
Abstract
BACKGROUND AND PURPOSE: Our aim was to evaluate the relationship of pain reduction, after intradiskal lidocaine administration during provocation lumbar diskography, to the presence of contrast leakage on postdiskographic imaging.
MATERIALS AND METHODS: Intradiskal lidocaine was injected at 182 significantly painful disk levels in 111 patients. The clinical records and imaging studies were reviewed for response to the lidocaine injection and for the presence/absence of diskographic contrast leakage on postdiskographic images and CT. Pain response was assigned the following grades: 1) complete or substantial improvement, 2) partial improvement, or 3) no significant improvement after lidocaine administration. Fluoroscopic imaging and postdiskographic CT were evaluated for the presence or absence of contrast leakage.
RESULTS: Eighty-two (45%) significantly painful treated disks were contained, and 100 (55%) demonstrated contrast leakage. In leaking disks, 74 (74%) demonstrated complete or near-complete pain reduction after lidocaine administration, 15 (15%) demonstrated partial improvement, and 11 (11%) demonstrated no pain relief. In contained disks, 56 disks (69%) demonstrated no improvement after lidocaine administration, 9 (11%) demonstrating partial relief, and 17 (20%) demonstrated complete or substantial improvement. Results comparing leaking disks versus contained disks and complete versus no improvement were statistically significant (P < .001).
CONCLUSION: Painful disks exhibiting diskographic leakage tend to be highly responsive to intradiskal lidocaine administration, whereas painful disks without diskographic leakage tend not to improve. This observation has implications with respect to targeting the origin of a patient's back pain and may have specific implications with respect to choice of treatment.
Lower back pain (LBP) is a common problem, which typically resolves with conservative management. In the event that LBP persists, effective treatment requires accurate targeting of the intrinsic cause with appropriate application of specific management options. Major sources of LBP include the facet joints, sacroiliac joints, vertebrae, disks, and muscular spasm.1–4
Initially thought to be inert and insensate, the intervertebral disk is considered a recognized source of LBP.4,5 Concordant pain has been provoked from the annulus, epidural structures, and dura at laminectomy performed under local anesthesia, and innervation of the annulus as well as surrounding structures has been established.1,5–8 Disk challenge by provocation diskography can reproduce a patient's familiar LBP (diskogenic pain) possibly due to stretch of the injured annulus or ligament, irritation of the adjacent vertebral endplate, or leakage of the inflammatory by-products of disk degeneration.5
In general, MR imaging is most effective at identifying abnormal features of a disk, including altered hydration/matrix, disk morphology, and adjacent inflammatory endplate/vertebral changes and loss of height, but these features do not reliably predict the painful disk.9–12 Studies have suggested that when MR imaging demonstrates a focal high-intensity zone in the posterior margin of the disk, the likelihood of LBP generated by that disk is high.13,14 CT, myelography, and routine radiography can identify abnormal-appearing disks but are also unable to establish which disk space is painful.15,16
Lumbar diskography is a long-standing provocative technique, which, by nature of direct disk stimulation, can identify the painful and concordant disk.5,9–28
A previous report on cervical diskography suggested that the response of a painful disk to local anesthetic can predict the response to cervical diskectomy.29 We routinely administer lidocaine to significantly painful lumbar disks during diskography to relieve the induced pain and allow more effective study of subsequently evaluated levels. Although pain relief was frequently observed, in many instances—in particular in contained disks—the patient's pain was not improved or would worsen with local anesthetic application.
In this study, we retrospectively evaluated the relationship of pain reduction after intradiskal lidocaine administration during provocation lumbar diskography with the presence or absence of diskographic contrast leakage as identified on diskographic images or postdiskographic CT.
Materials and Methods
During a 13-month period, 130 consecutive patients had provocation lumbar diskography at our institution by 1 of 2 experienced spine interventional neuroradiologists. Eighty-seven patients were men and 43 were women (average age, 41 years; range, 22–64 years). Patients typically presented with long-standing severe LBP unresponsive to conservative management and were referred by spine-focused orthopedic surgeons or neurosurgeons for preoperative planning. Severe LBP was accompanied by radiating hip or gluteus pain in 10% and leg pain in 50% of patients. Twenty-eight of 130 patients had undergone prior lumbar surgery.
