
Abstract
BACKGROUND AND PURPOSE: Blood-brain barrier permeability is not routinely evaluated in the clinical setting. Global cerebral edema occurs after SAH and is associated with BBB disruption. Detection of global cerebral edema using current imaging techniques is challenging. Our purpose was to apply blood-brain barrier permeability imaging in patients with global cerebral edema by using extended CT perfusion.
MATERIALS AND METHODS: Patients with SAH underwent CTP in the early phase after aneurysmal rupture (days 0–3) and were classified as having global cerebral edema or nonglobal cerebral edema using established noncontrast CT criteria. CTP data were postprocessed into blood-brain barrier permeability quantitative maps of PS (permeability surface-area product), Ktrans (volume transfer constant from blood plasma to extravascular extracellular space), Kep (washout rate constant of the contrast agent from extravascular extracellular space to intravascular space), VE (extravascular extracellular space volume per unit of tissue volume), VP (plasmatic volume per unit of tissue volume), and F (plasma flow) by using Olea Sphere software. Mean values were compared using t tests.
RESULTS: Twenty-two patients were included in the analysis. Kep (1.32 versus 1.52, P < .0001), Ktrans (0.15 versus 0.19, P < .0001), VP (0.51 versus 0.57, P = .0007), and F (1176 versus 1329, P = .0001) were decreased in global cerebral edema compared with nonglobal cerebral edema while VE (0.81 versus 0.39, P < .0001) was increased.
CONCLUSIONS: Extended CTP was used to evaluate blood-brain barrier permeability in patients with SAH with and without global cerebral edema. Kep is an important indicator of altered blood-brain barrier permeability in patients with decreased blood flow, as Kep is flow-independent. Further study of blood-brain barrier permeability is needed to improve diagnosis and monitoring of global cerebral edema.
ABBREVIATIONS:
- BBBP
- blood-brain barrier permeability
- EES
- extravascular extracellular space
- F
- plasma flow
- GCE
- global cerebral edema
- IVS
- intravascular space
- Kep
- washout rate constant of the contrast agent from EES to IVS
- Ktrans
- volume transfer constant from blood plasma to EES
- PS
- permeability surface-area product
- VE
- extravascular extracellular space volume per unit of tissue volume
- VP
- plasmatic volume per unit of tissue volume
The blood-brain barrier plays an important role in many CNS diseases relating to microvascular dysfunction and neuroinflammation, which are known to increase blood-brain barrier permeability (BBBP) in animal models.1 Obtaining quantitative BBBP information in the clinical setting would constitute a novel diagnostic and therapeutic strategy with widespread application. Global cerebral edema (GCE) represents a major complication in patients with SAH, is an independent predictor of SAH morbidity and mortality,2,3 and is thought to be related to disruption of the BBB. Moreover, delayed cerebral ischemia represents an independent major complication and poor prognostic factor in patients with SAH.4 Initial studies have shown that earlier diagnosis of delayed cerebral ischemia before manifestation of clinical symptoms, altered CBF, and NCCT findings is possible with BBBP imaging by using CTP.5 BBBP evaluation with CTP is a promising technique, especially in patients with SAH, given that these patients are critically ill, require intensive monitoring, and often have contraindications to evaluation with MR imaging.5 Currently, imaging diagnosis of GCE relies on NCCT demonstrating diffuse effacement of the hemispheric sulci and diffuse obscuration of the hemispheric gray-white matter junction at the level of the centrum semiovale.3 These findings are challenging to identify in the setting of diffuse SAH and increased intracranial pressure effacing the sulci and cisterns. Moreover, NCCT fails to provide a direct assessment of the hemodynamic and microvascular dysfunction thought to be central to the underlying pathophysiology of GCE. Quantitative imaging of microvascular parameters, such as measures of BBBP, may provide for more accurate detection and monitoring of GCE compared with NCCT and could potentially improve the clinical management and outcomes of patients after SAH.
