
Abstract
BACKGROUND AND PURPOSE: Brain CT is widely used to exclude or confirm acute cerebral venous sinus thrombosis. The purpose of this study was to assess the value of attenuation measurement and the H:H ratio on unenhanced brain CT scans in the diagnosis of acute cerebral venous sinus thrombosis.
MATERIALS AND METHODS: This retrospective study evaluated 20 patients with acute cerebral venous sinus thrombosis and 20 age- and sex-matched control participants without thrombosis. Three experienced observers independently evaluated the unenhanced brain CT scan for the presence of cerebral venous sinus thrombosis and measured the attenuation in the dural sinuses. Interreader differences were examined, as well as densities and H:H ratio between patients with acute cerebral venous sinus thrombosis and control participants.
RESULTS: A significant difference in the average sinus attenuation was found between patients with acute cerebral venous sinus thrombosis (73.9 ± 9.2 HU) and the control group (52.8 ± 6.7 HU; P < .0001). A similar difference was found for the H:H ratio (1.91 ± 0.32 vs 1.33 ± 0.12 in patients with and without cerebral venous sinus thrombosis, respectively; P < .0001). Optimal thresholds of 62 HU and 1.52 lead to accuracies of 95% for average sinus attenuation and 97.5% for the H:H ratio, respectively.
CONCLUSIONS: Hyperattenuation and the H:H ratio in the dural sinuses on unenhanced brain CT scans have a high accuracy in the detection of acute cerebral venous sinus thrombosis.
ABBREVIATIONS:
- CVST
- cerebral venous sinus thrombosis
- HCT
- hematocrit
- H:H ratio
- Hounsfield unit-to-hematocrit ratio
- HU
- Hounsfield unit
- ICC
- intraclass correlation coefficient
Cerebral venous sinus thrombosis (CVST) is a challenging neurologic disorder because of the wide variety of clinical manifestations. The annual incidence is estimated at 2 to 7 cases per a population of 1 million. There are numerous causes and predisposing factors for CVST. The clinical features are nonspecific, and as a consequence, brain CT scan is often requested for exclusion of CVST.1 Although timely and correct anticoagulation or thrombolytic therapy may improve clinical outcomes, the diagnosis is often delayed.
Unenhanced brain CT scan is a cost-effective and widely available imaging technique in an emergency setting. The classic sign of acute CVST on unenhanced CT images is an increase in attenuation of the occluded sinus, reflecting a newly formed thrombus.2 It is accepted as a useful technique to decide on further imaging and is reported to have a sensitivity and specificity of 64.6% and 97.2%, respectively, in the detection of CVST.3,4
The attenuation of blood on unenhanced CT scans is predominantly caused by the protein factor of hemoglobin within the red blood cells. As a result, a linear relationship existed between the attenuation of blood and hemoglobin and HCT levels in a large series of 166 patients.5 The most common cause of false-positive interpretation of CVST on unenhanced CT scans is a high HCT (eg, in patients with polycythemia vera), causing a hyperattenuated sinus.6,7
Because an apparent increase in attenuation can be misleading and is not always visually picked up, measurement of attenuation in the sinus might be a more reliable method. Normalization of measured attenuation regarding HCT may further improve the detection of CVST on unenhanced CT scans.5
Black et al5 also measured the attenuation of the venous sinus in 8 patients with CVST and suggested the potential usefulness of attenuation measurements and H:H ratio to diagnose CVST. The purpose of our study was to assess the clinical usefulness of attenuation measurement and to compare its normalized ratio with HCT in the diagnosis of acute CVST on unenhanced brain CT scans.
Materials and Methods
We compiled a radiologic data base of patients with CVST who were admitted to our institution between 2003 and 2011. Patients had to meet the following inclusion criteria: 1) unenhanced brain CT scan on admission, and 2) a confirmed diagnosis of CVST with CT venography and/or MR venography within 24 hours. These criteria led to a selection of 29 patients, and their clinical reports were read. Of these, 9 patients were excluded because they presented with symptoms older than 7 days before the CT scan.
Records of the remaining 20 patients (17 women, 3 men; mean age, 35.1 years; age range, 0–60 years) with confirmed acute CVST were analyzed. Patient demographics, hemoglobin, HCT, serum urea nitrogen, and creatinine levels from the day of the examination or 1 day before or after were documented. The location of the thrombus is listed in the Table. All CT images were acquired on 1 of 3 different systems: Sensation 64, Sensation 16, or Navigator (Siemens, Erlangen, Germany). The following scanning parameters were used: 120 kV, 300 mA, and a section thickness of 2.5 below the tentorium and 6 mm above the tentorium.
