
Article Figures & Data
Figures
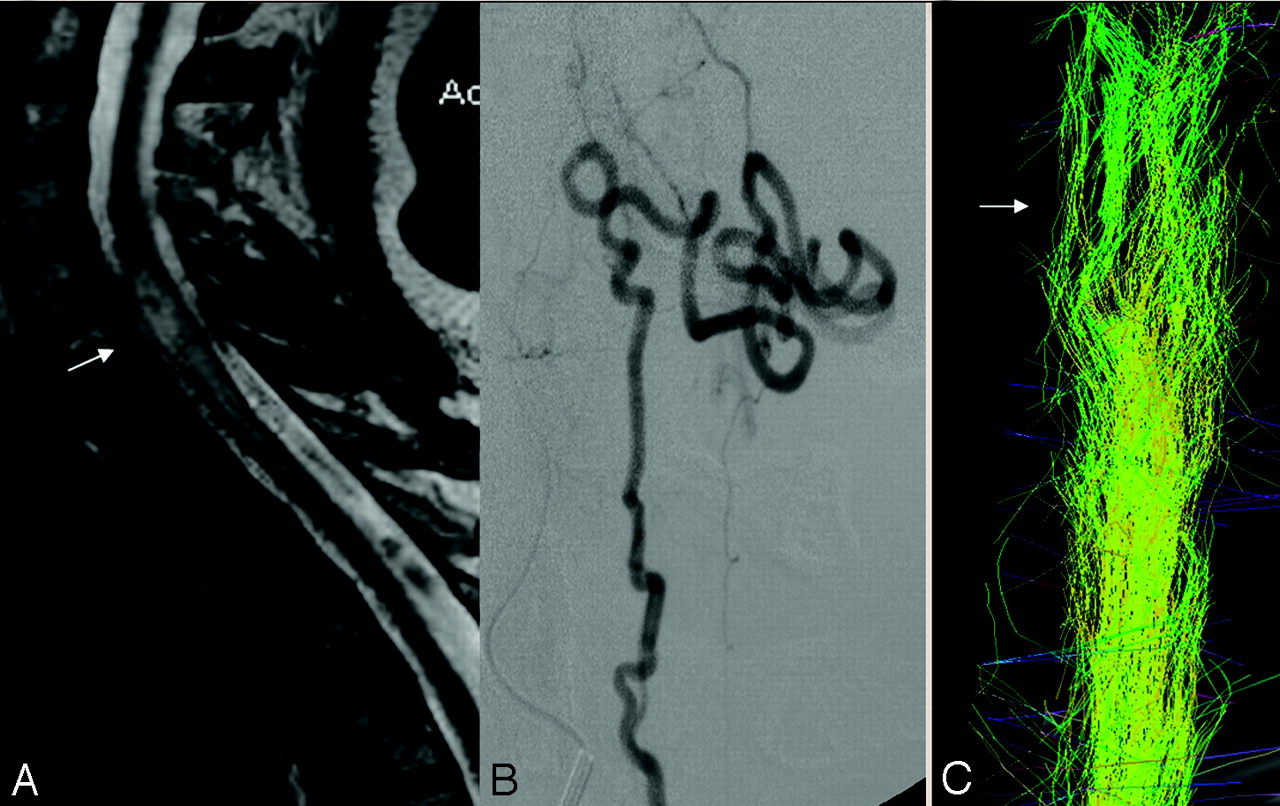
- Fig 1.
Venous congestion of the spinal cord and separated tracts (patient 1, DTI25d). This 57-year-old woman presented with a 2-year history of progressive paresthesia in the bilateral lower limbs, followed by further development of leg weakness and sphincter problems. The McCormick score was II. A pial arteriovenous fistula that was fed by the lateral spinal artery arising from the left posteroinferior cerebellar artery was found.
A, T2-weighted images showed enlargement of the spinal cord at the C6 level with hyperintensity reflecting local venous congestion (arrow).
B, There was a dilated vessel at the anterior surface of the cord, which corresponded with a vein draining the shunt caudally, as depicted on selective injection during angiography.
C, Posterior view of the FT25d showed separated fascicles at the level of C6 (arrow), with global enlargement of the beam of tracts. The remaining fibers were grouped together into fascicles. By counting the tracts at the level of the congestion (674) and below it (741; ratio: lesion level/caudal to lesion = 0.91), we were able to show that there was no evidence of focal interruption of the tracts.
- Fig 2.
Cavity in the cord: thinning of the beam of tracts and separated tracts (patient 2, DTI6d). This 29-year-old woman presented to our service 3 months after she had experienced a sudden complete paraplegia. Subsequently, no clinical improvement was noted.
