
Abstract
Summary: We present the case of a 30-year-old man with silent sinus syndrome. A CT scan obtained 10 years earlier showed completely normal maxillary sinuses. This case illustrates the acquired nature of this disorder.
The silent sinus syndrome, also known as imploding antrum and chronic maxillary sinus atelectasis, consists of findings of painless enophthalmos and inward retraction of the ipsilateral maxillary sinus walls on imaging studies (1, 2). The resultant volume loss in the maxillary sinus accounts for orbital enlargement and enophthalmos. The distinction between the imaging appearance of hypoplastic maxillary sinus and silent sinus syndrome is not well understood. Some authors believe that a congenital underdevelopment of the maxillary sinus is responsible for the development of silent sinus syndrome, but the acquired nature of this condition is now more readily apparent (3). Obstruction of the maxillary ostium appears to play a critical role in the development of silent sinus syndrome. Events leading to retraction of the walls of the obstructed sinus are not clearly understood.
Case Report
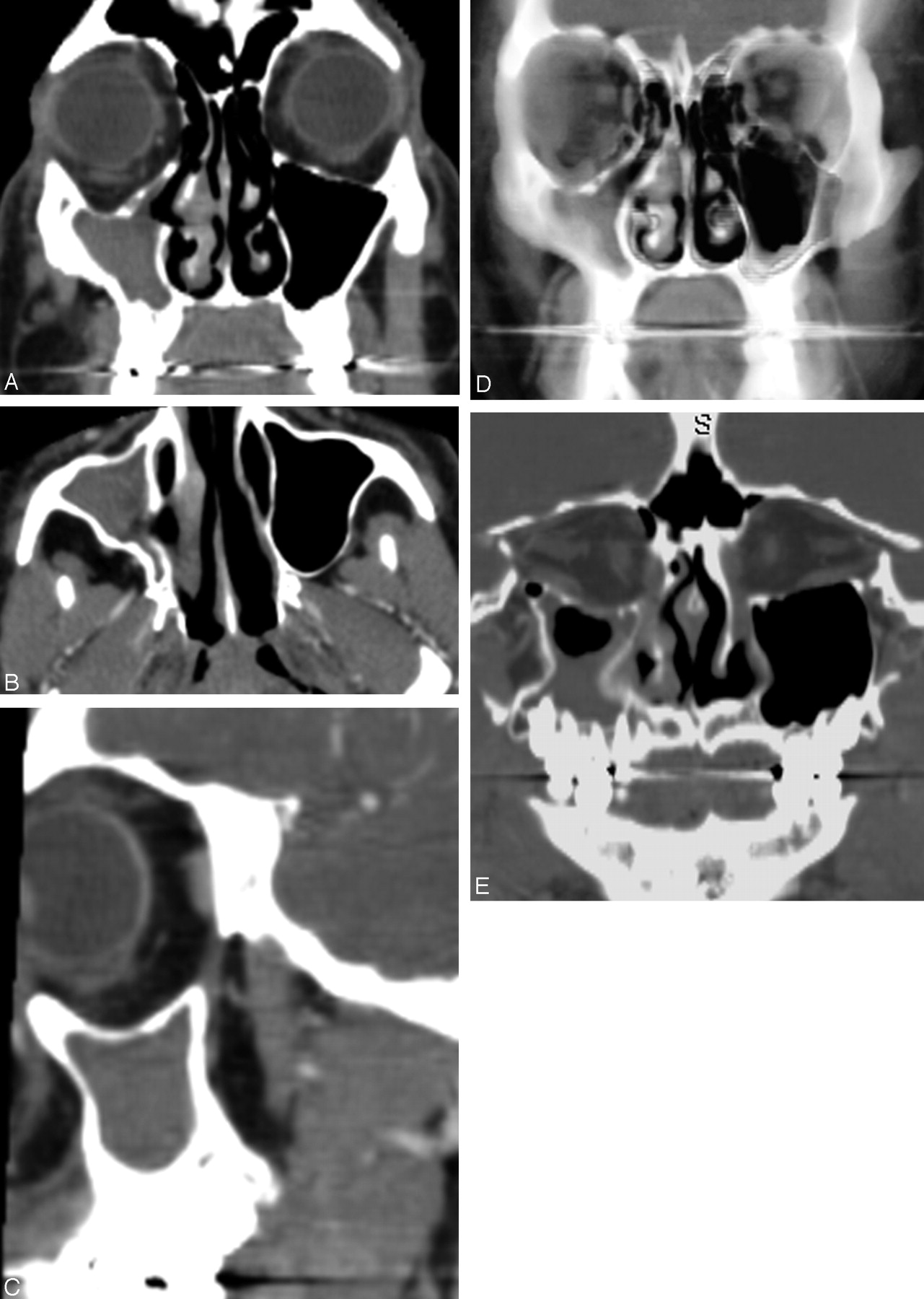
A 30-year-old man was found to have asymmetrically enlarged palatine tonsils, right greater than left, during an upper respiratory infection. The tonsillar asymmetry did not resolve with proper antibiotic treatment. A CT scan of the neck performed for evaluation of a potential underlying mass revealed a completely opacified maxillary sinus on the right. There was significant volume loss of the right maxillary sinus with inward retraction of the slightly thickened walls and consequent enlargement of the right orbit and middle meatus (Fig 1). The uncinate process was thinned and retracted to the orbital wall, obstructing the maxillary sinus infundibulum. Of note, there was no underlying mass to account for tonsillar asymmetry. The patient did not have any symptoms that might be related to sinusitis. He did not notice any enophthalmos but retrospectively recalled a girlfriend several years before noting his right “eye line” being lower than that on the contralateral side. Right enophthalmos and 1–2 mm of hypoglobus were observed on repeat examination (Fig 2).