Location of thrombus in 20 patients with acute CVST
For our case-control study, the initial unenhanced brain CT examinations of the 20 confirmed cases of patients with CVST were sex- and age-matched with 20 patients who did not have CVST. These examinations were loaded in a diagnostic viewing station (Impax; Agfa-Gevaert, Mortsel, Belgium) in alphabetical order and were read by 2 experienced neuroradiologists and 1 experienced radiologist. Although the readers knew the purpose of the study, they were blinded to patient clinical data and any prior or follow-up imaging. The readers were asked to determine the presence or absence of CVST considering all possible CT signs. If they suspected a venous sinus to have a thrombosis, they measured the attenuation on 3 different locations in the respective sinus by using the cursor. If not, they measured the attenuation in 3 random, but different, venous sinuses they believed to be reliably differentiated from the surrounding brain parenchyma.
The measured densities were documented in HU. To normalize them regarding HCT, we calculated the H:H ratio for all 40 patients.
We performed statistical analysis by using the Analyze-It 2.12 (Analyze-It, Leeds, England) and SPSS 13.0 for Windows (SPSS, Chicago, Illinois) software packages. All continuous variables are presented as mean ± SD, unless specified otherwise. Intrareader correlations were assessed by use of the ICC. For both the attenuation and the H:H ratio, receiver operating characteristic curves were obtained and were used to find optimal cutoff values, for which sensitivity, specificity, and accuracy were reported. We performed all comparisons between patients with CVST and control participants by using Mann-Whitney tests. A P value of < .05 is considered to indicate a statistically significant difference.
Results
HCT levels ranged from 25.3% to 46.3% (mean, 39.2%) in the patient group and 30.8% to 44.2% (mean, 39.8%) in the control group (P = .76). Hemoglobin levels ranged from 6.9 to 14.8 g/dL (mean, 11.5 g/dL) in the positive patient group and 10.6 to 15.3 g/dL (mean, 13.6 g/dL) in the control group (P = .52). Also, the serum urea nitrogen and creatinine levels were not significantly different between groups (serum urea nitrogen: 24.6 ± 7.3 vs 24.3 ± 8.4 mg/dL and creatinine: 0.69 ± 0.25 vs 0.70 ± 0.17 mg/dL for the patients with CVST and the control participants, respectively). None of the patients had elevated serum urea nitrogen-to-creatinine ratios (signifying dehydration) that could cause elevated blood attenuation.
The average time from the onset of neurologic symptoms until the unenhanced brain CT examination was 3 days (range, 1–7 days).
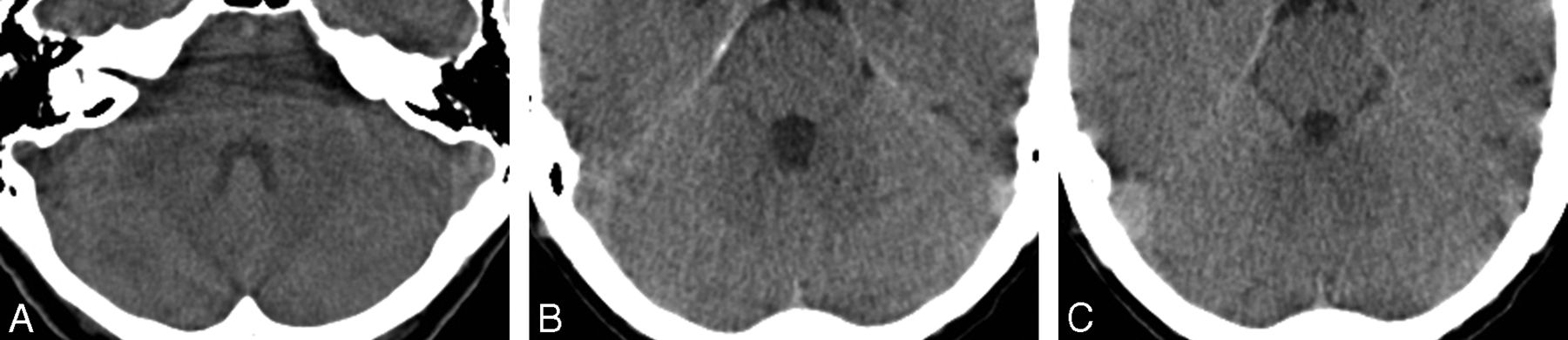
The readers used both direct and indirect signs on CT scans to evaluate the presence of a venous sinus thrombosis and were able to correctly identify most cases. A hemorrhagic venous infarct was present in 4 of 20 patients with acute CVST. There was no difference among the readings of the 3 observers. False-negative readings were noted in 2 patients (2 readers in 1 patient and 1 reader in 1 different patient). One of the patients in whom a sinus thrombosis was missed had a low HCT (36.8%), which caused the sinus to appear less attenuated (Fig 1). It is possible that 1 false-positive case (by 1 reader) in a patient with a relatively high HCT (43%) may have caused the incorrect interpretation (Fig 2).

