
Abstract
INTRODUCTION: There are no well-established physiologic or neuropsychological criteria for identifying which patients with stenosis of the cervicocerebral vessels are at high risk of stroke or cognitive impairment. Our purpose was to evaluate changes in cognitive performance and cerebral perfusion associated with endovascular stent placement of the cervicocerebral vessels.
METHODS: A consecutive series of 20 patients, 31–88 years of age, who underwent 21 stent procedures for arterial stenosis (10 extracranial carotid stents [ECS], four intracranial carotid stents [ICS], and seven extra- or intracranial vertebrobasilar stents [VBS]) was investigated retrospectively. All patients were evaluated with CT or MR perfusion studies both before and after stent placement. Cognitive response after stent placement was evaluated by using an informant questionnaire.
RESULTS: In patients with anterior circulation stenoses (ECS and ICS group), 11 of 14 (79%) had a baseline perfusion abnormality and all 11 patients showed improved perfusion after stent placement. Four of seven (57%) patients with posterior circulation stenoses (VBS group) had a baseline perfusion abnormality and two of the four patients showed improved perfusion after stent placement. Degree of stenosis was the strongest predictor of the presence of a baseline perfusion abnormality (P = .03). Fifteen of 19 (79%) of the patients showed improved cognitive scores after stent placement. Among patients with improvement in perfusion after stent placement, 11 of 13 (85%) had improved cognitive scores. Improved perfusion after stent placement was a significant predictor of cognitive improvement (P = .04). Patients who were stented on an elective basis demonstrated greater improvement in cognition as compared with patients stented urgently (P = .01).
CONCLUSION: Endovascular stent placement of the cervicocerebral vessels can safely and effectively resolve cerebral perfusion abnormalities. Improvement in perfusion parameters is associated with cognitive improvement. Larger, blinded, prospective studies are needed to confirm these preliminary observations.
Atherosclerosis of the cervicocerebral vessels is responsible for a large proportion of strokes. Although extracranial carotid occlusive disease is responsible for 25% of the 750,000 yearly strokes in the United States, as much as 10% of the stroke population harbor significant intracranial carotid artery stenosis (1, 2). Studies of patients with extracranial internal carotid artery stenosis undergoing carotid endarterectomy (CEA) have shown impaired preoperative neuropsychological performance (3–6). These studies have also shown that restoration of blood flow after endarterectomy correlated with cognitive improvement. Although there has been increasing adoption of endovascular stent placement of the cervicocerebral vessels as a less-invasive alternative to open surgery, the benefit of these new techniques in relation to cerebral perfusion and cognition has not been documented.
In the past several years stent placement of the cervicocerebral vessels has emerged as a less-invasive therapeutic alternative to CEA and extracranial/intracranial (ECIC) artery bypass in patients with significant intracranial stenosis. The safety of extracranial internal carotid artery stent placement has been demonstrated and carotid stents have recently received US Food and Drug Administration approval for use in high-risk patients (7–11). Several randomized clinical trials are in progress to compare the efficacy of extracranial carotid stent placement to CEA (12–17). The preliminary results of these studies have demonstrated comparable or lower 30-day and 1-year event rate of stroke, heart attack, or death in patients who have undergone extracranial internal carotid stent placement as compared with CEA.
Advancements in technology, such as more flexible coronary stents, have made treatment of intracranial stenosis more feasible. Several small, uncontrolled case series have demonstrated the safety and efficacy of intracranial stent placement (18–23). The SSYLVIA trial, the first prospective clinical study to evaluate stents for intracranial stenosis, has shown promising preliminary data (24). Compared with the natural history, the 30-day and 1-year stroke rates appear encouraging.
The first goal of this retrospective study was to evaluate whether stent placement improves cerebral perfusion abnormalities in patients with a related significant stenosis. The second aim was to determine whether patients experienced improved cognition following endovascular stent placement. Finally, we hoped to determine whether there was a correlation between improved cerebral perfusion and enhanced cognitive function.