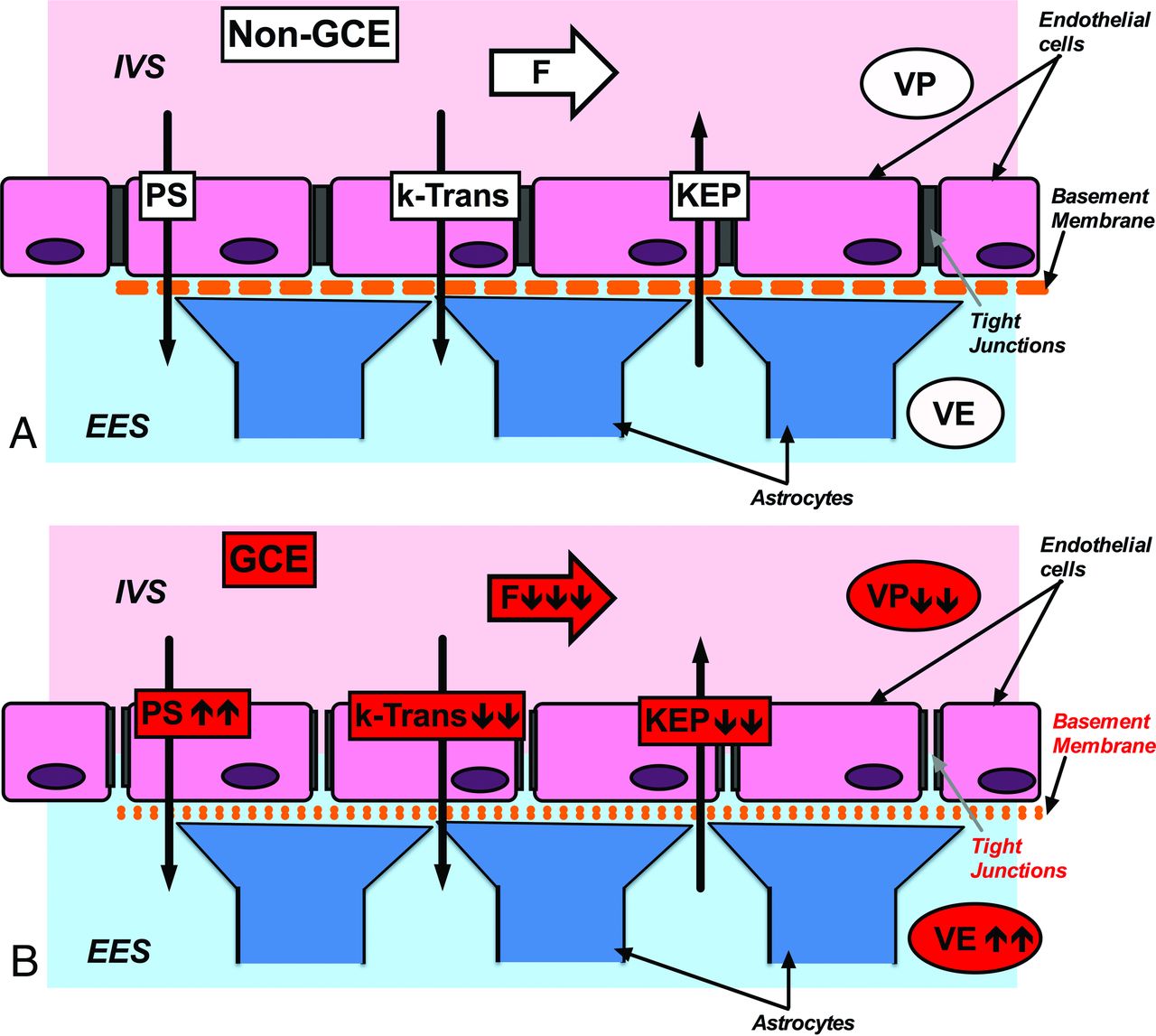
Extended CTP allows measurement of BBBP parameters not currently used in clinical practice. Kep represents the washout rate constant of the contrast agent from the extravascular extracellular space (EES) to the intravascular space (IVS). Kep therefore reflects the flow across the blood vessel wall from the EES to the IVS, and is independent of blood plasma flow. Based on transport equations proposed by Gowland et al6:
 where T is the time constant for transfer across the BBB. Therefore, Kep is thought to be related inversely to BBBP. Ktrans represents the volume transfer constant from the blood plasma to the EES. PS is the permeability surface-area product and represents the flow across the blood vessel wall from the IVS to the EES. VE represents the volume in the EES per unit of tissue volume, and VP represents the plasmatic volume per unit of tissue volume. F represents the plasmatic flow. In summary, Kep, PS, and Ktrans can be viewed as the primary BBBP parameters because they reflect flow across the BBB.6,7 On the other hand, VE, VP, and F are descriptive of hemodynamic conditions on either side of the BBB (the IVS or the EES, respectively). Fig 1 summarizes the relationships of BBBP parameters under normal conditions and in the setting of GCE. CTP has numerous practical advantages that make it highly suitable for critically ill patients: it is widely available, can be performed with most scanners, has few contraindications, and has rapid acquisition and processing times. Assessment of these parameters offers a promising technique to evaluate BBBP in the clinical setting. However, it has not been widely adopted in clinical practice, with few published investigations studying measures of BBBP.5,8,9
where T is the time constant for transfer across the BBB. Therefore, Kep is thought to be related inversely to BBBP. Ktrans represents the volume transfer constant from the blood plasma to the EES. PS is the permeability surface-area product and represents the flow across the blood vessel wall from the IVS to the EES. VE represents the volume in the EES per unit of tissue volume, and VP represents the plasmatic volume per unit of tissue volume. F represents the plasmatic flow. In summary, Kep, PS, and Ktrans can be viewed as the primary BBBP parameters because they reflect flow across the BBB.6,7 On the other hand, VE, VP, and F are descriptive of hemodynamic conditions on either side of the BBB (the IVS or the EES, respectively). Fig 1 