Axial brain CT scan in a patient with false-negative results (left sigmoid sinus according to the measurements of 2 readers [mean HU, 55; HCT, 39.6; H:H ratio, 1.39]).

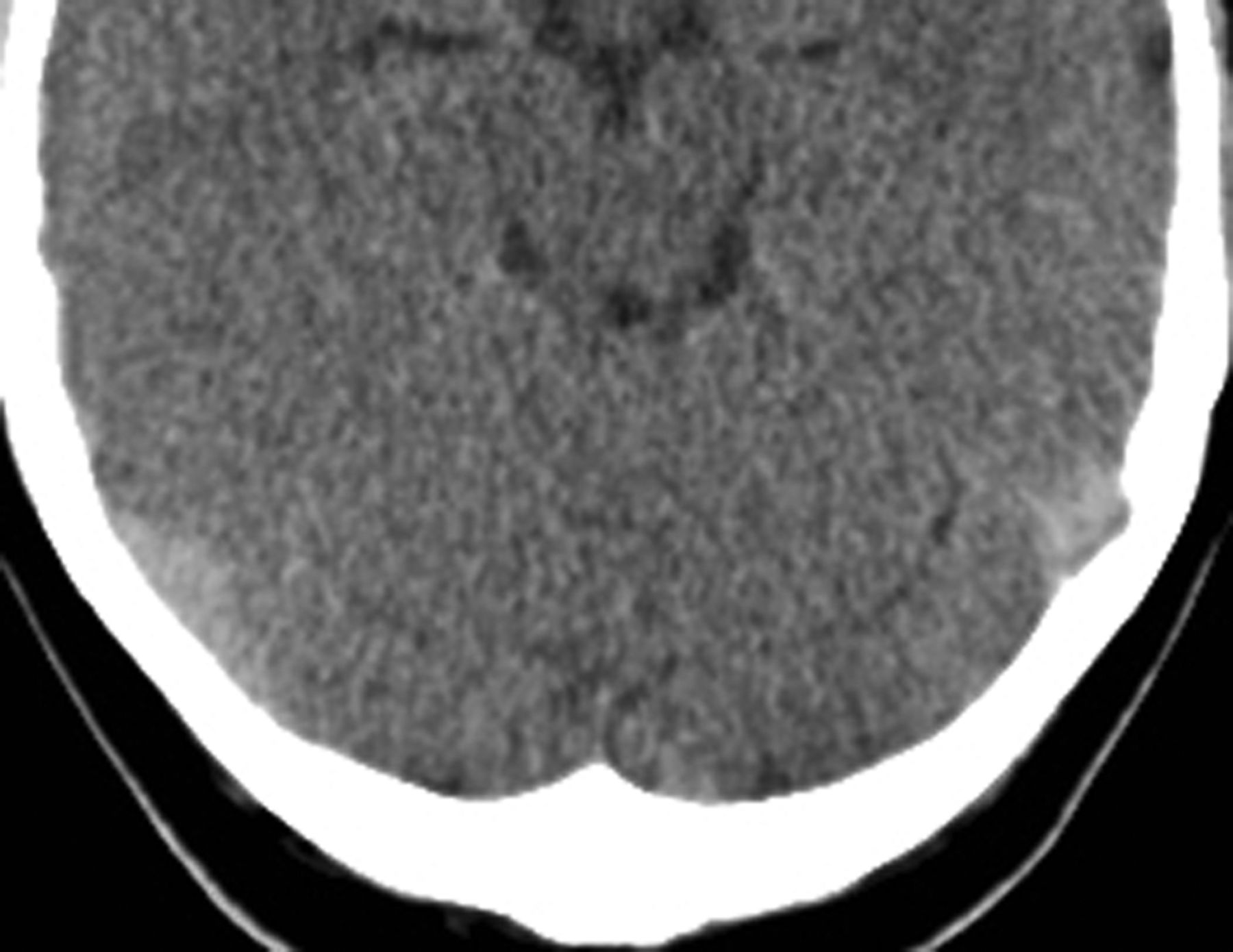
Axial brain CT scan in a control participant with false-positive results in the transverse sinuses according to the measurements of 1 reader (mean HU, 66.3; HCT 43; H:H ratio, 1.54).