Materials and Methods
Subjects
All procedures were performed according to institutional review board–approved guidelines. Between August 2003 and May 2004, 20 patients (21 procedures), 31–88 years of age, with a diameter stenosis of ≥65% of a major cervicocerebral vessel, underwent stent placement. All patients were referred for stent consideration because of ongoing neurologic symptoms in the related vascular region, despite maximal medical therapy. The patient population included nine patients with 10 extracranial carotid stenoses) (Table 1), four patients with intracranial carotid stenosis (Table 2), and seven with either extra- or intracranial vertebrobasilar stenoses (Table 3). Six patients (4, 7, 9, 10, 13, and 19) had radiographic evidence of small acute or subacute infarctions at presentation. All of the infarction sizes were <2 cm or involved <2 cm of cortex as determined by CT or MR imaging. Of the 21 stents placed, 17 were elective and four were urgent (within 4 hours of patient presentation) because of patient symptomatology. All stenoses were atherosclerotic except for one, because of progressive carotid dissection.
Cases of stents placed for extracranial carotid stenoses
Cases of stents placed for intracranial carotid stenoses
Cases of stents placed for vertebrobasilar stenoses
Perfusion Imaging Acquisition and Analysis
Routine preprocedure stroke workup in all cases was performed with comprehensive head and cervical neurovascular MR or CT protocols, including MR angiography (MRA) and MR perfusion (MRP) and/or CT angiography (CTA) and CT perfusion (CTP). Poststent follow-up examinations were obtained at time points ranging from 4 hours to 3 months, by using the same imaging technique (CT, CTA, CTP or MR, MRA, MRP; Tables 1–3). Patient 15 did not have follow-up perfusion imaging after stent placement because of a progressive worsening of renal function; however, because the patient did not have baseline perfusion abnormality before stent placement, poststent perfusion imaging was not felt to be clinically necessary.