summarizes the relationships of BBBP parameters under normal conditions and in the setting of GCE. CTP has numerous practical advantages that make it highly suitable for critically ill patients: it is widely available, can be performed with most scanners, has few contraindications, and has rapid acquisition and processing times. Assessment of these parameters offers a promising technique to evaluate BBBP in the clinical setting. However, it has not been widely adopted in clinical practice, with few published investigations studying measures of BBBP.5,8,9

Cytoarchitecture of the BBB and schematic representation of BBBP parameters derived from extended CTP. A, Non-GCE. At baseline, the BBB is composed of endothelial cells connected by tight junctions (as opposed to fenestrated endothelium outside of the CNS), the basement membrane, and the astrocyte processes. B, In the setting of GCE, there is an increase in EES as reflected by increased VE and decreased Kep, indicating increased BBBP (indicated in the drawing by a more porous basement membrane and tight junctions). PS is also elevated, indicating increased BBBP. Importantly, Kep is independent of F. In GCE, Kep is the most reliable parameter to evaluate BBBP in the setting of flow impairment.
The purpose of our study was to apply BBBP imaging by using extended CTP in the setting of GCE and to quantitatively assess its parameters. We hypothesize that application of extended CTP is able to detect a significant difference in the BBBP parameters in patients with GCE compared with patients without GCE in the early phase after SAH.
Materials and Methods
Population
This study was an institutional review board–approved retrospective analysis performed on consecutive patients with SAH enrolled in a prospective diagnostic accuracy trial at our institution. SAH was determined by a combination of NCCT, CTA, DSA, and/or CSF analysis. In this prospective study design, CTP was performed on days 0–3 after aneurysmal rupture to assess baseline cerebral perfusion and to compare with later examinations for interval change. All patients underwent either endovascular coiling or surgical clipping before CTP. Demographic and clinical data were collected (Table 1).
Clinical characteristics of the study population
All patients with SAH with CTP performed on days 0–3 were included in our study. Exclusion criteria were CTP examinations with severe motion degradation limiting postprocessing methods and unavailable CTP data from archives for postprocessing.