For all readers, significant differences in attenuation were found between patients with and without sinus thrombosis, with overall higher attenuation values in patients with thrombosis (Fig 3). A high ICC was found among the 3 readers (ICC, 0.88), with ICC values for each of the pair-wise comparisons ranging between 0.86 and 0.91. To limit influences of outliers among readers, the averaged attenuation value of the 3 readers was used for further evaluation. This method led to values of 73.9 ± 9.2 HU for patients with CVST and 52.8 ± 6.7 HU for the control participants (Fig 4), which were also significantly different (P < .0001). The receiver operating characteristic analysis of the attenuation showed an area under the curve of 0.985 and an optimal cutoff value of 62 HU, leading to a sensitivity of 95%, specificity of 95%, and accuracy of 95%.

Axial brain CT scan in a patient with a thrombosis in the superior sagittal sinus (A) and right transverse sinus (B) (mean HU, 76.6; HCT, 40.2; H:H ratio, 1.86).

The average attenuation values among the 3 readers was significantly different in patients with acute CVST (73.9 ± 9.2 HU) compared with control participants (52.8 ± 6.7 HU) (A). The H:H ratio showed values of 1.33 ± 0.12 in patients without CVST, and 1.91 ± 0.32 in patients with CVST (P < .0001) (B).
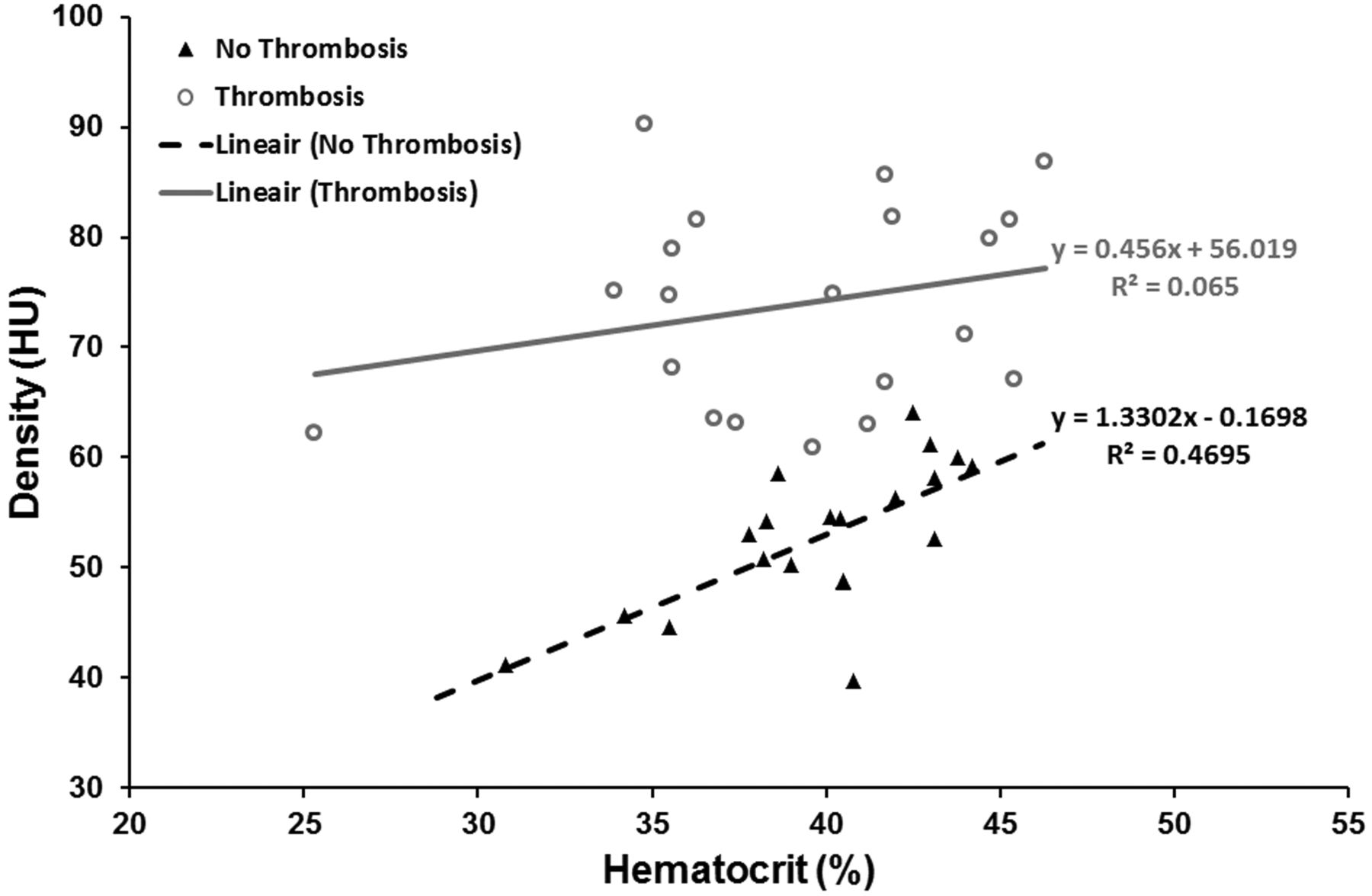
Regression analysis showed a significant positive correlation between attenuation values and HCT in patients without CVST (R2 = 0.47; P = .0009), but not in patients with CVST (R2 = 0.07; P = .28) (Fig 5). The H:H ratio showed values of 1.33 ± 0.12 in patients without thrombosis, and 1.91 ± 0.32 in patients with thrombosis (P < .0001). The receiver operating characteristic analysis of the H:H ratio showed an area under the curve of 0.995 and an optimal cutoff value of 1.52, leading to a sensitivity of 95%, specificity of 100%, and accuracy of 97.5%.

Scatterplot of venous sinus attenuation as a function of HCT showing a significant positive correlation between HCT and attenuation values in patients without acute CVST (R2 = 0.47; P = .0009), but not in patients with CVST (R2 = 0.07; P = .28).
Discussion
