
Abstract
BACKGROUND AND PURPOSE: DVST is an important cause of ICH because its treatment may require anticoagulation or mechanical thrombectomy. We aimed to determine the frequency of adequate contrast opacification of the major intracranial venous structures in CTAs performed for ICH evaluation, which is an essential factor in excluding DVST as the ICH etiology.
MATERIALS AND METHODS: Two readers retrospectively reviewed CTAs performed in 170 consecutive patients with ICH who presented to our emergency department during a 1-year period to determine by consensus whether qualitatively, contrast opacification in each of the major intracranial venous structures was adequate to exclude DVST. “Adequate contrast opacification” was defined as homogeneous opacification of the venous structure examined. “Inadequate contrast opacification” was defined as either inhomogeneous opacification or nonopacification of the venous structure examined. Delayed scans, if obtained, were reviewed by the same readers blinded to the first-pass CTAs to determine the adequacy of contrast opacification in the venous structures according to the same criteria. In patients who did not have an arterial ICH etiology, the same readers determined if thrombosis of an inadequately opacified intracranial venous structure could have potentially explained the ICH by correlating the presumed venous drainage path of the ICH with the presence of inadequate contrast opacification within the venous structure draining the venous territory of the ICH. CTAs were performed in 16- or 64-section CT scanners with bolus-tracking, scanning from C1 to the vertex. Patients with a final diagnosis of DVST were excluded. We used the Pearson χ2 test to determine the significance of the differences in the frequency of adequate contrast opacification within each of the major intracranial venous structures in scans obtained using either a 16- or 64-section MDCTA technique.
RESULTS: Fifty-eight patients were evaluated with a 16-section MDCTA technique (34.1%) and 112 with a 64-section technique (65.9%). Adequate contrast opacification within all major noncavernous intracranial venous structures was significantly less frequent in first-pass CTAs performed with a 64-section technique (33%) than in those performed with a 16-section technique (60%, P value < .0001). Delayed scans were obtained in 50 patients, all of which demonstrated adequate contrast opacification in the major noncavernous intracranial venous structures. In 142 patients with supratentorial or cerebellar ICH without an underlying arterial etiology, we found that thrombosis of an inadequately opacified major intracranial venous structure could have potentially explained the ICH in 38 patients (26.8%), most examined with a 64-section technique (86.8%).
CONCLUSIONS: Inadequate contrast opacification of the major intracranial venous structures is common in first-pass CTAs performed for ICH evaluation, particularly if performed with a 64-section technique. Acquiring delayed scans appears necessary to confidently exclude DVST when there is strong clinical or radiologic suspicion.
Abbreviations
- AVM
- arteriovenous malformation
- CTA
- CT angiogram
- DVST
- dural venous sinus thrombosis
- ICH
- intracerebral hemorrhage
- INR
- international normalized ratio
- IVH
- intraventricular hemorrhage
- MDCTA
- multidetector CT angiography
- NCCT
- noncontrast CT
Nontraumatic ICH accounts for approximately 10%–15% of cases of acute stroke.1 In an important minority of cases, the ICH has an underlying vascular etiology such as an AVM, an intracranial aneurysm with a purely intraparenchymal rupture, or a DVST. These vascular etiologies have accounted for 13%–65% of ICH cases in recent MDCTA studies, with their frequency depending on clinical and NCCT factors—most important, patient age and ICH location.2–7 At our institution, DVST has been identified as the third most common vascular ICH etiology in both patients younger than 41 years of age (26% of vascular etiologies) and in all adult patients (17% of vascular etiologies) examined with MDCTA.4,6,7 Timely and accurate identification of patients with DVST as the ICH etiology is important because its treatment may require immediate anticoagulation—despite the presence of ICH—as well as potential mechanical thrombectomy.
Because MDCTA is frequently performed emergently to rule out an AVM or aneurysm as the ICH etiology, this technique is optimized for evaluation of the intracranial arterial structures; this practice raises the concern that it is not necessarily optimized for evaluation of the intracranial venous structures. Indeed, there may be a risk of inadequate venous opacification following MDCTA, which may be due to either scan timing or the presence of DVST, with vastly different implications for patient management. However, the extent of this risk is not currently clear, and it may be that some providers accept negative findings on MDCTA as having adequately excluded both arterial and venous ICH etiologies. Indeed, in the future, this dilemma is likely to become more common due to the increasing availability of 64-section CT scanners with faster imaging times. While review of the NCCT to assess associated hyperattenuation is often helpful, its reported sensitivity for the detection of DVST is relatively low (65%).8
The purpose of this study was to determine the frequency of adequate contrast opacification of the major intracranial venous structures during the first-pass CTA performed with either a 16- or 64-section MDCTA technique in patients presenting to the emergency department with ICH. These findings will help determine whether MDCTA can safely exclude DVST as the ICH etiology.