In 111 of the 130 patients, 1 or more significantly painful disks were encountered, and intradiskal lidocaine was injected to reduce or eliminate the patient's provoked pain. Nineteen patients were not included (normal diskogram, n = 5; volume limitation to lidocaine injection at all painful levels, n = 5; pain only at cage fused levels, n = 4; lidocaine not administered, n = 2; and uninterpretable provocation response, n = 3).
Provocation diskography was performed at 350 levels in these 111 patients. At 182 disk levels, severe pain was provoked (concordant, 154 levels; nonconcordant, 28 levels) during disk evaluation, and intradiskal lidocaine was injected for pain control. Unoperated (L5-S1, 64; L4-5, 53; L3-4, 24; L2-3, 6; L1-2, 1; T11-12, 1) and previously operated levels (L5-S1, 16; L4-5, 17) were both studied. These 182 disk levels form the basis of this report. Severe LBP was encountered at a single level in 53 patients, 2 levels in 46 patients, 3 levels in 11 patients, and 4 levels in 1 patient. Leg or hip pain accompanied the provoked LBP in 15% of patients.
Intradiskal lidocaine was not administered in the remaining 168 levels (normal, 126; mild nonconcordant diskomfort, 30; volume limitation to lidocaine injection or extensive venous filling on disk contrast injection, 12).
Institutional review board approval was obtained for this retrospective study.
Lumbar Diskography Technique
Diskography was performed in a standard fashion after appropriate informed consent. The patient's pain history, including leg-versus-back pain contribution, was clarified, and the most-severe-versus-immediate preprocedural pain level was documented using the 0–10 visual analog scale (VAS). Limited intravenous conscious sedation (fentanyl, 0.05 mg; midazolam [Versed]), 1 mg) was given before the procedure with a dose of fentanyl typically given at the end of the examination. Administration of additional fentanyl during the examination was necessary only on rare occasions when disk provocation resulted in extremely severe patient pain that was not responsive to intradiskal anesthetic, and the level of consciousness was never affected. Supplemental administration of additional conscious sedation during the diskography was generally avoided. The lower lumbar region was cleansed and draped, trajectory to target disk space was identified with C-arm fluoroscopy (OEC Series 9800; GE Healthcare, Milwaukee, Wis), and local anesthetic was applied. Disk access was achieved employing a double-needle technique using a 20-gauge guiding spinal needle followed by a curved long 25-gauge spinal needle into the center of the disk space. All needles were placed concordantly opposite the side of leg pain before individual disk injection. Anticipated normal/control disk level was typically studied first.
Disk spaces were studied and provoked by a moderate-to-rapid hand injection of 1.5- to 4.5-mL iohexol, 240 mg Iodine/mL, delivered by a 3-mL syringe and a small 0.6-mL-volume connection tube under direct fluoroscopic guidance. Injection volume was dependent on 1) disk-volume end point, 2) clearly established severe pain response, or 3) exaggerated capacity in degenerative disks. Patients were kept unaware of whether a level was being provoked or which level was being studied. Response to injection was initially observed by the operator, and with a positive pain response, the features of the pain were clarified, VAS level of pain was established, and these items were recorded in a manner similar to the technique of Walsh et al.27 Concordant pain was recorded if the provoked pain was the patient's typical or familiar pain, and nonconcordant pain was recorded if the provoked pain was not the typical pain. Fluoroscopic spot film imaging was obtained for each disk level in anteroposterior and lateral projections during and following the injections.
During disk testing, the patient's immediate response to injection, response to injection end point (if present), and perception of provoked pain (concordant or diskordant) were the primary focus of the diskographer. Syringe disk pressures were not recorded during injection.
If a significantly painful disk space (typically VAS ≥7, concordant or nonconcordant) was encountered, preservative-free lidocaine (2% strength, 1- to 1.5-mL lidocaine (Xylocaine-MPF) was injected into the disk in an attempt to reduce the patient's provoked pain and to allow response clarity in subsequently studied lumbar levels.