Patients were classified into 3 outcome groups: GCE (n = 11), non-GCE (n = 11), and indeterminate (n = 2) based on admission NCCT. GCE was defined using the following established criteria3: complete or near-complete effacement of the hemispheric sulci and basal cisterns and bilateral and extensive disruption of the hemispheric gray-white matter junction (including basal ganglia) at the level of the centrum semiovale.3 Absence of both features resulted in classification as non-GCE. If only 1 feature was present, patients were classified as indeterminate. Classification was performed independently by 2 board-certified neuroradiologists (15 years and 3 years of experience) blinded to all other clinical and imaging data. Consensus reading was provided for adjudication. Interobserver agreement was analyzed using the κ coefficient.
Image Acquisition, Postprocessing, and Quantitative Analysis
CTP was performed in the early phase (days 0–3) after SAH, along with NCCT and CTA, as part of our study trial protocol. NCCT was performed from the foramen magnum to the vertex by using the following parameters: 120 kVp, 250 mAs, 1.0 rotation time, and 5.0-mm collimation.
Extended CTP scanning was performed on a 64-section scanner (LightSpeed Discovery HD-750; GE Healthcare, Milwaukee, Wisconsin) with an axial shuttle mode protocol for simultaneous acquisition of CTA and CTP data using the following parameters: 80 kVp, 400 mAs, 0.4 rotation time, 5.0-mm collimation with 17 cine cycles, and 2.8-second interscan delay for the first pass. Second pass technique included 10 cine cycles with a 10-second interscan delay. A total of 90 mL of nonionic contrast was intravenously administered at 4.0 mL/s followed by a 30 mL saline-bolus chaser. Average CT dose index volume was 300 mGy and average dose-length product was 2500 mGy-cm for the entire examination, including NCCT, CTA, and extended CTP.
For this study, CTP data were postprocessed off-line into maps of the BBBP parameters (Kep, Ktrans, PS, F, E [extraction fraction of contrast agent], VE, and VP), CBF, CBV, and MTT by using commercially available software (Olea Sphere V.2.0; Olea Medical, La Ciotat, France), based on previously published recommendations and guidelines.8,10 Quantitative analysis of CTP data was performed using standardized sampling of the cerebral cortex according to established methods4,11 with round, continuous ROIs placed along the cerebral cortex. Up to 24 ROIs were included in each CTP section, distributed in the following territories: approximately 4 in the anterior cerebral artery, 12 in the middle cerebral artery, and 4 in the posterior cerebral artery territories. ROIs overlying large cortical vessels with CBF greater than 100 mL/100 g/min were excluded from the statistical analysis.12 Mean values and 95% CIs were calculated using the remaining ROIs in all CTP sections for each patient. Unpaired t tests were performed to compare Kep, Ktrans, PS, F, extraction fraction of contrast agent, VE and VP, as well as CBF, CBV, and MTT in the GCE and non-GCE groups.
Permeability Modeling
Permeability parameters were calculated using the Delayed Lawrence and Lee Model.13 According to the Delayed Lawrence and Lee Model, Kep represents the washout rate constant of the contrast agent from the EES to the IVS. The formula for Kep is:
 Kep appears to have an inverse relationship with BBBP, and therefore decreases with increased permeability. Importantly, Kep is independent of flow.6
Kep appears to have an inverse relationship with BBBP, and therefore decreases with increased permeability. Importantly, Kep is independent of flow.6
Ktrans equals the blood plasma flow per unit volume of tissue, derived through the formula:
 where E represents the extraction fraction of contrast agent that leaves the IVS in the first pass of the bolus through the vascular bed. E has no units assigned and has a value between 0 and 1. F represents the plasma flow per unit tissue volume and its units are mL × mL−1 × min−1. Ktrans is dependent on the blood flow.
where E represents the extraction fraction of contrast agent that leaves the IVS in the first pass of the bolus through the vascular bed. E has no units assigned and has a value between 0 and 1. F represents the plasma flow per unit tissue volume and its units are mL × mL−1 × min−1. Ktrans is dependent on the blood flow.