MR studies were performed on a standard 1.5T magnet (GE Medical Systems, Milwaukee, WI; 11.0 software platform). Standard clinical imaging sequences included sagittal T1, axial T2, axial diffusion-weighted images (B = 1000) with apparent diffusion coefficient maps, axial T2*, 3D time of flight (3D TOF) MRA at the circle of Willis, two-dimensional (2D) TOF cervical carotid arteries, dynamic contrast enhanced elliptic-centric MRA of the aortic arch through the circle of Willis, dynamic contrast bolus perfusion, followed by postcontrast axial T1 and coronal T2 fluid-attenuated inversion recovery brain images. Perfusion was acquired dynamically as a single-dose gadolinium T2* series covering 20–24 5–7-mm sections of brain. Parameter maps were calculated off-line on a commercially available system (GE Advantage Windows [AW] Workstation, version 4.2 by using Functool software, Milwaukee, WI), and maps were also automatically generated at the scanning console by using in-house software utilizing arterial deconvolution to calculate cerebral blood flow (CBF), cerebral blood volume (CBV), and mean transit time (MTT) maps according to previously published methods (25).
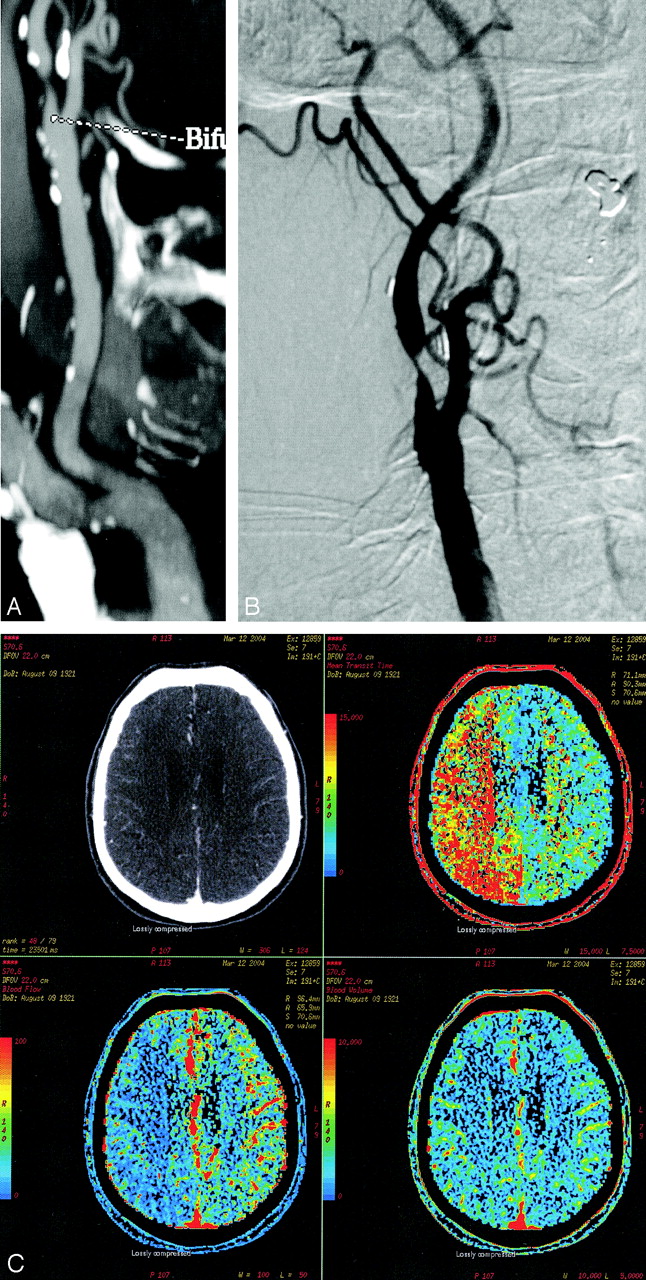
CT scans were also performed by using commercially available eight- or 16-section scanners (GE). Perfusion parameter maps were prepared on a GE AW Workstation using version 4.2 Perfusion 3 software. A routine head CT was performed with contiguous 5-mm axial images before and after the CTA/CTP. CTA of the head and neck was performed with a 120-mL timed bolus injection and a minimum section thickness of 1.25 mm spanning from the aortic arch to the top of the head. Thick-slab multiplanar CTA reformations and 3D reconstructions were built from this data set. CT perfusion images were then acquired by using a dynamic 40-mL intravenous contrast bolus, scanning a 2-cm region of the brain for 40–45 seconds (Fig 1). Perfusion coverage was adjusted according to vascular territory of interest, with carotid-directed examinations centered at the level of the top of the ventricles, and vertebrobasilar coverage centered to include the upper posterior fossa and lower occipital region.


Sample patient with cervical internal carotid artery stenosis.
A, CTA 2D reformation showing the innominate, right common, and internal carotid arteries with a significant stenosis in the proximal ICA.
B, DSA showing right ICA stenosis.
C, Prestent CT perfusion demonstrating abnormal prolongation of mean transit time (MTT; upper right), decreased cerebral blood flow (CBF; lower left), and normal cerebral blood volume (CBV; bottom right).
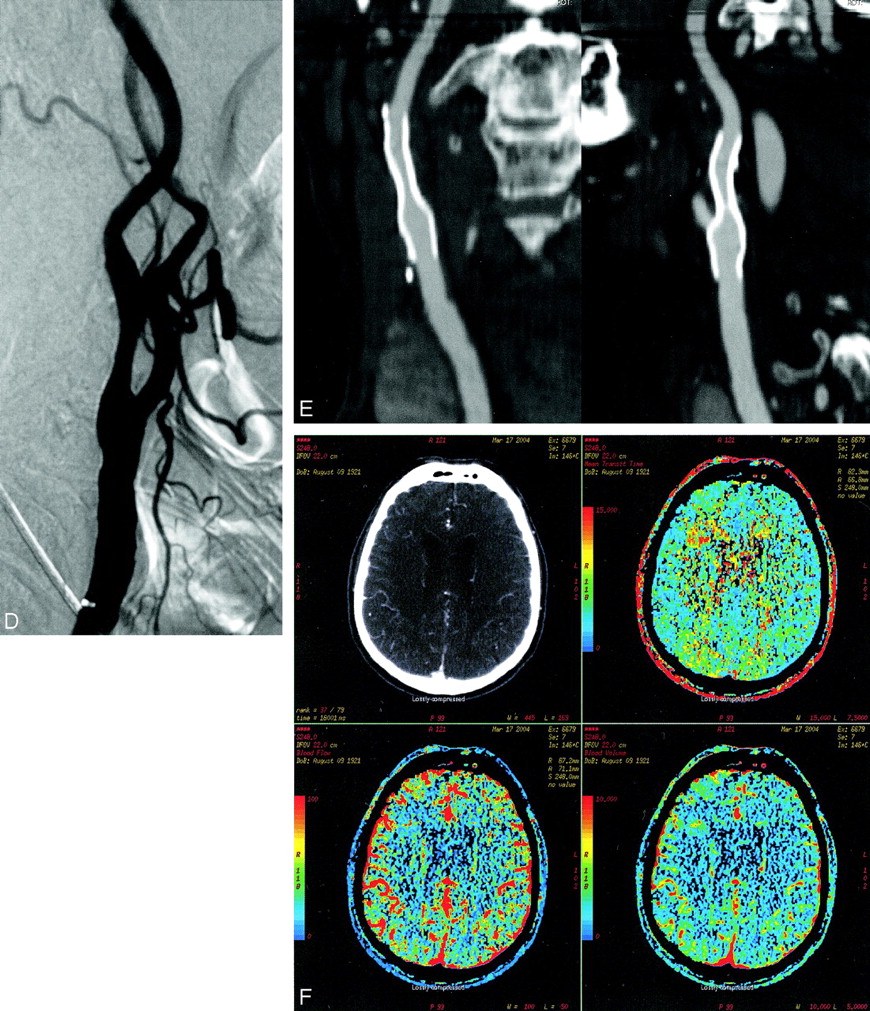
D, DSA after stent placement.