The patient was routinely questioned regarding any pain reduction; after administration of the intradiskal lidocaine, the response was recorded as either 1) complete or near-complete pain relief, 2) partial pain relief, or 3) no significant pain relief or as a specific VAS-grade reduction from the pain generated by disk provocation relative to the baseline pain, depending on patient's ability to express the change. Responses initially reported with the VAS were converted to the 3-point scale by calculating the percentage of pain reduction relative to baseline VAS pain level (>66% pain reduction, complete or near-complete pain relief; 33%–66% pain reduction, partial pain relief; and <33% pain reduction, minimal or no significant pain relief).
Postdiskogram CT (GE Healthcare, Milwaukee, Wis) was obtained in all patients immediately following the diskogram employing bone and soft-tissue algorithms with either direct axial 3-mm-section acquisition or with a spiral technique and 3-mm axial and sagittal reformatting with isotropic voxels.
Imaging and Lidocaine Response Analysis
Diskographic fluoroscopic images with the postdiskographic CT of all significantly painful lidocaine-treated disk spaces were independently and blindly reviewed by 2 neuroradiologists experienced in lumbar diskography. Identification of epidural diskographic contrast leakage was primarily established by assessment of the fluoroscopic images with secondary inspection and correlation with the postdiskographic CT. Significant leakage at the disk margin around the needle-entry site was classified as a true leak, but minimal contrast identified at needle entry only after needle withdrawal was not classified as leakage. Disks were judged as either “contained” (no contrast leaking from the disk space) or “leaking” (epidural contrast leakage from the disk space due to radial tear, combined annular and radial tear, or annular and nuclear herniation), itemized, and tabulated. Discordant judgments were resolved by consensus.
Imaging identification of diskographic leakage in the significantly painful treated disks was compared with the 3-point response to lidocaine administration: 1, complete or near-complete relief; 2, partial pain relief; and 3, minimal or no significant relief.
Statistical Analysis
Statistical analysis was performed by χ2 comparison between complete response and no response to lidocaine in contained and leaking disks and a logistic regression model adjusting for the disk state to compare the 2 diskographers regarding the proportion of responses among patients (SAS release 8.2, SAS Institute, Cary, NC).
Results
