
Abstract
SUMMARY: Giant serpentine aneurysms are fusiform partially thrombosed aneurysms with a separate outflow tract to normal distal cerebral vessels. Three patients with giant serpentine aneurysms of the anterior and middle cerebral arteries were treated with endovascular occlusion of the aneurysmal lumen with coils or glue after balloon test occlusion of the involved vessel. In all 3 patients, leptomeningeal collateral circulation was sufficient to prevent distal ischemia.
Serpentine aneurysms are uncommon fusiform arterial dilations in which the lumen extends longitudinally along the axis and curves of the original artery, creating a serpentine pathway with a separate entrance and outflow tract. Repeating dissection with intramural thrombus formation is proposed as the underlying cause.1–3 Most serpentine aneurysms are giant partially thrombosed lesions with a preferential location in the posterior circulation and on the middle cerebral artery. Clinical presentation is usually by mass effect, seizures, or ischemic symptoms; hemorrhage is rare. Surgical treatment of serpentine aneurysms is technically challenging because distal revascularization is considered required.1–4
In this article, we present 3 patients with giant serpentine aneurysms treated with endovascular intraluminal trapping with coils or glue after selective balloon test occlusion of the involved vessel.
Case Reports
Case 1
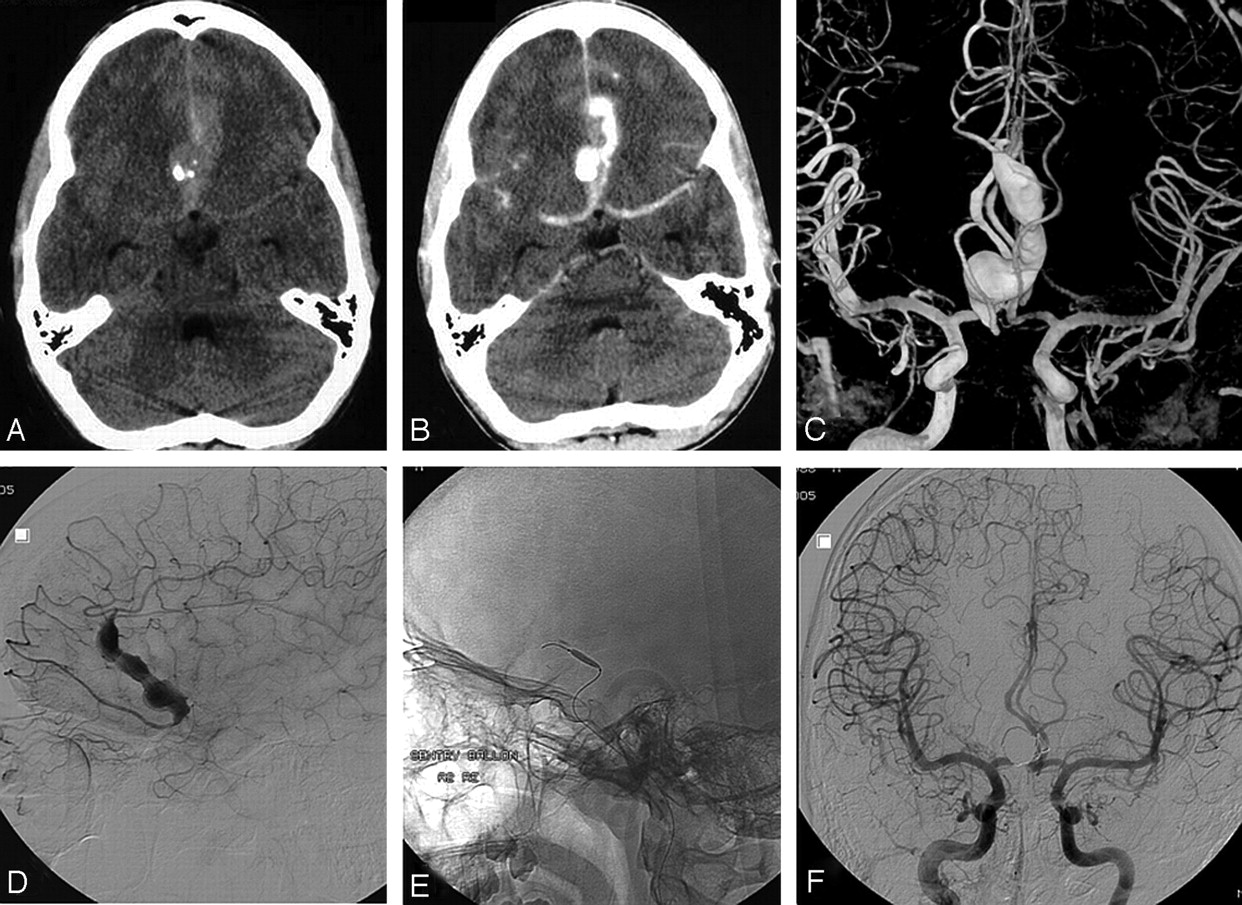
A 16-year-old boy presented with acute severe headache (Fig 1). Apart from drowsiness, no neurologic symptoms were apparent. Native and contrast-enhanced CT scans showed a subarachnoid hemorrhage from a calcified partially thrombosed fusiform aneurysm in the frontal interhemispheric fissure. Bilateral internal carotid artery angiography demonstrated a serpentine aneurysm from the A2 segment of the right anterior cerebral artery. Additional 3D rotational angiography revealed a duplicated right A2 segment with the aneurysm located on the lateral branch. Selective angiography of this segment demonstrated the fusiform nature of the aneurysm, with branches arising both proximal and distal to the dilated segment. Under full heparinization, a nondetachable microballoon (Sentry 15 mm; Boston Scientific, Fremont, Calif) was navigated just proximal to the aneurysm and inflated for test occlusion. For 30 minutes, the patient was repeatedly examined by a senior neurology resident. No clinical symptoms developed, and subsequently the proximal part of the aneurysm was completely occluded with coils (Guglielmi Detachable Coil 18; Boston Scientific). The patient made an uneventful recovery and went back to high school 2 weeks later. A follow-up MR imaging 2 months later showed no infarctions.