E, CTA 2D multiplanar reformation with orthogonal projections through the stent.
F, CT perfusion after stent placement demonstrates normalization of MTT (upper right), CBF (bottom left), and CBV (bottom right).
For the purposes of this study, routine clinically acquired CT or MR perfusion scans were analyzed by an independent senior neuroradiologist, blinded to the clinical condition, at a later time on a PACS workstation. The examiner addressed the following questions in this order: (1) Does a perfusion abnormality exist on the prestent study? (2) If a perfusion abnormality exists, does it correspond to the vascular distribution of the stenotic vessel? (3) In cases demonstrating prestent perfusion abnormality, does the poststent study show decline (assigned “−1”), no change (assigned “0”), improvement (assigned “1”) or normalization (assigned “2”) of perfusion? All three questions were answered by qualitative analysis of the MTT, CBV, and CBF maps displayed in standard color rainbow scale. A mean score for change in perfusion after stent placement was calculated for the anterior (ECS and ICS) and posterior circulation.
Angiographic Procedure and Analysis
The presence of carotid or vertebrobasilar stenosis was evaluated and characterized by utilizing the patients’ initial CTA or MRA, which allowed preoperative planning and risk stratification before conventional angiography. Quantitative angiographic measurements of the stenotic vessels were taken from the conventional angiograms before and after stent placement, according to methods described by the North American Symptomatic Carotid Endarterectomy Trial (NASCET) for cervical carotid lesions and WASID criteria for intracranial lesions (26, 27).
All patients were pretreated with clopidrogel (Plavix) and aspirin if they were not already taking these medications. All cervical carotid stenoses were treated with self-expanding stents (Precise, Cordis Corp., Miami, FL). All intracranial stenoses were treated with balloon expandable coronary stents (Driver, Medtronic Corp., Minneapolis MN; or BX Velocity, Cordis). Attempts were made to primarily stent all lesions with the stent size that most closely approximated the vessel without oversizing for balloon expandable stents and oversizing by 1–2 mm for self-expanding stents. Those stenoses where a stent would not primarily traverse the lesion were predilated with a 2.5- or 3-mm-diameter balloon (Maverick, Boston Scientific, Fremont CA), to allow passage of the stent. All intracranial stents were deployed with balloon inflation to nominal pressure. If necessary, angioplasty was performed after stent placement to achieve a 20% or less residual diameter stenosis.
The presence of circle of Willis collateral pathways was determined according to Hartkamp et al by analysis of the angiogram, CTA or MRA, and assigned separate scores for the anterior and posterior pathways (28). The anterior circle of Willis was considered intact if both proximal anterior cerebral artery segments were present together with an anterior communicating artery (Acom) or incomplete if any of these elements were missing (Tables 1–3). The configuration of posterior communicating arteries (Pcom) was also determined along with the side relative to the stenosis. In the ECS and ICS, the circle of Willis was labeled as “functional” if there was a competent Acom or a Pcom ipsilateral to the stenosis. For the VBS group, the circle of Willis was labeled as “functional” if at least one Pcom was present. The presence of a contributing contralateral vertebral artery was evaluated in patients with vertebral stenosis.