The results are summarized in Table 1 and Figs 1–5. Eighty-two of 182 (45%) lidocaine-treated disks were contained disks with 100 (55%) demonstrating diskographic leakage through radial tear, radial and annular tear, or partially herniated annular or nuclear material.

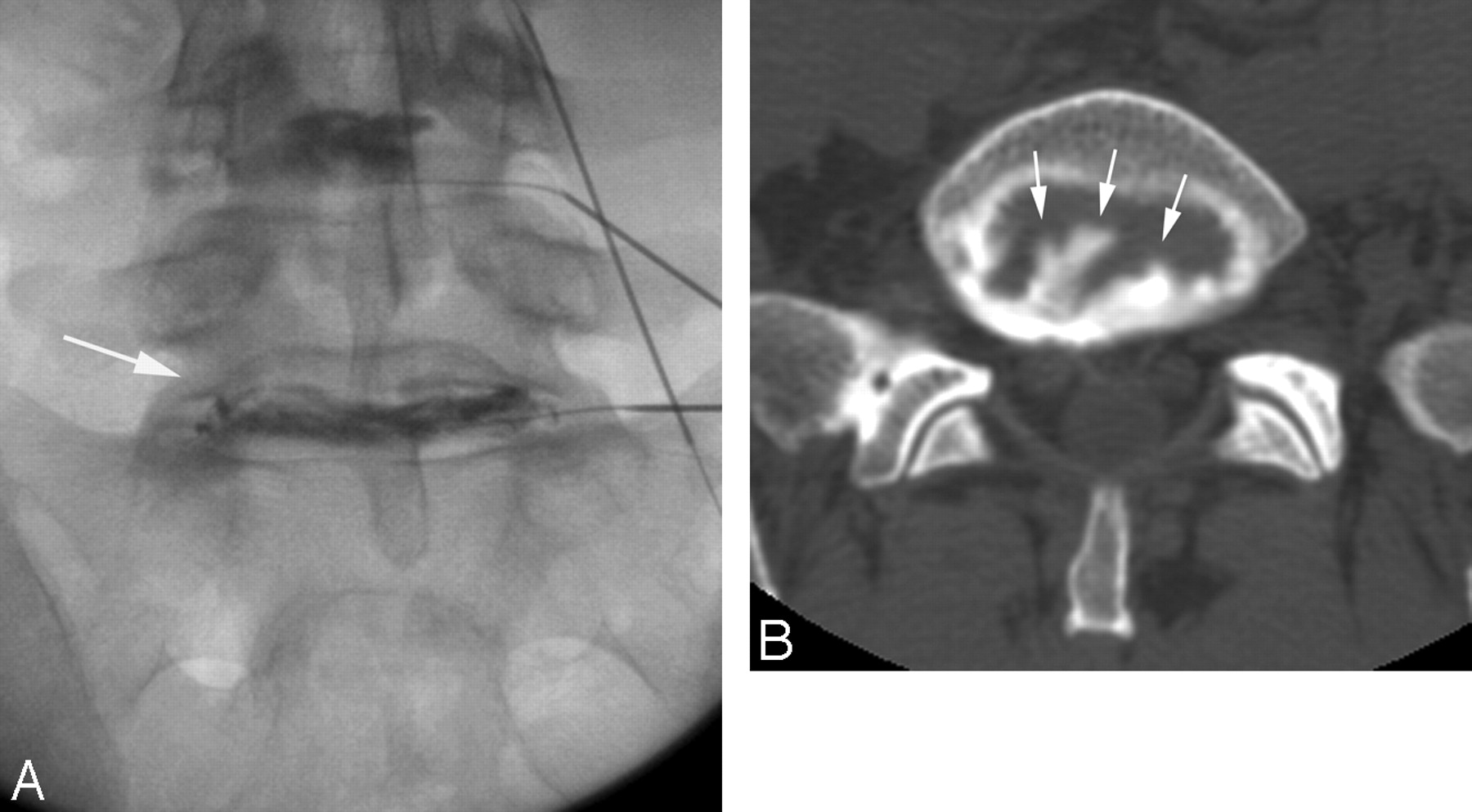
Patient is a 39-year-old man with an injury 20 years ago related to an overturned military vehicle. He has long-standing lower back pain that has recently worsened (VAS score, 8/10). Significant degenerative disk changes are present at L4-5 and L5-S1 on MR imaging, and surgery is now being considered. After 3-mL contrast injection at L5-S1, severe concordant lower back pain was provoked (VAS score, 8/10), with no improvement after 1 mL of intradiskal lidocaine administration.
A, Frontal diskographic fluoroscopic image obtained after contrast injection at L5-S1 demonstrates degenerative changes with nuclear and annular fragmentation (arrow) but no contrast leakage.
B. Axial postdiskographic CT image obtained at L5-S1 demonstrates significant degenerative disk changes with central and peripheral annular tears (arrows) without leakage.
Disk-space response to lidocaine administration: 182 studied lumbar levels
In contained disks, 56 (69%) demonstrated no improvement after intradiskal lidocaine administration (Figs 1 and 2) with 9 (11%) demonstrating partial improvement (Fig 3) and 17 (20%) demonstrating complete or near-complete pain improvement. In leaking disks, 74 (74%) demonstrated complete or near-complete pain relief after intradiskal lidocaine administration (Figs 4 and 5) with 15 (15%) demonstrating partial improvement and 11(11%) demonstrating no significant improvement.

Patient is a 36-year-old man with long-standing back pain and left leg pain (VAS score, 8/10), who had prior diskectomy at L4-5, with only limited improvement. Diskography was requested for follow-up assessment. After 2-mL contrast injection at L5-S1, severe nonconcordant pain was provoked (VAS score, 8/10) with no improvement after 1 mL of intradiskal lidocaine administration. His pain did reproduce concordantly at the diskectomy level.
A, Outside MR sagittal T2-weighted image demonstrates significant degenerative disk changes at L4-5 and L5-S1 (arrowheads) with a high-intensity zone noted along the posterior L5-S1 disk margin (arrow).
B, Lateral diskographic fluoroscopic image obtained after contrast injection at L5-S1 demonstrates degenerative changes (arrow), without evidence of contrast leakage. Contrast dilution was noted throughout the disk after lidocaine administration (not shown), but provoked pain did not improve.
C, Axial postdiskographic CT image obtained at L5-S1 demonstrates a contained radial tear with focal disk protrusion and focal contrast accumulation without epidural leakage (arrow).

