basis of the established VWMRI features of various lesion compositions,14,16,17 a lesion was considered MH if it had concentric wall thickening and homogeneous signal intensity, with luminal stenosis identified on VWMRI and TOF-MRA. A lesion was considered atherosclerotic plaque if it had eccentric wall thickening and heterogeneous signal intensity with or without luminal stenosis. Endarterectomized vessels with no luminal stenosis or eccentric wall thickening were defined as normal post-CEA vessels.
Plaque Characterization.
For each identified carotid plaque, readers were allowed to view the postcontrast VWMRI to characterize its components (ie, lipid core, fibrous cap, calcification, IPH, and ulceration) on the basis of previously established criteria (Online Supplemental Data).14,17,18 Adventitial enhancement was categorized for primary and recurrent plaques as described previously: 0, no enhancement; 1, enhancement of <50% of the outer wall circumference; and 2, enhancement of >50% of the outer wall circumference.14 The circumferential location of the plaque was recorded (ie, along the flow divider, opposite the flow divider, or on the sidewalls) (Online Supplemental Data).
Quantitative Measurements.
Quantitative analyses were performed using VesselMass software (Leiden University Medical Center) based on previously described methods.19 The lumen and outer wall contours were manually traced on 3 continuous slices with maximal wall thickening on pre- and postcontrast VWMRI. The maximum wall thickness on the 3 postcontrast images was obtained. Plaque contrast enhancement was computed as the relative change in signal intensities from the pre- to postcontrast VWMRI. Signal intensities were standardized using spinal cord signal intensity if included in the image or noise contour mean, as previously described.20 The detailed quantitative measurements are shown in the Online Supplemental Data. The remodeling ratio was calculated as the outer wall area at the maximal stenotic site relative to the outer wall area at the reference site. For primary plaques, the nearest distal plaque-free segment was used as a reference. For recurrent plaques, to account for the influence of patches, the reference segment was measured at the nearest distal plaque-free segment if the plaque was within the surgical margin or at the most distal segment within the surgical margin if the plaque was beyond the surgical margin. Lesion length was measured on TOF-MRA by referencing VWMRI scans that showed the margin of the lesion. Carotid stenosis was measured on TOF-MRA according to the NASCET criteria.2
Statistical Analysis
Data were analyzed using STATA 14.0 (StataCorp). Continuous variables were compared using either the Student t test or the Mann-Whitney nonparametric test. Categoric variables (frequency of occurrences) were compared using χ2 tests. Multivariate logistic regression (adjusted for maximum wall thickness) was used to identify which imaging characteristics were associated with recurrent plaques. A P value < .05 was considered statistically significant.