PS represents the flow across the blood vessel wall from the IVS to the EES. The formula for PS is:
 where Hct is the hematocrit. According to recommendations contained in the Olea Manual, a default hematocrit level is set to 0.45 for the calculation of all derived perfusion and permeability parameters for which a hematocrit level is required. PS increases with increased permeability; however, PS is also flow-dependent.6
where Hct is the hematocrit. According to recommendations contained in the Olea Manual, a default hematocrit level is set to 0.45 for the calculation of all derived perfusion and permeability parameters for which a hematocrit level is required. PS increases with increased permeability; however, PS is also flow-dependent.6
In summary, Kep, PS, and Ktrans have previously been used to assess BBBP in patients9,14 and animal models.15,16 However, according to the Lawrence and Lee Model derivations above, decreasing Kep most accurately reflects increasing disruption and permeability of BBB, especially in the setting of impaired CBF, such as occurs in GCE.12
Results
Study Population
Twenty-two patients were included in the study after excluding indeterminate patients (n = 2) from the statistical analysis. In the 22 patients, 50% (11/22) were classified as having GCE and 50% (11/22) as non-GCE. There was statistically significant high interobserver reproducibility, with κ interobserver agreement coefficient of 0.86 (P < .0001) for sulcal effacement and 0.73 (P < .0001) for gray-white matter differentiation between the 2 blinded neuroradiologists. Clinical characteristics of the study population are summarized in Table 1.
Global BBBP Analysis
Quantitative BBBP results along with CTP results are summarized in Table 2. Kep, Ktrans, VP, and F were significantly decreased, while VE was significantly increased, in the GCE group compared with the non-GCE group. Differences in PS and extraction fraction of contrast agent did not reach statistical significance. However, there was a trend for increased PS in GCE. CBF was significantly decreased in the GCE group compared with the non-GCE group, while differences in CBV and MTT did not reach statistical significance.
Quantitative BBBP and CTP resultsa
Fig 2 demonstrates quantitative BBBP maps in a representative patient from the GCE group and a representative patient from the non-GCE group, respectively.

BBBP quantitative maps of Kep, Ktrans, and VE in a representative patient from the GCE group (top panel) and a representative patient from the non-GCE group (bottom panel). NCCT images demonstrate loss of gray-white matter differentiation and presence of sulcal effacement in the patient with GCE. Corresponding BBBP maps reveal decreased Kep, slightly decreased Ktrans, and increased VE in the same patient compared with the patient without GCE.
Discussion
Assessment of BBBP with CTP is a novel technique that has not been adopted in clinical practice despite its numerous practical advantages, including widespread availability and relatively low cost. Quantitative BBBP evaluation in the clinical setting promises new insights into the underlying pathophysiology of many neurologic diseases. The relationship between BBBP and microvascular dysfunction and neuroinflammation plays an important role in numerous conditions, such as GCE.
GCE remains a major complication after SAH. Presently, assessment of GCE relies primarily on NCCT findings that are often difficult to identify in the setting of diffuse SAH and increased intracranial pressure. Given the influence of GCE on SAH morbidity and mortality, earlier detection of GCE may improve outcomes in SAH.3
At present, there are no clinically established methods to assess the pathophysiologic mechanisms underlying GCE, such as microvascular dysfunction, inflammatory effects, and neurotoxic effects of blood.3 Given that these factors also play a role in BBB dysfunction, we have evaluated the utility of BBBP parameters in the assessment of GCE after SAH. However, these findings may be applicable to a wide spectrum of conditions where cerebral edema is known to occur, such as acute stroke, traumatic and anoxic brain injury, and CNS infections.
Our findings suggest that Kep decreases with increased BBBP14,15 and may represent the most useful parameter in GCE because it is independent of low blood flow conditions. This inverse relationship between Kep and BBBP could be attributed to the underlying pathophysiologic mechanisms, including time kinetics. Kinetic analysis of BBBP changes during focused sonography-induced BBB opening demonstrated initial decrease in Kep with subsequent recovery over time.16 Therefore, time kinetics are a crucial component in the assessment of the different BBBP parameters. In our study, we measured BBBP at a very early (initial) stage in patients with SAH who develop GCE demonstrating decreased Kep. However, future work will show if Kep recovers on follow-up examinations in these patients. The exact timing of BBBP imaging during the course of the disease is an important factor in understanding Kep in these patients, as it relates to the timing of the BBB breakdown.