Materials and Methods
Patient Selection
Our study was approved by the institutional review board of our hospital and was conducted in compliance with the Health Insurance Portability and Accountability Act. Informed consent was waived because this was a retrospective study. We conducted a retrospective review of all adult patients who presented to our institution from January 1, 2008, until December 31, 2008, with nontraumatic ICH on an NCCT examination of the head and were evaluated with a CTA of the intracranial circulation within 24 hours of presentation. Medical records were reviewed for patient age, sex, history of hypertension, antiplatelet therapy, admission INR, and final diagnosis. Patients with a final diagnosis of DVST as the ICH etiology were excluded from the study.
Image Acquisition
NCCT and MDCTA acquisitions were performed according to standard protocols on either 16- or 64-section helical CT scanners (LightSpeed; GE Healthcare, Milwaukee, Wisconsin). The NCCT examination was performed by using an axial technique with 120–140 kV(peak), 170 mA, 2-second scanning time, and 5-mm-section-thickness reconstruction. First-pass MDCTA was subsequently performed by scanning from the base of the C1 vertebral body to the skull vertex by using the following parameters: pitch, 0.5; collimation, 1.25 mm; maximal milliampere, 350; kilovolt (peak), 120; FOV, 22 cm; and 65–85 mL of nonionic contrast material administered by power injector at 4–5 mL per second into an antecubital vein with SmartPrep software (GE Healthcare), a semiautomatic contrast bolus−tracking technique that triggered scanning after an opacification of 50 HU above baseline in the ascending aorta was reached.
Delayed MDCTA acquisitions were performed with the same scanning technique as the first-pass scans with the delay time determined by the clinical providers. The resulting 1.25-mm-thick axial source images were digitally archived. The decision to perform MDCTA and to obtain a delayed CTA acquisition was at the discretion of the clinical providers. In general, delayed CTA acquisitions were obtained for the following reasons: 1) to exclude DVST as the ICH etiology, 2) to assess the presence of delayed spot signs,9–12 or 3) to aid in the differentiation between spots signs and aneurysms or AVM in challenging cases.
Image Analysis
First, the NCCTs were reviewed by 2 experienced readers to determine, by consensus, the ICH location and its presumed venous drainage path according to the cerebral venous territories described by Meder et al13 for the supratentorial structures and by Jinkins14 for the infratentorial structures (Table 1).
Presumed venous drainage path according to ICH locationa
Subsequently, the first-pass CTA source images were reviewed by the same 2 readers, blinded to the MDCTA technique (16- or 64-section), to determine, by consensus and qualitatively, the adequacy of contrast opacification within each of the major intracranial venous structures for the purpose of confidently excluding the presence of either partial or complete thrombosis of the venous structure examined. “Adequate contrast opacification” of a venous structure was defined as homogeneous opacification of the structure examined. “Inadequate contrast opacification” of a venous structure was defined as either inhomogeneous opacification (Fig 1) or nonopacification (Fig 2) of the structure examined.