RESULTS
Patient Recruitment
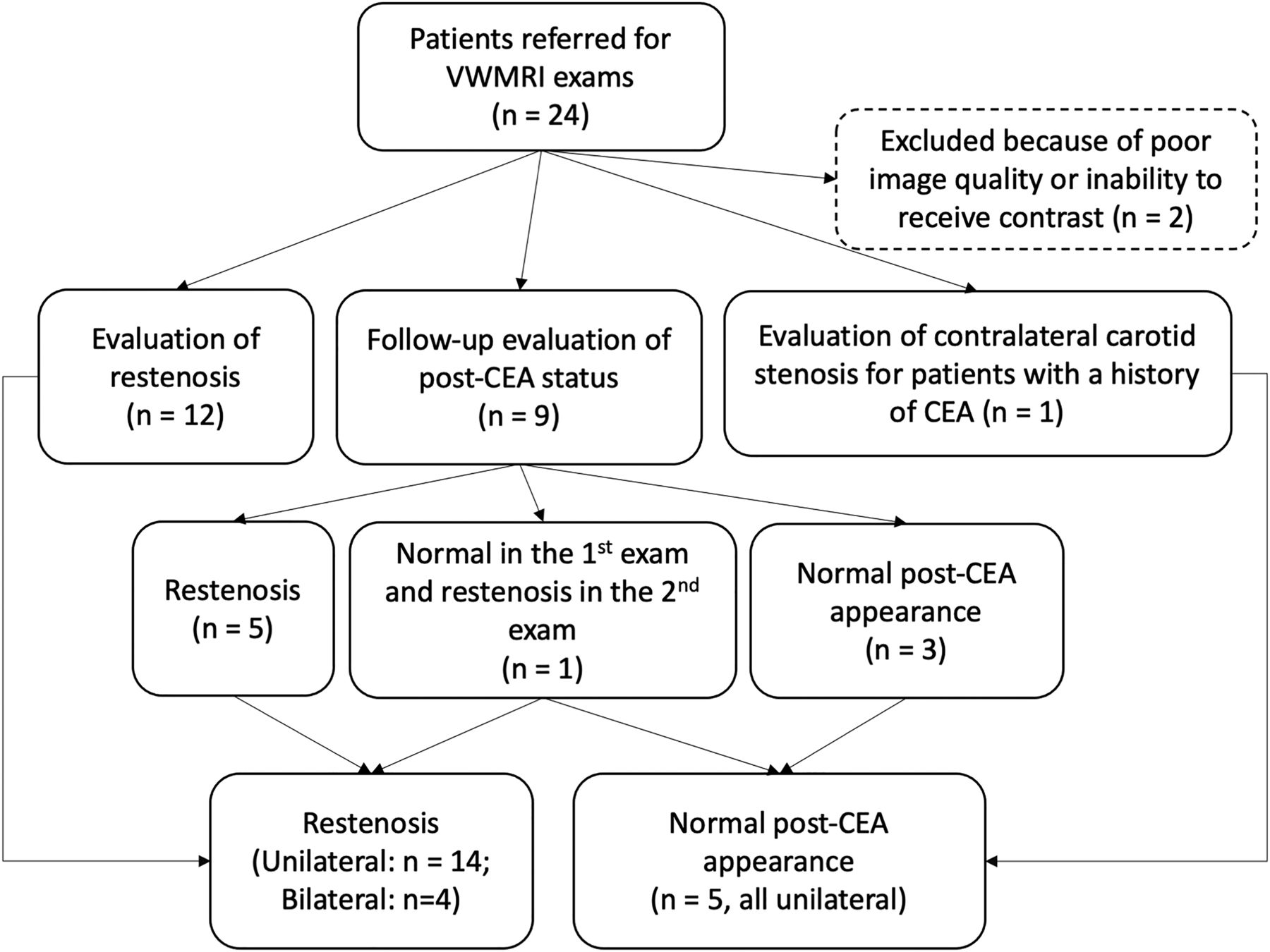
A total of 24 patients were referred for VWMRI after CEA (Fig 1). All CEAs were performed using the patch as the closure technique. Two patients were excluded because of poor image quality or an inability to receive contrast. In the remaining 22 patients (mean age, 72.2 [SD, 11.0] years, 15 men), 18 had restenosis (14 unilateral and 4 bilateral) and 4 had a unilateral normal post-CEA appearance. For the normal post-CEA group, we also included 1 patient who had normal findings on the first examination and returned with unilateral restenosis (Fig 2). All lesions were asymptomatic.

Flow chart of patient inclusion. The flow chart details referral reasons and exclusion criteria for patients with VWMRI examinations. N indicates number of patients.

Progression from normal post-CEA appearance to MH. TOF-MRA (A) of a post-CEA carotid artery shows an expected vessel geometry 2 months after the operation. Pre- (B) and postcontrast (C) VWMRI acquired at the proximal ICA (indicated by white line in A) shows vessel wall enhancement but no abnormal wall thickening of the proximal ICA (long arrows). TOF-MRA acquired 10 months after CEA (D) shows luminal stenosis. Pre- (E) and postcontrast (F) VWMRIs acquired at the same location (indicated by white line in D) show circumferential wall thickening with mild, homogeneous enhancement compatible with MH (long arrows). Short arrows in B, C, E, and F indicate the external carotid artery. VWMRIs were acquired using an electrocardiogram-gated double inversion recovery turbo spin-echo sequence (TR/TE/echo-train, 1 RR/9 ms/10; resolution, 0.35 × 0.35 × 2 mm3).
Classification of Carotid Artery Restenosis
A total of 22 restentoic lesions were identified in the 18 patients, in whom 9 lesions (40.9%) were concentric and predominantly homogeneous, suggestive of MH (Fig 3). The median interval from the operation to VWMRI scans for MH was 0.9 years (interquartile range, 0.8–1.6 years; ranging from 0.5 to 10.0 years). The other 13 lesions (59.1%) showed recurrent plaques that were eccentric and heterogeneous (Fig 4). The intervals from the operation to VWMRI scans for recurrent plaques (7.8 years; interquartile range, 2.8–9.3 years; ranging from 0.6 to 16.2 years) were longer than those of the MH group (P = .027). MH showed higher enhancement compared with recurrent plaques (80.10% [SD, 42.42%] versus 56.74% [SD, 46.54%], P = .042). Of the 9 MH lesions, 2 (22.2%) had 50%–69% stenosis and 2 (22.2%) had 70%–99% stenosis. In comparison, 3 of 13 (23.1%) recurrent plaques showed 50%–69% stenosis, and 5 (38.5%) showed 70%–99% stenosis. There was no difference in the degree of luminal stenosis between the MH and recurrent plaque groups (41% versus 55%, P = .252).