(A) Coronal, (B) transverse, and (C) sagittal CT images of the sinuses show inward retraction of all walls of the right maxillary sinus with enlargement of the orbit and the middle meatus. The uncinate process is not clearly visualized because it is markedly thinned and retracted to the inferomedial orbital wall (confirmed with nasal endoscopy). (D) Thick-slab volume reconstruction in the coronal plane and (E) curved reconstruction along the optic nerves better demonstrates the maxillary sinus volume loss and enlargement of the orbit and middle meatus.

Frontal view of the patient, demonstrating hypoglobus and enophthalmos of the right eye.
The patient had undergone a CT scan of the paranasal sinuses 10 years previously for presurgical evaluation of a posttraumatic nasal septum deformity that occurred during childhood. Findings showed that the right maxillary sinus size and wall thickness were normal (Fig 3). Soon after that initial CT, he underwent nasal septal reconstruction and revision rhinoplasty, including lateral nasal osteotomies.

Coronal sinus CT of the patient obtained 10 years previously, before nasal septal reconstruction and rhinoplasty with lateral osteotomies, shows normal sinuses.
The patient elected not to pursue surgical treatment of the maxillary sinus disease. His tonsillar asymmetry remained stable during a 14-month follow-up.
Discussion
The silent sinus syndrome is a spontaneous unilateral maxillary atelectasis with complete or partial opacification of the sinus. Silent sinus syndrome is a rare disorder, but it is probably underdiagnosed because of a lack of recognition (1). The typical patient with silent sinus syndrome is an adult in the third through fifth decades of life who presents with spontaneous, painless, and occasionally progressive enophthalmos and hypoglobus (1, 2). No symptoms attributable to chronic sinonasal disease are present. Physical examination findings may include upper lid retraction, deepened upper lid sulcus, malar depression, facial asymmetry, and diplopia. The diagnosis of silent sinus syndrome can be made clinically, but it should be differentiated from other causes of spontaneous enophthalmos such as Parry-Romberg syndrome and linear scleroderma.
The imaging findings are characteristic (4). The primary finding is maxillary sinus volume loss due to inward retraction of the sinus walls, which accounts for the increased orbital volume and enlargement of the middle meatus. Typically, all 4 walls of the sinus are retracted, though one of the medial, anterior, or posterolateral walls may be spared. The orbital floor (maxillary roof) is always retracted and commonly thinned. The other walls may be thinned, normal, or slightly thickened. The maxillary infundibulum is always occluded and the sinus is opacified. The uncinate process is retracted against the inferomedial aspect of the orbital wall.
Our patient exhibited all the characteristic findings of silent sinus syndrome and slight thickening of the walls of the sinus including the orbital floor. The orbital floor thickening is uncommon and was reported to be present in 3 of 12 patients of Rose et al (2) and none of 68 patients of Soparkar et al (1). We speculate that the slight thickening of all walls of the sinus and ipsilateral tonsillar hypertrophy are secondary to chronic inflammation. Soparkar et al argued that the wall thickening may indicate a coexistent developmental hypoplasia, which was clearly not the case in our patient because imaging before disease onset showed completely normal sinus walls (1).
The pathophysiology of silent sinus syndrome remains unclear. Initially, it was suggested that a developmentally small sinus with chronic obstructive sinusitis was the cause (3). The acquired nature of this condition, however, is now well recognized. Negative intrasinus pressure has been demonstrated in patients with silent sinus syndrome (5). Obstruction of the sinus ostium is always present, but it is not clear whether this is the cause or the result of sinus wall retraction. Complete obstruction of the mucous membrane–lined sinus resulting in gas resorption and negative pressure formation, in a similar manner to middle ear atelectasis due to Eustachian tube dysfunction, is the most plausible explanation. Given the rarity of silent sinus syndrome and the very high prevalence of maxillary sinus obstruction, however, one has to question this explanation. This theory also fails to offer an explanation for the exclusive involvement of the maxillary sinus. Perhaps, other compounding factors such as trauma or anatomic predisposition play a role (6).
In our patient, childhood nasal trauma and subsequent surgical trauma were likely factors in the later insidious development of silent sinus syndrome. An osteotomy performed during septal reconstruction and rhinotomy typically passes through the nasal process of the maxilla; however, an osteotomy extending more posteriorly could enter and destabilize the maxillary sinus. Despite the absence of chronic sinusitis symptoms in our patient’s case, subsequent scar contracture or maxillary sinus hypoventilation might then have resulted in the sinus atelectasis, hypoglobus, and enophthalmos typical of silent sinus syndrome.
The initial management in this syndrome should be conservative. If this is inadequate, then normal sinus drainage is restored by enlarging the maxillary ostium with functional endoscopic sinus surgery. Surgical intervention to improve sinus aeration typically halts the progress of maxillary sinus contraction but does not restore sinus volume. In patients with diplopia or severe cosmetic deformity, repair of the orbital floor with placement of a subperiosteal implant can be performed at the same time or after functional endoscopic sinus surgery.
In summary, this case supports the notion that silent sinus syndrome is an acquired condition. Thickening of the sinus walls is probably related to chronic inflammation and not to underlying developmental hypoplasia. Surgical or other trauma to the maxilla and sinus ostium may play a role in the pathogenesis of this condition.
- Received November 29, 2004.
- Accepted after revision December 13, 2004.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}