Hyperattenuating signs are observed on unenhanced CT scans when an acute thrombus has formed in a blood vessel. It can be seen in various vascular diseases, including cerebral infarction; pulmonary thromboembolism; aortic dissection with a thrombosed false lumen; deep venous thrombosis; and, of course, CVST.8⇓–10 The increase in attenuation is caused by clot retraction, eliminating water and thereby raising the concentrations of red blood cells and hemoglobin. This mechanism results in increased attenuation of the thrombus to 60–90 HU. As time passes, the thrombus ages and is rechanneled so that the red blood cells and hemoglobin are degraded. Subsequently, the attenuation gradually decreases for approximately 7–14 days, at which point the thrombi cannot be differentiated from normal blood or may even appear hypoattenuating relative to blood.11
Hyperattenuating signs can serve as unique findings indicating an acute stage, at a time when treatment is most likely to be effective and to have a great effect on clinical outcome.10 In CVST, the hyperattenuating sign has been referred to as the (hyper)attenuated dural sinus sign in the literature.7 This sign was originally found in only a minority of patients with cerebral sinus thrombosis, and there were doubts about the value of this sign in routine diagnosis. An earlier study reported a sensitivity of approximately 25%.11 With thinner CT sections, however, this sign was detected much more frequently. A more recent study4 reported a significantly higher sensitivity (64%) of the hyperattenuated dural sinus sign for CVST. The authors included subacute and chronic cases, and it is known that the attenuation of a thrombus decreases as time passes, resulting in possible false-negative imaging findings on unenhanced CT scans.4
Appreciating moderate increases in attenuation by active attenuation measurement within the dural sinuses can be helpful in the detection of acute CVST. We found a mean attenuation of 73.9 HU in thrombosed venous sinuses. This degree of attenuation has also been found in acute clots elsewhere in the body. Cobelli et al9 found similar densities on unenhanced CT scans for acute pulmonary emboli (mean, 74.25 HU; range, 57–93 HU), and Goldstein et al10 found similar densities for acute abdominal venous thromboses (mean, 67.12 HU; range, 53–84 HU). Our findings suggest that a threshold of 62 HU can be used to discriminate patients with acute CVST from those without.