In contrast, Ktrans is dependent on blood flow and also decreased with increased BBBP in our study, representing a less reliable parameter for assessment of BBBP in GCE. Furthermore, our findings demonstrate significant differences in VE and VP in patients with GCE. The mathematical derivation of VE and VP is based on the fractions of volume of the EES and IVS, respectively. Fig 1 summarizes the relationships of these BBBP parameters under normal conditions and in the setting of GCE. In the setting of interstitial edema such as GCE, fluid from the IVS (represented by VP) transgresses the BBB into the EES (represented by VE). In GCE, there is an increase in EES as reflected by increased VE and decreased Kep, indicating increased BBBP. Furthermore, our findings also demonstrated significantly decreased Ktrans and F in patients with GCE. In the literature, CBF impairment recently has been reported in patients with GCE.12 Our data demonstrated decreased CBF in patients with GCE compared with patients without GCE and is thus concordant with previously published studies.12 Because the derivation of Ktrans is dependent on F, it is a less reliable parameter in flow-restricted conditions, such as seen in GCE.17 Given that Kep is independent of F, it may represent a more useful parameter to assess BBBP in the context of GCE, particularly when flow impairment occurs.12 These findings further contribute to the development of an imaging biomarker of BBBP in flow-restricted conditions such as cerebral edema.
In this initial exploratory study, our sample was limited to patients with SAH who had an extended CTP technique performed. Future studies evaluating BBBP parameters in other patient populations such as stroke, hypoxic-ischemic injury, traumatic brain injury, neoplasm, and inflammation will be important to improving our understanding of BBBP in different clinical settings as well as to evaluate BBBP parameters as potential outcome measures in specific disease states.
Although there was a trend for increased PS in patients with GCE compared with patients without GCE, statistical significance was not achieved. However, these findings support further prospective work to elucidate the pathophysiologic processes leading to GCE after SAH.
Conclusions
Further study of BBBP is needed to improve diagnosis and monitoring of GCE. Validating a potential quantitative imaging biomarker may improve detection and management of GCE and may provide a quantitative end point for future clinical trials aimed at improving SAH outcomes.
Footnotes
Disclosures: Jana Ivanidze—RELATED: Grant: Radiological Society of North America Research and Education Foundation,* Comments: Resident Research Grant 2014–2015. Ajay Gupta—RELATED: Grant: CTSC Pilot Award (NIH/NCATS Grant # UL1TR00457)*; UNRELATED: Grants/Grants Pending: Foundation of the American Society of Neuroradiology Scholar Award.* Jan Claassen—UNRELATED: Consultancy: Actelion, Sage, Comments: Advisory board for study planning. Pina C. Sanelli—RELATED: Grant: Brain Aneurysm Foundation Grant 2014–2015. *Money paid to the institution.
This work was supported by the Radiological Society of North America Research and Education Foundation Resident Research Grant (awarded to J.I.), the Brain Aneurysm Foundation Grant (awarded to P.C.S.), and grant 5K23NS058387 from the National Institute of Neurological Disorders and Stroke (NINDS), a component of the National Institutes of Health (NIH). Its contents are solely the responsibility of the authors and do not necessarily represent the official view of NINDS or NIH.
Paper previously presented at: Annual Meeting of the American Society of Neuroradiology, April 25–30, 2015; Chicago, Illinois.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received June 22, 2015.
- Accepted after revision February 22, 2016.
- © 2016 by American Journal of Neuroradiology





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Alterations in Blood-Brain Barrier Permeability in Patients with Systemic Lupus Erythematosus
- Early focal brain injury after subarachnoid hemorrhage correlates with spreading depolarizations
- Effects of Radiation Exposure on the Cost-Effectiveness of CT Angiography and Perfusion Imaging in Aneurysmal Subarachnoid Hemorrhage