Patient is a 50-year-old woman with long-standing lower back pain, not associated with injury (VAS score, 10/10), with an outside MR imaging study demonstrating mild degenerative disk changes at L4-5 and significant degenerative disk changes at L5-S1 but no evidence of disk protrusion. The patient is currently being evaluated further by provocation diskography for potential surgical treatment. After 2.5-mL contrast injection at L5-S1, her severe and concordant lower back pain reproduced (VAS score, 9–9.5/10). Partial improvement in her concordant pain occurred after intradiskal administration of 1-mL lidocaine.
A, Frontal diskographic fluoroscopic image obtained after contrast injection at L5-S1 demonstrates fragmentation and degenerative changes of both nuclear and annular components (arrow), without evidence of contrast leakage.
B, Axial postdiskographic CT image at L5-S1 demonstrates degenerative disk changes with fragmentation and tears of the annulus (arrows) but without any epidural contrast leakage.

Patient is a 40-year-old man with long-standing severe lower back pain (VAS score, 10/10) and some leg diskomfort, without specific injury or trauma, with an outside MR imaging study that demonstrated degenerative disk changes at L4-5 and L5-S1. He was being considered for surgical intervention, and diskography was requested. After 3-mL contrast injection at L4-5, the patient developed severe and concordant pain (VAS score, 10/10). Injection of 1.5-mL lidocaine into this painful disk resulted in complete or near-complete elimination of the provoked pain.
A, Lateral diskographic fluoroscopic image at L4-5 demonstrates degenerative disk changes (arrow) with clear contrast leakage extending into the epidural space (arrowheads).
B, Axial postdiskographic CT image at L4-5 demonstrates complex degenerative changes with both nuclear fragmentation and annular tears (arrow) and a small disk protrusion and focal leakage of contrast into the adjacent epidural space on the left (arrowhead).

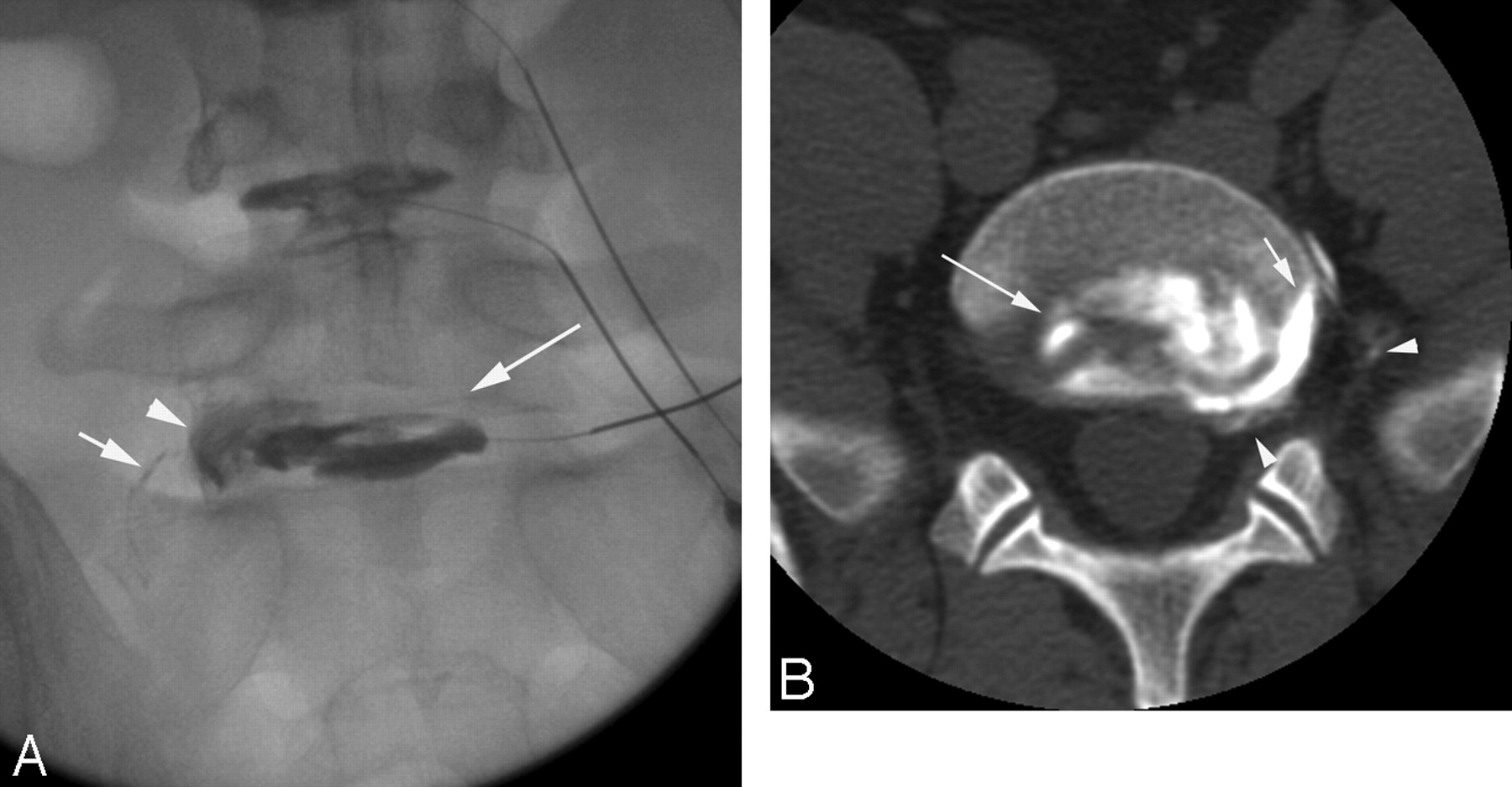
Patient is a 35-year-old man with long-standing lower back pain along with minor leg diskomfort, experiencing increasing pain during the past year. Outside MR imaging demonstrated significant degenerative changes at L4-5 and L5-S1, with possible spondylolysis of L5. Currently, he claimed the back pain would “bring him to his knees” (VAS score, 10/10), and diskography was requested in consideration of surgical intervention. After 3-mL contrast was injected at L5-S1, severe and concordant LBP was provoked without leg pain (VAS score, 10/10). Injection of 1-mL lidocaine resulted in complete elimination of his provoked back pain.