Representative images of MH. TOF-MRA (A) shows restenosis post-CEA extending from proximal to distal to the carotid bifurcation. Precontrast VWMRI (B) at the level of proximal ICA (indicated by white line in A) shows concentric homogeneous wall thickening (long arrow), indicative of MH. The lesion is enhanced on postcontrast VWMRI (C, long arrow). Short arrows in B and C indicate the external carotid artery. VWMRIs were acquired using an electrocardiogram-gated double inversion recovery turbo spin-echo sequence (TR/TE/echo-train, 1 RR/9 ms/10; resolution, 0.35 × 0.35 × 2 mm3).

Representative images of recurrent plaque. TOF-MRA (A) shows high-grade restenosis of the carotid bulb. The white line indicates the location of VWMRIs. Pre- (B, left image) and corresponding postcontrast (B, right image) VWMRIs show enhancing eccentric wall thickening with ulceration (asterisks), suggestive of a recurrent plaque. The corresponding specimen sections stained with MOVAT (C) confirm the diagnosis of recurrent plaque. The asterisk indicates ulceration. The arrowheads in B and C indicate the lumen. VWMRIs were acquired using an electrocardiogram-gated double inversion recovery turbo spin-echo sequence (TR/TE/echo-train, 1 RR/9 ms/10; resolution, 0.35 × 0.35 × 2 mm3).
Comparison of MH with Normal Post-CEA Vessels
Five carotid arteries had a normal appearance following CEA, with a median interval from CEA to VWMRI of 0.6 years (interquartile range, 0.1–3.0 years; ranging from 0.1 to 5.0 years). For the 9 vessels with MH, the mean length was 2.37 (SD, 1.19) cm and 6 (66.7%) showed both common carotid artery (CCA) and ICA involvement. The other 3 (33.3%) were limited to the CCA. No difference in enhancement was detected between normal post-CEA vessels and MH (mean, 82.97% [SD, 36.22%] versus 80.06% [SD, 42.42%], P = .824).
Comparison of Recurrent Plaques with Primary Atherosclerotic Plaques
Thirty-nine asymptomatic primary plaques from 38 patients showing heterogeneous signal intensity on precontrast images were matched with recurrent plaques by stenosis, so the percentages of each stenosis category were equally represented in the recurrent and primary plaque groups (<50% stenosis, 38.5%; 50%–69% stenosis, 30.8%; 70%–99% stenosis, 30.8%). Table 1 compares clinical and imaging characteristics between recurrent and primary plaques. Compared with primary plaques, recurrent plaques had a higher prevalence of IPH (61.5% versus 30.8%, P = .048). Recurrent plaques were much longer than primary plaques (mean, 2.26 [SD, 1.12] versus 1.47 [SD, 0.54], P = .001) along the long axis of the vessel. Seven of 9 (77.8%) recurrent plaques extended from the CCA to the proximal ICA. While most primary plaques were located opposite the flow divider (79.5%), recurrent plaques were more frequently distributed along flow divider or sidewalls (69.2%, P = .002), predominantly involving the flow divider (53.8%). Otherwise, recurrent plaques did not show significant differences in clinical risk factors (hypertension, hyperlipidemia, diabetes), the presence of plaque components (ie, lipid, fibrous cap, calcium, ulceration), remodeling ratio, or categories of adventitial enhancement compared with primary plaques.
Comparison of clinical and imaging characteristics between recurrent and matched primary plaquesa
The multivariate logistic regression analysis, including all characteristics found to be significantly different between primary and recurrent plaques, confirmed that lesion length (OR. 4.27; 95% CI, 1.32–13.85; P = .015) and involvement of the flow divider or sidewalls (OR, 6.96; 95% CI, 1.37–35.28; P = .019) were associated with recurrent plaques, after adjusting for maximum wall thickness (Table 2).
Multivariate logistic regression model for plaque-feature detection in recurrent plaques compared with primary plaques
DISCUSSION
We have shown increased contrast enhancement in MH compared with recurrent plaques using contrast-enhanced VWMRI. Compared with primary plaques, recurrent plaques had a potentially higher prevalence of IPH and more often involvement of the flow divider and side walls. This finding may highlight the importance of VWMRI for the evaluation of carotid restenosis.