A–C, The T2-weighted (A and B) and T1-weighted (C) morphologic sequences showed a central cavity within the thoracic cord, an AVM nidus located at T5, and dilated perimedullary vessels mainly cranial but also caudal to the nidus. There was only a moderate enlargement of the cord, which may have been because of the mass effect of the venous pseudoaneurysm.
D, Anteroposterior view of the angiogram showed the venous drainage of the arteriovenous shunt. There was a venous false aneurysm at the level of the nidus that was partially thrombosed as depicted on MR imaging (hyperintensity on both T1 and T2) and surrounded by hemosiderin (hypointensity on T1 and T2), indicating a previous hemorrhage, responsible for her initial symptoms.
E, Posterior view of the FT6d caudal to the nidus (arrow) showed a global thinning but no interruption of the beam of tracts at the level of the cavity in comparison with the normal size of the white matter tracts at C7 (double arrows). The tracts were separated from the midline but still grouped into fascicles.
- Fig 3.
Nidus and segmental interruption of tracts (patient 3, DTI25d). A 23-year-old man presented with bilateral upper limb paresthesia, predominantly on the right side with a sensory deficit. MR imaging showed edema of the cervical spinal cord around the cervical AVM nidus at C2-C3, without any sign of hemorrhage. Angiography revealed a nidus inside the right hemicord, posteriorly located, fed by the pial network arising from the right vertebral artery. First embolization was followed by a clinical improvement of the right upper limb and regression of the T2 hyperintensity on MR imaging. A second session of embolization was performed 1 year later.
A, The third (and last) angiogram performed 3 years 9 months after the onset of the symptoms was not followed by embolization.
B, MR imaging performed at that time with DTI showed T2-hyperintensity inside the inferior part of the nidus corresponding with the embolized part of the nidus.
C, FT25d showed segmental interruption of the tracts of the right posterior column (arrowhead) as could be verified by counting the tracts at the level of the lesion (681) and below it (1017; ratio: lesion level/caudal to lesion = 0.67). The remaining tracts of the lateral column and the midline were slightly shifted showing a mild mass effect on the midline.
- Fig 4.
Nidus at the surface of the cord shifting the tracts (patient 5, DTI25d). A 14-year-old boy presented 4 months after he experienced a sudden paraplegia, which secondarily completely resolved (McCormick I).
A–C, MR imaging showed a nidus located close to the right surface of the thoracic cord, at the level of T8-T9. On these T2-weighted images, no hyperintensity of the cord was visualized.
D shows the anisotropy that, because of the small remaining volume of the cord at that level, cannot be determined.