A, Frontal diskographic image at L5-S1 demonstrates degenerative disk changes with annular tears and fragmentation (arrow), along with a peripheral annular tear projecting over the left foraminal disk margin (arrowhead) and focal leakage into the foramen and far lateral region (short arrow).
B, Axial postdiskographic CT image demonstrates internal annular tears and fragmentation (arrow) and a peripheral annular tear on the left (short arrow), with leakage into the epidural space, L5-S1 foramen, and far lateral region (arrowheads).
Overall, 91 of 182 (49%) disks demonstrated complete or near-complete improvement after intradiskal lidocaine administration with 24 (13%) demonstrating partial improvement and 67 (37%) demonstrating no significant improvement. Of disks that demonstrated complete or near-complete improvement, 74 of 91 (82%) were diskographic leaking disks and only 17 (18%) were contained disks. Of disks that demonstrated no significant improvement after intradiskal lidocaine administration, 56 of 67 (84%) were contained disks and 11 (16%) were diskographic leaking disks. In the 58 patients with 2 or more significantly painful levels, 33 (57%) had a combination of both leaking and contained painful disks.
Assessment between complete relief versus no significant improvement after intradiskal lidocaine in leaking disks versus contained disks (Table 1, data columns 1 and 3) was statistically significant (χ2, P < .001). Interinterpreter difference was not detected by logistic regression (P = .31).
Results separating postoperative and nonpostoperative disks are summarized in Tables 2 and 3. Leaking disks demonstrated complete or near-complete improvement after lidocaine administration more frequently than contained disks in both postoperative levels (P = .009) and nonpostoperative levels (P < .001), similar to that of the overall study population.
Disk-space response to lidocaine administration: 33 postoperative levels
Disk-space response to lidocaine administration: 149 nonoperative levels
Regarding postoperative disks, 17 of 33 (51.5%) were contained disks, and 16 were leaking disks (48.5%). A greater fraction of painful postoperative disks demonstrated no significant improvement after intradiskal lidocaine administration (17 of 33 [51.5%], Table 2). This trend was seen in both leaking (4 of 16 [25%]) and contained (13 of 17 [76.5%]) postoperative disks. Results in the nonoperative disks paralleled the overall patient results (Tables 1 and 3).