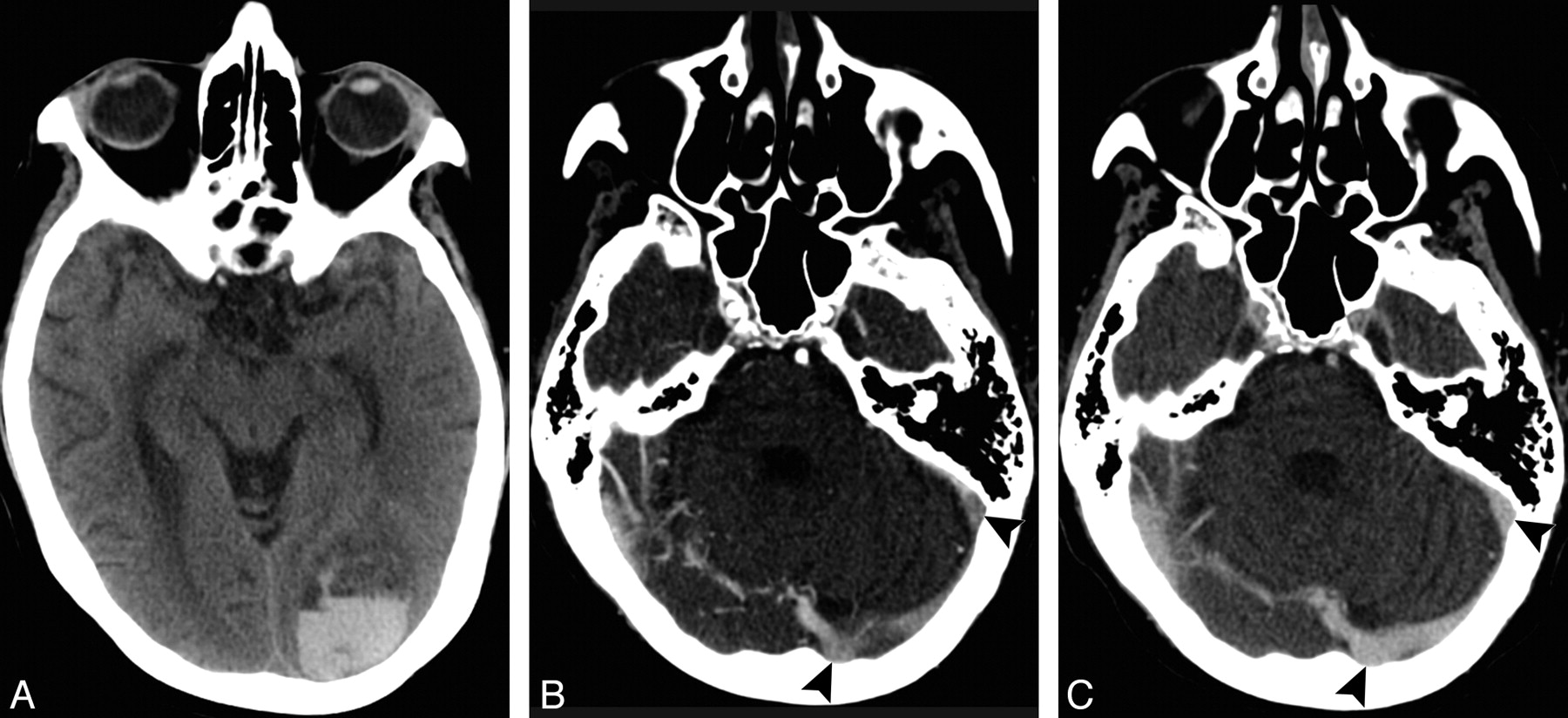
A 57-year-old woman who presented with headache and a right visual field deficit. A, NCCT demonstrates a left occipital ICH. B, Axial source image of a first-pass CTA performed in a 64-section CT scanner demonstrates inhomogeneous opacification of the left transverse and sigmoid sinuses (arrowheads), which may be related to scan timing or partial DVST. C, Axial source image of a delayed CTA acquisition performed 110 seconds after the first-pass scan demonstrates homogeneous opacification of the left transverse and sigmoid sinuses (arrowheads), which excludes DVST as the ICH etiology.

A 65-year-old woman who presented with worsening aphasia and confusion. A, NCCT demonstrates a large left temporo-occipital ICH with intraventricular extension. B, Axial source image of a first-pass CTA performed in a 64-section CT scanner demonstrates nonopacification of the left transverse and sigmoid sinuses (arrowheads), which may be related to scan timing or DVST. C, Axial source image of a delayed CTA acquisition performed 32 seconds after the first-pass scan demonstrates homogeneous opacification of the left transverse and sigmoid sinuses (arrowheads), which excludes DVST as the ICH etiology.
If a delayed CTA acquisition was performed, it was reviewed by the same 2 readers blinded to the first-pass CTA acquisition and MDCTA technique, at least 2 weeks after review of the first-pass CTA, to determine the adequacy of contrast opacification within the major intracranial venous structures according to the same aforementioned criteria.