Clinical Data and Analysis
Demographic and clinical data of the patients in the study population were obtained by chart review. Changes in cognition were assessed by phone interview performed by a physician blinded to clinical data by using the Informant Questionnaire on the Cognitive Decline in the Elderly (IQ-CODE), which has been validated in prior studies (29–31). The IQCODE has been shown to correlate with the Mini-Mental State examination as well as a test of episodic memory performance (32, 33). This questionnaire consists of 16 questions assessing the patients’ memory, calculation skills, and decision-making capacity on a daily basis. One investigator performed all the cognitive evaluations. Patients were contacted by telephone, and verbal consent was obtained over the phone before conducting the interview. The questions were posed to a close contact (spouse or next of kin) who had an opportunity to observe the patient on a daily basis and was able to compare the patient’s performance before and after stent placement. In the event of a close contact not being available, the patient’s own response to the questionnaire was recorded. Each of 16 questions were graded +2 (much improved), +1 (slightly improved), 0 (no change), −1 (slight decline), or −2 (marked decline). Individual scores were tallied for each patient. The scale thus ranged from +32 for maximal improvement to −32 for maximal decline in cognition. All 20 patients had cognitive evaluation except patient 17, who was lost to follow-up (Tables 1–3).
Statistical Analysis
Associations between the presence of a preperfusion deficit and other baseline variables were assessed by using logistic regression. Predictors of the degree of postperfusion improvement and cognitive changes were assessed by using ordinary least squares. Differences in percent stenosis and cognitive change between groups were assessed by using the Wilcoxon rank-sum test.
Results
Patients
The mean age for the 20 patients was 67 years, with a range of 31–88 years. The mean age for the ECS group was 69 years and for the ICS and VBS group was 65 years. The patients included 19 men and one woman. Four of the 20 patients were actively symptomatic and treated urgently. Two of the patients treated urgently had extracranial carotid stenoses and two had vertebrobasilar stenoses (Tables 1 and 2). Of the four patients treated urgently, three had atherosclerotic-related stenosis and one a progressive dissection. Six patients had radiographic evidence of small acute or subacute infarctions at presentation.
Imaging
Examination of the initial perfusion studies demonstrated that prestent perfusion abnormalities were present in 15 of 20 (75%) patients. Analysis of the prestent perfusion studies by specific vascular category showed that seven of nine (78%) patients in the ECS group, four of four patients in the ICS group, and four of seven (57%) patients in the VBS group had prestent perfusion abnormalities (Tables 1–3). The prestent perfusion abnormality in all cases (15/15) corresponded to the territory of the stenotic vessel that was stented.
The mean poststent perfusion imaging follow-up was 18 days, range 0 (4 hours after stent procedure) to 90 days. Perfusion abnormalities improved or normalized in 13 of 15 (87%) patients and did not change in the other two patients. No patient had worsening in perfusion after stent placement. The poststent perfusion analysis was broken down by vascular categories. In the anterior circulation (ECS and ICS groups), all 11 patients with baseline perfusion abnormality had improvement or normalization of perfusion (Tables 1 and 2). In the posterior circulation (VBS) group, of the four patients with baseline perfusion abnormality two improved or normalized after stent placement (Table 3). Patients with anterior circulation stenosis demonstrated a greater degree of perfusion improvement after stent placement compared with patients with the posterior circulation stenosis (P = .02).
Nine of the 20 patients have had additional late perfusion imaging follow-up. The mean imaging follow-up has been 5 months (range, 1.5–8.5 months). None of these patients has developed a new perfusion abnormality in the vascular territory that was stented. In fact, two patients have had further improvement in their prior existing perfusion abnormality.
The results of the circle of Willis collateral pathways are summarized for each vascular category in Tables 1–3. Note that of the five patients who did not have prestent perfusion abnormality, four had a functional circle of Willis and one (patient 5) had bilateral extracranial carotid stenoses when the prestent perfusion imaging was acquired.
The degree of vessel stenosis was >65% in all subjects and was >90% in four patients in the ECS group (mean stenosis, 79%). Patients with prestent perfusion abnormalities had more severe stenoses on average (81.7%) than patients without a baseline perfusion abnormality (73%; P = .03).
Stent-related complications were infrequent and are in keeping with other reported series. One patient had a basilar restenosis at 1 month and one patient had a vertebral origin restenosis at 3 months. Both of these lesions were treated successfully by balloon angioplasty with resolution of symptoms. Patient 11 experienced a seizure due to reperfusion 1 week after right carotid siphon stent placement. None of the patients experienced a procedure-related stroke.