E demonstrates displacement of the beam of fibers to the right without focal interruption (FT25d). Distal to the nidus, the fibers seem to be more separated compared with the proximal part, which may indicate an increased water content of the cord that is not yet visible on T2-weighted images as edema, which in fact suits the decreased FA values that were found in this area (Table 2).
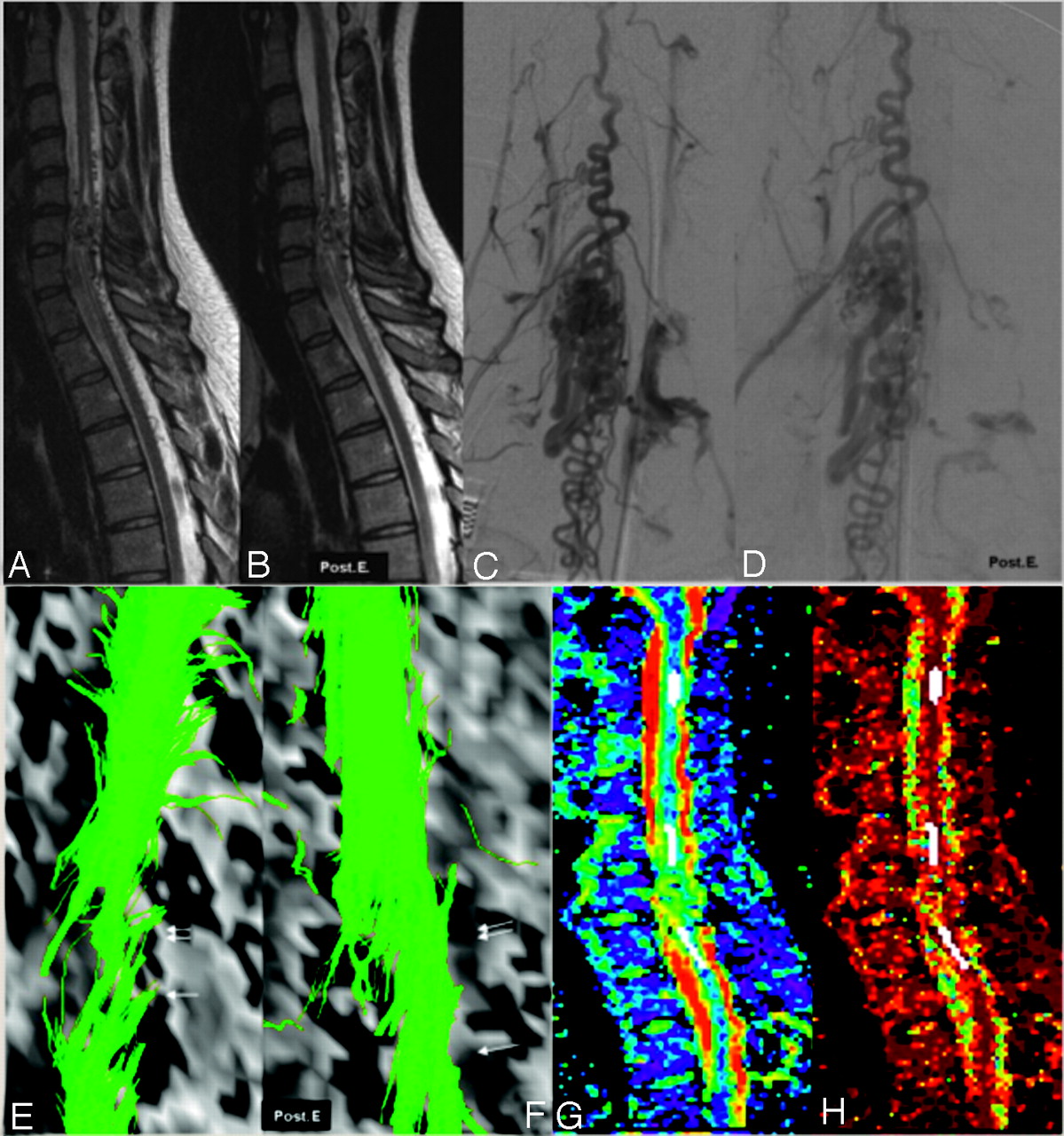
- Fig 5.
Increase of the tracts (FT6d) after embolization (patient 6, DTI6d). A 21-year-old woman with cervical spinal cord arteriovenous malformation first presented with a sudden tetraplegia when she was 12 years old. The neurologic status gradually improved (the McCormick score was grade I at the time of referral to our hospital). MR imaging, angiograms, fiber tracking before (A, C, and E) and after embolization (B, D, and F), and FA and ADC images (G and H) are shown.
At the level of the nidus (arrow), located within the cord, there was partial discontinuity of the tracts (E). Above and below the nidus, conventional T2-weighted images (A,B) showed a central cavity in the cord. Here, FT6d showed both a global thinning of the beam (double arrow in E) and separated tracts around the central cavity. When we compared the evolution after embolization, angiography demonstrated decrease of flow inside the nidus and the draining veins (D). T2-weighted images did not show any modification of the appearance of the perinidal cord. The FT6d showed (F) an increased number of tracts at the level (arrow) and just above (double arrow) the nidus, presumably due to a reduction of venous congestion with concomitant higher FA values and therefore better visualization of fiber tracts. Panels G and H demonstrate the FA values and the ADC map with the ROI placements (white areas) at 3 different levels.
- Fig 6.
Hemorrhage in the spinal cord (patient 7, DTI6d). An 18-year-old male patient presented with a sudden paraplegia because of hemorrhage in a thoracic AVM. When he was admitted 3 months later, the neurologic status was the same (McCormick IV).
A, MR imaging showed a nodular heterogeneous signal intensity inside the thoracic cord at the T2 level, corresponding with the point of bleeding.
B, The cord hemorrhage was located in the vicinity of the nidus that harbored an associated arterial aneurysm in the anterior sulcus of the cord with concomitant mass effect on the anterior spinal artery (arrow). An associated T2 hypointensity corresponding with hemosiderin was located at the anterior part of the cord and spread cranially to the midbrain and caudally to T4 level.
C, FT6d showed an interruption of all of the tracts at the T2-level (arrow), presumably because of susceptibility artifacts related to hemosiderin.