Finally, in patients who did not have an arterial abnormality as the ICH etiology identified by MDCTA, the same 2 readers determined, by consensus, if thrombosis of an inadequately opacified intracranial venous structure could have potentially explained the ICH. This determination was performed by correlating the presumed venous drainage path of the ICH with the presence of inadequate contrast opacification within the structure draining the venous territory where the ICH was located. This analysis was performed for the first-pass CTA and delayed CTA acquisitions independently. Patients with brain stem ICH were excluded from this analysis because the superior petrosal sinuses were not evaluated for adequacy of contrast opacification.
In addition, ICH and IVH volumes were determined with Analyze 9.0 software (Mayo Clinic, Rochester, Minnesota) by thresholding with manual hematoma outline adjustment in the NCCT examination.
Statistical Analysis
Statistical analysis was performed using MedCalc, Version 11.1 for Windows (MedCalc Software, Mariakerke, Belgium). Using the Pearson χ2 test, we determined the significance between the differences in the frequency of adequate contrast opacification within each of the major intracranial venous structures in scans obtained by using either a 16- or 64-section MDCTA technique. In addition, we used the Pearson χ2 test to determine the significance of the difference between the frequency of scans in which thrombosis of an inadequately opacified venous structure in the first-pass and delayed CTA acquisitions could have explained the ICH comparing 16- or 64-section MDCTA techniques. P ≤ .05 was considered statistically significant.
Results
From January 1, 2008, until December 31, 2008, a total of 176 adult patients presented to our emergency department with ICH on an NCCT examination and were evaluated with a CTA of the intracranial circulation within 24 hours of admission. Six patients were excluded from the study because of a final diagnosis of DVST as the ICH etiology (3.4%). Of note, all of these patients had either inhomogeneous opacification or nonopacification of the thrombosed major intracranial venous structures in the first-pass CTA and, when obtained, in the delayed CTA acquisition as well. Specifically, the diagnosis of DVST was made by the presence of either inhomogeneous opacification or nonopacification of a major intracranial venous structure in the first-pass CTA coupled with the following: 1) persistent inhomogeneous opacification or nonopacification of the venous structure in the delayed CTA acquisition in 3 patients, 2) hyperattenuation within the venous structure on the NCCT in 2 patients, and 3) inhomogeneous opacification or nonopacification of the venous structure at conventional angiography in 1 patient.
Hence, a total of 170 patients met the inclusion criteria of our study, with a mean age of 64.3 years (median, 66.5 years; range, 18–92 years). Ninety patients were men (52.9%) and 80 were women (47.1%). Table 2 summarizes the baseline clinical and radiologic characteristics in our patient population. One hundred twelve patients were scanned using a 64-section MDCTA technique (65.9%), and 58 were scanned using a 16-section MDCTA technique (34.1%). Delayed MDCTA acquisitions were obtained in 50 patients (29.4%), 40 of whom were scanned with a 64-section MDCTA technique (80%) and 10 with a 16-section MDCTA technique (20%). Mean delay time was 95 seconds after the first-pass CTA (median, 57 seconds; range, 10–426 seconds; standard deviation, 30 seconds).
Baseline clinical and radiologic patient characteristics
Frequency of Adequate Contrast Opacification of the Major Noncavernous Intracranial Venous Structures
Table 3 summarizes the frequency of adequate contrast opacification of the major intracranial venous structures in the first-pass CTA, categorized by the MDCTA technique. For major noncavernous intracranial venous structures, there was a significantly higher frequency of adequate contrast opacification in all of the venous structures in the first-pass CTAs performed with a 16-section MDCTA technique (60%) compared with those performed with a 64-section MDCTA technique (33%, P value < .001). However, delayed CTA acquisitions demonstrated adequate contrast opacification in all the major noncavernous intracranial venous structures (100%), regardless of MDCTA technique used (P value 1).
Frequency of adequate contrast opacification of the major intracranial venous structures in first-pass CTAs performed for evaluation of intracerebral hemorrhagea
Frequency of Adequate Contrast Opacification of the Cavernous Sinuses
Pooling the right and left cavernous sinuses, we found a significantly higher frequency of adequate contrast opacification within the cavernous sinuses in patients scanned with a 16-section MDCTA technique (13.8%) compared with those scanned with a 64-section MDCTA technique (6.3%; P value, 0.02). However, in the delayed CTA acquisitions, there was no significant difference in the frequency of adequate contrast opacification within these venous structures in scans obtained with either a 16-section (90%) or a 64-section (80%) MDCTA technique (P = .25).