Discussion
LBP is a significant and expensive health care problem. Sources of LBP include the facet, sacroiliac joints, intervertebral disk, vertebral injury or destruction, muscle spasm, and instability. Clearly, accurate targeting of the cause of LBP is crucial to proper application of appropriate treatment options.
Although this finding was initially controversial, the intervertebral disk is recognized as a source of LBP, with several different mechanisms (stretch of the annulus, pressurization of the endplate, and chemical irritation) considered potentially responsible.5 Free nerve endings, presumably pain fibers, have been identified in the peripheral annulus and posterior longitudinal ligament (PLL) as well as in the adjacent dura, epidural vessels, and anterior longitudinal ligament.30–38 Probing or stimulation of clinically painful disks clearly provokes a painful response when tested during laminectomy with the patient under local anesthesia.6–8 Familiar pain can be reproduced in contained disks during provocation diskography, likely related to stretch of the annulus or stimulation of the adjacent vertebral endplates.5,39 Disk material can also induce inflammation and chemical irritation; nociceptive stimulation could develop at the annular/ligamentous margin or epidural/dural structures secondary to leakage of degenerative disk by-products.40–48
Although imaging can identify abnormal-appearing disk spaces and help point to the cause of LBP or radiculopathy, provocative diskography is critical for confirming a painful disk and in particular for identifying the concordant painful disk levels in an individual patient.
Our results demonstrate several important observations with regard to the painful lumbar disk: 1) Most painful contained disks are unresponsive to intradiskal lidocaine administration, 2) some painful contained disks respond to intradiskal lidocaine, demonstrating partial or complete pain resolution, 3) most painful disks with diskographic leakage demonstrate complete or near-complete improvement after intradiskal lidocaine administration, and 4) some painful leaking disks demonstrate only partial or no pain improvement after intradiskal lidocaine. Pain improvement after lumbar intradiskal anesthetic administration has been occasionally mentioned in the diskography literature but, to our knowledge, never comprehensively assessed.49,50 These observations may suggest several different and frequently overlapping causes of diskogenic LBP.
Contained Painful Disks: No Relief
In 69% of painful contained disks, intradiskal lidocaine administration resulted in no significant improvement in their provoked pain (Figs 1 and 2). Despite the degenerative fluoroscopic and postdiskographic CT imaging appearances, pain relief was not achieved when these internal deranged surfaces (disk degeneration, annular degeneration, and annular tears) were bathed with local anesthetic. LBP in these disks is likely generated peripheral to the internal disk surfaces, perhaps in the peripheral annulus or posterior longitudinal ligament. One could question, in these instances, whether peripheral annular injury was present and not recognizable at imaging.
Contained Painful Disks: Partial or Complete Relief
Complete pain relief was seen in 20% of painful contained disks, and partial pain relief occurred in 11% (Fig 3). This observation strongly suggests that the visualized internal degenerative features are related to pain provocation for that disk level. The existence of pain nociceptive fibers in the disk has been long debated. Free nerve endings suggesting pain fibers have been documented in the peripheral one third of the annulus and PLL, most commonly associated with small penetrating blood vessels.1,31,34,38 Free nerve endings have been observed extending as far as the peripheral half of the annulus in patients with disk herniation.51 Neovascularization and substance P immunoreactive innervation (nociceptive pain-mediator fibers) of the inner one third of the annulus (46%) and nucleus (22%) have been described in operative biopsy of painful disk levels52 and recently reconfirmed with calcitonin gene-related peptide-expressing nociceptor innervation demonstration in the outer and inner annulus of postoperative specimens.53 Local anesthetic action on these annular or nuclear pain fibers could be responsible for the pain resolution or improvement noted in this subset of our patients with painful contained disks.
Painful Disks with Diskographic Leakage: Complete Response
In 74% of painful leaking disks, complete or near-complete resolution of LBP occurred after intradiskal lidocaine administration (Figs 4 and 5). In these lumbar disks, local anesthetic was either reaching the location of the LBP generator or blocking its central neural transmission.