Tables
Patients Age (Years)/ Sex Presenting Symptoms Time Elapsed between Onset of Symptom and Imaging Clinical Status before Imaging McCormick Score Level of the Nidus MR Hyperintensity T2 Hemorrhage 1 57/F Progressive paresthesia followed by motor weakness of lower extremities 18 months Sensorimotor deficit of lower extremities II N.A. (peri-medullary fistula) C5-C7 − 2 29/F Paraparesis developed within 48 hours 4 months Paraparesia and sphincterian deficit IV T5 T3-T6 + 3 23/M Paresthesia of superior limbs 3 months Paresthesia of superior limbs I C2-C3 − − 4 19/M Paresthesias of all extremities 3 years Normal I C1 − − 5 14/M Transitory paraplegia 4 months Dorsalgias I T8-T9 − − 6 21/F Acute tetraplegia 8 years Paresis and paresthesias of right inferior limb I C6 C4-C5 − 7 18/M Paraplegia developed within 24 hours 6 months Paraplegia and sphincterian deficit IV T2 − + 8 35/F Acute hemiparesis 2 years Hemiparesis II C2-C3 − − 9 13/M Acute hemiparesis 2 years Hemiparesis II C5-C7 C3-T2 − Note:—F indicates female; M, male. McCormick clinical functional score: grade I: neurologic examination normal or mild deficit without impairment of the function of any limb and normal walking; grade II: sensitivomotor deficit of limbs and/or severe pains and/or sensitive deficit responsible of an impairment of the quality of life but compatible with independent and self-sufficient walking; grade III: severe sensitivomotor deficit of inferior limbs, enabling not walking anymore, or disabling sensitivomotor deficit of the superior limbs with or without loss of self-sufficient walking; and grade IV: deficit of inferior and/or superior limbs responsible for a total dependence.
- Table 2:
FA and ADC values, qualitative assessments, and angiomorphology in the 9 investigated patients
Patient ROI Placement T2 Hyperintensity FA Z-FA ADC (10−3) Z-ADC Qualitative Results AVM Type and Comments 1 C6 + (congestion) 0.42 −11.83* 55 −0.34 Separated Perimedullary pial fistula fed by the lateral spinal artery; no measurement at the level of the nidus possible because no nidus-type arteriovenous shunt was present (fistulous AVM) T5 − 0.73 −0.25 736 −2.02* Normal 2 C5 0.64 −3.77* 938 −0.47 Normal Glomerular intramedullary AVM fed by radiculopial and radiculomedullary arteries, false aneurysm, and signs of previous intramedullary hemorrhage present; measurements at the level of the nidus not possible because of artifacts from previous hemorrhage; measurements distal to the nidus not possible because of limited FOV T2 + (cavity) 0.49 −9.21* 787 −1.63 Separated T4 + (cavity) 0.36 −14.18* 1196 1.51 Separated Nidus T5 Partially interrupted 3 C1 − 0.70 −1.50 862 −1.06 Normal Glomerular intramedullary AVM fed by the radiculopial network by posterolateral spinal arteries predominantly from the right side; measurement at the level of the nidus not possible because of previous embolization with glue and subsequent artifacts at that level Nidus C2–3 Partially interrupted C4 − 0.77 1.25 801 −1.53 Normal C6 − 0.79 1.78 715 −2.11* Normal 4 Nidus C1 0.59 −5.55* 1113 0.87 Separated Glomerular intramedullary AVM fed by radiculopial arteries; measurement cranial to the nidus not possible because of brain stem location C2 − 0.76 0.65 946 −0.42 Normal C7 − 0.78 1.63 767 −1.79 Normal 5 T6 − 0.78 1.58 1011 −0.01 Normal Glomerular extramedullary AVM fed by radiculopial arteries; measurement at the level of the nidus not possible because of small remaining size of the cord T8 − 0.77 1.16 859 −1.08 Normal Nidus T9 Shifted T10 − 0.64 −3.57* 951 −0.38 Normal 6 C2 − 0.64 −3.59* 873 −0.97 Normal Glomerular intramedullary AVM fed by the anterior and posterolateral spinal arteries; measurement at the level of the nidus not possible because of small remaining size of the cord C5 + (cavity) 0.36 −14.12* 1451 3.47* Separated Nidus C6 Partially interrupted C7 + (cavity) 0.49 −9.25* 1380 2.93* Separated T3 − 0.67 −2.50* 915 −0.65 Normal 7 C2 − 0.62 −4.45* 1139 1.07 Normal Glomerular intramedullary AVM fed by the anterior spinal artery with an associated aneurysm that arose from a sulcal artery and concomitant hemorrhage within the cord; measurement at the level of the nidus not possible because of artifacts because of blood degradation products C4 − 0.65 −3.48* 1152 1.18 Normal T1 − 0.50 −8.72* 1077 0.60 Partially interrupted Nidus T2 Completely interrupted T3 − 0.55 −6.88* 1014 0.11 Partially interrupted Note:—AVM indicates arteriovenous malformation; FA, fractional anisotropy; ADC, apparent diffusion coefficient.
* These values are statistically significantly different from the normal volunteers whose mean values were 0.748 with a range of 0.7–0.8 for FA and 1.00 10−3 with a range of 0.77–1.25 10−3 for the ADC.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.