Frequency of ICHs Potentially Explained by Thrombosis of an Inadequately Opacified Intracranial Venous Structure
MDCTA identified 22 patients with an underlying arterial etiology for the ICH (12.9%, 15 AVMs and 7 aneurysms with purely intraparenchymal rupture). There were 7 patients with brain stem ICH (4.1%, all pontine), 1 of whom had an AVM.
Hence, there were 142 patients with either supratentorial or cerebellar ICH who did not have an arterial etiology for the ICH identified by MDCTA (83.5%). After correlating the presumed ICH venous drainage path with the adequacy of contrast opacification in the first-pass CTA in the major intracranial venous structure draining the venous territory of the ICH, we found that thrombosis of an inadequately opacified major intracranial venous structure could have potentially explained the ICH in 38 patients (26.8%), 33 of whom had been evaluated with a 64-section MDCTA technique (86.8%). Twenty-three of these patients had delayed CTA acquisitions performed (60.5%), all of whom demonstrated adequate opacification within the venous structure in question. After these delayed CTA acquisitions were taken into account, there was a significant decrease in the number of patients in whom thrombosis of an inadequately opacified major intracranial venous structure could have potentially explained the ICH (15, 10.6%, P <.001). Eleven of these patients had been evaluated with a 64-section MDCTA technique (73.3%).
There was a significant difference in the frequency of patients in whom thrombosis of an inadequately opacified major intracranial venous structure in the first-pass CTA could have potentially explained the ICH when comparing the 16-section (10.9%) and 64-section (34.4%) MDCTA techniques (P value = .003). However, this difference was not significant once the delayed CTA acquisitions were taken into account, resulting in a frequency of 8.7% for patients evaluated with a 16-section MDCTA technique and 11.5% in patients evaluated with a 64-section MDCTA technique (P = .43).
Discussion
We have determined the frequency of adequate contrast opacification within each of the major intracranial venous structures in a large cohort of patients with ICH evaluated with MDCTA who did not have a final diagnosis of DVST. These data may serve as a guide for the expected frequency of adequate contrast opacification within the major intracranial venous structures in this patient population, which would be a valuable tool for CTA readers who aim to exclude the presence of DVST as the potential cause of ICH.
Nonetheless, these results are specific to the scanning technique used at our institution, where we use bolus-tracking and scan from the level of the C1 vertebral body to the skull vertex. Indeed, our results for the superficial venous drainage system of the brain are directly related to the direction of our scanning technique: We found much lower frequencies of adequate contrast opacification in the sigmoid and transverse dural sinuses (48%–66%), which are scanned earlier, compared with the superior sagittal sinus (81%), which is scanned later. The particularly low frequency of adequate contrast opacification of the left (36%–54%) and right (42%–58%) transverse and sigmoid sinuses in 64-section CTAs is particularly important, because a recent study by Girot et al15 found that among 245 patients with DVST who initially presented with ICH, 50% had involvement of the left transverse and sigmoid sinuses and 33% had involvement of the right transverse and sigmoid sinuses.
Most important, we found significantly higher frequencies of adequate contrast opacification within all the major noncavernous intracranial venous structures in scans obtained by using a 16-section MDCTA technique compared with scans obtained by using a 64-section technique. These findings are a direct result of the longer time required to scan a patient's head with a 16-section CT scanner (12–15 seconds) compared with a 64-section CT scanner (4–5 seconds), thus allowing more time for opacified blood to reach the venous structures with the former technique. Indeed, in patients without an underlying arterial ICH etiology who were examined with the 64-section MDCTA technique, we found that in 34% of first-pass CTAs, we were unable to confidently exclude DVST as the ICH etiology because there was inadequate contrast opacification within the major venous structure draining the venous territory where the ICH was located. Awareness of this important potential diagnostic pitfall when assessing CTAs for the presence of DVST in this patient population will become increasingly important in the future because medical centers will acquire CT scanners with increasing numbers of detector rows and scanning time will continue to decrease.