A positive correlation and significant association have been established with both hemoglobin and HCT and attenuation of blood on unenhanced CT scans.12 Patients with anemia have low hemoglobin levels and, therefore, low attenuation of blood. In a similar fashion, in patients with high hemoglobin or HCT (eg, in patients with polycythemia vera or in young children), blood may appear hyperattenuating. These findings have been reported to be the most common cause of false-positive readings in CVST.6
Black et al5 were the first to use the H:H ratio to demonstrate the correlation between hyperattenuation on CT scans and HCT level, and they successfully applied their observations in 8 patients with CVST. Calculating the H:H ratio is especially useful in these situations because it corrects for the abnormal HCT level, thereby limiting the risk for a false-positive or negative interpretation of the sinus attenuation. Black et al5 found mean H:H values of 2.20 in patients with CVST and 1.44 in patients without CVST. In our study, the mean H:H value in the patients with acute CVST was 1.91 ± 0.32 vs 1.33 ± 0.12 in patients without CVST. There is almost no overlap in the distribution of H:H ratio between patients with CVST and those without CVST. On the basis of our findings, an H:H ratio of more than 1.52 suggests a strong likelihood of a clot. Black et al5 suggested a cutoff value of 1.8 as a threshold to suspect the presence of thrombosis. The mean and cutoff value differences between the study by Black et al5 and our study seem to be mostly related to a difference in HCT (on average, 36.425 for the patients with CVST in the study by Black et al5 vs 39.16 for the patients in our study).
The accuracy of the H:H ratio was 97.5% in our study, whereas the accuracy of the HU measurement was 95%. This minor difference indicates that HU alone could be a very good substitute when HCT measurement is not available. A statistical comparison between the H:H ratio and the HU measurement by use of the current dataset is not feasible, as the minor difference would lead to very large required patient counts to find significance.
Some limitations of our study need to be taken into account. Partial volume effects caused by the immediate vicinity of the skull could have resulted in false-positive hyperattenuation of the sinus. Our retrospective study was prone to selection bias. Although all readers were blinded to patient clinical data, the measurements could have been biased by the presence of indirect signs of acute CVST on CT scans, such as a hemorrhagic venous infarct.
Conclusions
Worldwide, brain CT scan is the technique of choice in patients with acute neurologic symptoms because of the easy access and low cost. Therefore, any finding that may improve the sensitivity of this technique to accelerate a diagnosis is welcome.
Unenhanced brain CT scan always had its place in the work-up of a patient with suspected acute CVST. We recommend the additional measurement of the venous sinus attenuation and the calculation of the H:H ratio to increase the sensitivity of this examination in the diagnosis of acute CVST. Our findings suggest that in patients with an attenuation of more than 62 HU, the diagnosis of acute CVST is more likely. If the H:H ratio is more than 1.52, then a high likelihood exists that the finding is of a true acute CVST. Density measurement in the venous sinus and calculation of the H:H ratio will increase the confidence of the radiologist in a setting with only CT being available, and it may help decide on the need for confirmatory CT or MR imaging studies.
In an ideal setting, larger prospective, perhaps multicenter, studies are warranted to further establish the proposed parameter for evaluation of acute CVST. However, given the rarity of the condition, the number of patients with acute CVST in our current study already confirms and partly validates the initial findings of the study by Black et al.5
Footnotes
Disclosures: Vincent Thijs—UNRELATED: Board Membership: Boehringer Ingelheim, *Bayer, *Pfizer, *Medtronic; *Consultancy: Boehringer Ingelheim, *Bayer, *Pfizer, *Medtronic; *Payment for Lectures (including service on speaker bureaus): Boehringer Ingelheim, *Medtronic; *Payment for Development of Educational Presentations: Abbott; *Travel/Accommodations/Meeting Expenses Unrelated to Activities Listed: Boehringer Ingelheim, Medtronic, Comments: Registration and hotel costs paid, but no money was received directly. Philippe Demaerel—UNRELATED: Board Membership: Editor “Diagnostic Neuroradiology” for Neuroradiology.
REFERENCES
- Received September 6, 2012.
- Accepted after revision November 4, 2012.
- © 2013 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}