Restenosis is a wound-healing process, in which inflammation plays a critical role in linking early vascular injury to neointimal proliferation and vascular narrowing.5 Contrast enhancement has been confirmed to be associated with inflammatory cells, neovessels, and fibrous tissue;21,22 thus, the greater contrast enhancement observed in the MH compared with recurrent plaques may reflect the stronger inflammatory response to the vascular injury and the greater contrast infiltration within the proliferated smooth-muscle cells and loose extracellular matrix in the MH. Furthermore, we observed no difference in contrast enhancement between MH and normal post-CEA vessels, suggesting that the inflammatory process begins immediately after blood-flow restoration following CEA when the involved vessels remain normal in appearance.23 Additionally, no difference in luminal stenosis was detected between MH and recurrent plaques, highlighting the importance of VWMRI in characterizing wall pathology of carotid restenosis. As demonstrated previously, recurrent plaque may have more embolic potential than MH and often necessitates surgical management,10 so the differentiation of recurrent plaque from MH on VWMRI may be valuable in clinical practice.
MH and atherosclerosis are often thought to occur at different time points following CEA, with MH typically occurring within 2 years and atherosclerosis taking longer to develop. However, a broad spectrum of changes can occur simultaneously, ranging from intimal thickening, atherosclerotic plaques to complex lesions with MH interspersed in the deep intima of atherosclerosis.8 In this study, we identified a case with MH diagnosed 10 years following CEA and a recurrent plaque that formed 7 months after CEA.
Despite sharing similar plaque components, recurrent plaques have been shown to be distinguishable from primary plaques on histology.9,24,25 Unlike primary plaques that consist of ordered plaque components (ie, a central necrotic core beneath a fibrous cap), recurrent plaque components are arranged in a less ordered manner. The necrotic core is superficial and not covered by a layer of collagen; and the thrombus is often deeply contained in the lesion rather than attached to the wall as a mural thrombus as detected in primary plaques.9 However, the aforementioned differentiation is not easily attainable on VWMRI because the imaging resolution is insufficient to allow the identification of a thin fibrous cap. A pathologic study demonstrated that IPH was an important feature that differentiated primary and recurrent plaques and reported 90% prevalence of IPH in recurrent lesions, much higher than in primary plaques (40%).24 IPH in primary plaques has been proved to be an important indicator of vulnerable plaques and is associated with a higher rate of stroke.14,26 A higher prevalence of IPH was more often found in recurrent plaques than in primary plaques in our study, implying that recurrent plaques may convey a higher stroke risk. However, the difference in IPH between the 2 groups did not reach significance in the multivariate regression, likely due to the small sample size in our study. Larger studies are needed to more confidently assess the prevalence of IPH in recurrent plaques and its association with the risk of further ischemic events. In contrast to our study, a prior VWMRI study reported a higher prevalence of fibroatheromatous tissue and smooth muscle and less lipid core in restenotic lesions compared with primary plaques,27 but the authors included MH in the restenotic lesion group, which may contribute to the difference in plaque components.
Primary atherosclerosis begins preferentially at the opposite wall of the flow divider, where the vessel wall is exposed to low wall shear stress that favors the formation of atherosclerosis.28,29 In contrast, recurrent plaques in our study were more often located at the flow divider or sidewalls, which are less prone to primary plaque formation and may be explained by the altered local hemodynamic characteristics after CEA in the carotid bulb.30 Both MH and recurrent plaques were diffusely distributed along the long axis of the carotid wall and involved both the ICA and CCA. In some cases, the external carotid artery was also involved. This may be attributable to the long extent of the CEA procedure.
There are some limitations to this study. First, due to the difficulty of obtaining restenosis specimens, MH or recurrent plaque was defined on the basis of imaging characteristics and not by histology, except for 1 case of recurrent plaque with a pathologic validation (Fig 4). Second, all CEAs were performed using patches that are suggested to reduce restenosis risk and recurrent stroke in comparison with primary closure by maintaining the arterial lumen diameter after the procedure.31 However, it is still unclear how distinct surgical procedures affect the formation and appearance of recurrent lesions, and post-CEA evaluation for other closure techniques (ie, primary closure) is needed for future investigation. Third, a small number of patients were included in the present study, and studies involving larger samples are warranted to validate our findings. Finally, VWMRI examinations were acquired at various time points after CEA due to the nature of clinical referrals, which may influence the imaging comparison between MH and recurrent plaques.
CONCLUSIONS
Contrast-enhanced VWMRI can distinguish primary atherosclerotic plaque from MH, suggesting a potential role for VWMRI in the evaluation of carotid restenosis. It also revealed differences in the distribution of plaque between primary and recurrent lesions and a possible increased frequency of IPH in recurrent lesions, offering some insight into plaque development and risk following CEA, though larger studies are needed for validation.
References
- Received April 29, 2021.
- Accepted after revision December 9, 2021.
- © 2022 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.