Delayed CTA acquisitions are valuable adjuncts when assessing for DVST as the ICH etiology because, in our study, they demonstrated adequate opacification in all major noncavernous intracranial venous structures. These delayed acquisitions were performed between 10 seconds and 7 minutes after the first-pass CTA. Indeed, when we included the results of the delayed CTA acquisitions in the analysis, the number of cases scanned with either a 16- or 64-section MDCTA technique in which we could not confidently exclude DVST as the ICH etiology decreased significantly. A potential alternative strategy to obviate acquiring a delayed CTA acquisition might be to evaluate the NCCT for the presence of hyperattenuation within a venous structure that is inadequately opacified in the first-pass CTA; however, the reported sensitivity of NCCT for the detection of a superficial DVST is low (65%).8 Alternatively, these patients could be subsequently assessed with MR venography to exclude DVST, though this would require performing an additional examination. Thus, in patients with inadequate opacification of a major intracranial venous structure in the first-pass CTA in a distribution that may explain the ICH, the clinical benefit derived from confidently excluding DVST as the ICH etiology should be carefully weighed against the increased radiation exposure incurred from a delayed CTA acquisition, which is similar to that of the first-pass CTA and NCCT examinations (approximately 2.5 mSV at our institution), or the added cost of performing an additional diagnostic examination such as MR venography.
The findings described above reflect the fact that the difference between a CTA and a CT venogram is chiefly the delay time at which images are acquired. At our institution, CTAs are acquired by using bolus-tracking, which typically results in a scanning delay time of 15–25 seconds after contrast injection (depending on the patient's cardiac output), while CT venograms are performed with a fixed 40-second delay from the time of contrast injection. Hence, at our institution, the difference in scanning delay time between a CTA and CT venogram typically ranges from 15 to 25 seconds.
Given the low frequency of adequate contrast opacification within the cavernous sinuses in both 16- and 64-section MDCTA techniques, acquiring a first-pass CTA only is insufficient to assess the presence of cavernous sinus thrombosis. Indeed, in our cohort, not all delayed CTA acquisitions demonstrated adequate opacification of these venous structures. Thus, assessing for this entity may require evaluation with a CT venogram with an extended scanning delay time. However, the frequency of ICH secondary to cavernous sinus thrombosis is likely to be low and would be limited to ICH in a peri-Sylvian or insular distribution.13,15
Most interesting, we found differences in the frequency of adequate contrast opacification between the superficial and deep venous drainage systems in the brain, with the deep venous system being adequately opacified more frequently (85%–88%) than the superficial venous system (48%–81%). These findings may reflect the shorter path followed by opacified blood that ultimately reaches the deep venous drainage system compared with the opacified blood reaching the superficial venous drainage system.
Overall, this study highlights the tremendous value of close communication at the point of care between the clinical providers and the neuroradiology team in the evaluation of this patient population. First, clinical providers should ensure that the neuroradiologist reviewing the images is aware that DVST is one of the differential diagnoses being considered. Second, there is likely a tremendous benefit to be derived from a member of the neuroradiology team rapidly reviewing the first-pass CTA images and determining whether a delayed CTA acquisition is necessary to confidently exclude DVST as the ICH etiology. Such measures would ensure that all necessary testing is performed emergently, while also minimizing radiation exposure and the need for repeat imaging after the patient has been admitted to the hospital.
The limitations of our study are its retrospective design, the qualitative rather than quantitative determination of adequate opacification of the venous structures examined, the unclear clinical significance of diagnosing DVST in patients with ICH, the lack of assessment of the superior petrosal sinuses, the lack of delayed CTA acquisitions in all patients in our cohort, and the variable delay time for the delayed CTA acquisitions. The lack of assessment of the superior petrosal sinuses has led to the inability of our study to assess the venous drainage of the brain stem. In addition, not all patients underwent a criterion standard study such as conventional angiography to exclude DVST, which may have led to an underestimation of the actual frequency of DVST in this patient population.
Conclusions
When MDCTA is performed as part of the ICH work-up, the first-pass CTA may not always demonstrate adequate opacification of the major intracranial venous structures to confidently exclude DVST, particularly if performed with a 64-section technique. Because DVST is the third most common vascular cause of ICH and has significant therapeutic implications, the presence of inadequate venous opacification in the first-pass CTA in a distribution that may potentially explain the ICH should prompt acquisition of a delayed scan to confidently exclude DVST as the ICH etiology.
Acknowledgments
We thank Jonathan Rosand, MD, MSc, for his contribution in the preparation of this manuscript, and Eleni K. Balasalle, BA, for her contribution in the artwork for this manuscript.
Footnotes
-
This work was supported, in part, by the National Institute of Neurological Disorders and Stroke grant K23NS059774.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received July 29, 2010.
- Accepted after revision September 8, 2010.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.