A 16-year-old boy presented with acute subarachnoid hemorrhage from a giant serpentine anterior cerebral artery aneurysm. A and B, Native (A) and contrast-enhanced (B) CT scans show subarachnoid hemorrhage from a calcified partially thrombosed fusiform aneurysm in the frontal interhemispheric fissure. C, Bilateral internal carotid artery 3D angiography reveals a duplicated right A2 segment with the aneurysm located on the lateral branch. D, Selective angiography of the aneurysm-bearing segment demonstrates branches arising both proximal and distal from the fusiform dilated segment. E, Microballoon for test occlusion. F, Complete exclusion from the circulation after coil occlusion of the proximal part of the lumen. No infarction developed.
Case 2
A 68-year-old woman presented with several episodes of dysphasia that lasted 5–10 minutes during the previous 2 months (On-line Fig 1). CT showed a multilobular hyperattenuated structure in the left Sylvian fissure. Additional MR imaging suggested a partially thrombosed serpentine left middle cerebral artery aneurysm with various stages of clot formation, confirmed at 2D and 3D angiography. A microballoon (HyperForm; ev3, Irvine, Calif) was positioned just proximal to the dilated segment of the middle cerebral artery branch and inflated for test occlusion. No symptoms developed during the 30-minute test occlusion. The next day, with the patient under general anesthesia, the aneurysm lumen was completely occluded with coils (Trufill Orbit; Cordis Neurovascular, Miami Lakes, Fla). Several hours later, she gradually developed slurred speech that recovered after rapid volume expansion. Repeat T2-weighted MR imaging 2 days later showed several new punctuate white matter hyperintensities in the left parietal region. However, during 3 months of follow-up, she has been free of symptoms with no new episodes of dysphasia.
Case 3
A 51-year-old woman presented with a frontal syndrome, which gradually progressed for 2 years (On-line Fig 2). MR imaging demonstrated a 5-cm giant serpentine aneurysm in the frontal midline with surrounding edema. Left internal carotid angiography showed the aneurysm to originate from the left anterior cerebral artery with a tortuous luminal channel. With steroid treatment, her functional status improved. A microballoon (Endeavor; Boston Scientific) was positioned in the proximal involved A2 and inflated to occlude its lumen. No symptoms developed during the 30-minute test occlusion. Then, a microcatheter was advanced into the aneurysm, and the luminal channel was occluded with glue (Histoacryl; Braun, Melsungen, Germany). No infarction in the distal anterior cerebral artery territory developed on follow-up MR imaging. Steroid treatment was discontinued without aggravation of symptoms. Ten months later, the thrombosed aneurysm was surgically partially removed.
Discussion
Giant serpentine aneurysms are extremely rare, with an incidence of <0.1%.3 Pathogenesis is assumed by repeated dissection of an intrinsic abnormal vessel wall with intramural hemorrhages.1 Giant serpentine aneurysms may develop from smaller fusiform aneurysms and represent a spectrum of the same pathologic entity.1,2 Clinical presentation is mostly related to mass effect and sometimes to distal ischemia by distal emboli, occlusion of side branches, or direct flow impairment. Hemorrhage is rare. Most giant serpentine aneurysms are located in the posterior circulation and the middle cerebral artery; other locations, including the anterior cerebral artery as in 2 of our patients, are very uncommon.
Characteristic of serpentine aneurysms is the involvement of a length of blood vessel with separate inflow and outflow sites. To prevent distal ischemia, surgical treatment usually includes a bypass procedure with inherent technical difficulties.1–4 However, distal revascularization is not necessary in patients with adequate leptomeningeal collateral supply. With endovascular techniques, it is now possible to perform a selective temporary balloon test occlusion of the involved vessel in the awake patient. If no neurologic deficit develops, it is safe to occlude the aneurysmal lumen with coils,5 balloons, or glue in an endovascular procedure. All 3 of our patients tolerated simple endovascular occlusion well. In our opinion, this is the therapy of choice. Only in patients who do not tolerate test occlusion may sophisticated bypass procedures be considered.
Footnotes
indicates article with supplemental on-line figures.
- Received December 12, 2007.
- Accepted after revision January 10, 2008.
- Copyright © American Society of Neuroradiology





{kind=link}