LBP in these patients could be generated at the annular/PLL surface at the radial tear or herniation. Alternatively, irritation of epidural structures (vessels) or dura could be the source of pain and relieved by the local anesthetic. It is well known to diskographers that leaking disks can reproduce severe and concordant LBP after only minimal contrast injection or leakage. Patients are also encountered in whom nonspecific/semiconcordant LBP is provoked with initial disk injection, but exact replication is recognized only when greater contrast volume and pressure are used and focal contrast leakage finally occurs.
The irritant effects and by-products of disk degeneration such as phospholipase A2, substance P, inflammatory cells, and hydrogen ions have been suggested as a source of LBP and radiculopathy.40–48 Unmyelinated fibers (somatic and autonomic) are known to be present in the peripheral annulus/PLL but are also concentrated in epidural blood vessels and the ventral dura. Radiating pain patterns (radiculopathy) at times resemble a nerve root distribution and at times are more indistinct, variable, or referred, perhaps reflecting the distribution of the somatome (somatic and autonomic innervation including dermatome, myotome, and sclerotome), and this distribution has been termed the “radiating zones of head.”2 A vascular pain fiber (epidural, paravertebral vessel, or dural) source of pain fiber irritation and LBP might explain a portion of the response to lidocaine in painful leaking lumbar disks.
Painful Disks with Diskographic Leakage: Partial Response or No Response
The fourth important observation is related to the absent improvement (11%) or partial improvement (15%) to local anesthetic noted in the painful leaking disks. Considering the response of contained disks, it is likely that some leaking disks also have internal derangement or peripheral annular injury as the source of their pain, which does not come in contact with the intradiskal local anesthetic. Absent pain improvement (11%) despite leakage suggests that the leak pathway and leaking substances may not be the pain generator and that pain is being produced elsewhere in the disk. Partial pain improvement (15%) suggests that the leak pathway and leaking products may partially contribute.
Pain origin in leaking disks, therefore, could be related to the visualized internal derangement, peripheral annular margin injury, leakage path, or irritant effects of epidural leakage of inflammatory material. Although a simple epidural anesthetic mechanism of pain extinction could be suggested for relief in the leaking disks, clearly complete pain ablation is not encountered in all instances. In addition, in many leaking disks, the leak is small and focal, and widespread leakage of contrast (and presumably lidocaine) is not present.
We have not embraced injection-pressure measurement during provocation lumbar diskography, despite familiarity with the technique. In our experience, pressure measurements have rendered limited insight into confirmation of or characterization of (concordant-versus-diskordant) objectively provoked diskogenic pain beyond a perceived end point to injection. This result is in part supported by the lack of clear postoperative improvement when pressure-controlled diskography is used in patient selection.54–56 Of interest, a statistically significant difference in surgical outcome between diskectomy/intradiskal fusion in low-pressure (leaking?) disks compared with fusion only in high-pressure (contained nonleaking?) disks has been demonstrated in a subset comparison within 1 study.56
Several limitations are present in this retrospective study, despite the large number of patients and disks evaluated. In contained disks, internal disk derangement is complex, flow of injected material is unpredictable, and uniform spread of the injected anesthetic may not occur, leading to a reduced rate of improvement in these disks. In leaking disks, early epidural contrast reabsorption may lead to under-recognition in subtle cases with small leaks, not originally appreciated at fluoroscopy. Second, many leaking disks cannot be completely distended, and areas of annular injury may not be fully tested with anesthetic or adequately provoked without more aggressive biomechanical strain. Third, anesthetic leakage, if excessive, could potentially mask the response at another level, but in our experience, adjacent levels can be correctly tested after anesthetic administration.
Conclusion
The provoked pain response of lumbar disks to intradiskal lidocaine administration was different for disks demonstrating diskographic leakage versus disks without contrast leakage. This observation suggests that the primary pain generator related to the disk is in the outer annulus or extrinsic to the disk. In painful disks without diskographic leakage, though some patients improved after anesthetic injection, most did not, and it is possible that injected lidocaine simply cannot reach the appropriate nerves. These observations suggest more than 1 cause of diskogenic LBP, and these causes may overlap in the patient or at an individual disk level.
Acknowledgments
We thank Marcia Kurs-Lasky for her support with statistical analysis and Eric Jablonowski for his assistance with image preparation.
References
- Received October 31, 2006.
- Accepted after revision December 11, 2006.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}