Clinical and Cognitive Outcomes
Follow-up with IQ-CODE questionnaire was performed between 3 and 14 months, with a mean of 6 months. Of the 20 patients, 19 had cognitive clinical follow-up and one (patient 17) was lost to follow-up. Five patients, all of whom lived independently, self-reported the IQ-CODE questionnaire due to unavailability of a close contact.
Fifteen of the 19 patients (79%) had positive cognitive scores (mean, +9.9; range, −8 to 32) after stent placement. Of the remaining four patients, one had no cognitive change (score, 0), and three had negative cognitive scores. The patient with a −8 cognitive score was treated emergently after failed surgery and had hemorrhagic conversion of an acute infarction. Among the anterior circulation patients 12 of 13 (92%) had positive cognitive improvements as compared with three of six patients (one lost to follow-up) in the posterior circulation. The mean improvement in cognitive scores was significantly higher (+12.8) in the anterior circulation as compared with the posterior circulation (+3.8; P = .05).
The relationship of perfusion improvement to cognitive scores was then examined. Improvement of perfusion after stent placement was a significant predictor of cognitive improvement (P = .04). Of the 13 patients whose perfusion improved or normalized after stent placement, 11 (85%) had a positive cognitive score, one had a negative score, and one was lost to follow-up (mean cognitive score, +13.5; range −8 to 32). Cognitive scores were then further analyzed in terms of not only perfusion, but also the vascular territory involved. Among patients who had improved or normalized perfusion after stent placement, 10 of 11 (91%) patients in the anterior circulation had positive cognitive scores (mean cognitive score, +14; range, −8 to 32; Tables 1 and 2). In the posterior circulation, one of two patients had a positive cognitive score, and one was lost to follow-up (Table 3).
Among the patients stented on an elective basis, 15 of 16 (94%) had positive cognitive score after stent placement. Of the four patients stented urgently, one had positive cognitive score, two had negative cognitive score, and one was lost to follow-up. Patients stented on an elective basis had significantly greater cognitive improvement (mean cognitive score, +12; range, −1 to 32) as compared with patients stented urgently (mean cognitive score, −1; range, −8 to 8; P = .01).
Discussion
High-grade stenosis of the cervicocerebral vasculature is a known risk factor for stroke (34); however, not all patients harboring stenosis will develop overt symptoms preceding a major stroke. Considerable controversy exists over the treatment of asymptomatic stenoses of the cervicocerebral vasculature (27, 35). There are many clinical factors and anatomic features that are used to stratify patients’ risk for stroke. Currently, however, there are no objective physiologic, imaging, or neuropsychological criteria for identifying which patients with cervicocerebral stenosis are at high risk for stroke.
NASCET and ECST have shown the benefit of surgical revascularization in patients with cervical carotid stenosis (26, 36). Although renewed interest in surgical bypass has recently developed, to date no studies have shown a clear advantage of medical therapy over surgical bypass for patients with intracranial stenosis (27, 37). Cervical internal carotid artery stent placement has been shown to have a low complication rate, but long-term outcomes are not known (38–40). Although endovascular therapy is an evolving technology with limited long-term data, it does show promise in patients with high risk of stroke related to intracranial stenosis (24).
This study suggests that many patients with significant cervicocerebral stenosis demonstrate perfusion abnormalities at initial presentation that are improved after stent placement. We noted the degree of perfusion improvement was greater after anterior circulation stent placement than posterior circulation. In the anterior circulation, all patients had improvement of perfusion abnormalities after stent placement, whereas in the posterior circulation half of the patients had improvement of perfusion. One explanation for the lesser degree of perfusion improvement in the posterior circulation could be the qualitative limitations of CT and MR perfusion imaging used in this study for evaluating posterior circulation anatomy. Our studies were qualitatively evaluated because of difficulty obtaining reproducible quantitative information from the CTP data sets, which has been recently reported (41). Other potential limitations to imaging the posterior fossa include small size of anatomic structures, T2* effects from the skull base with MRP, and limited coverage area of CTP. These theories could also explain why baseline perfusion abnormalities were not seen in 57% of the posterior circulation patients as compared with 85% of anterior circulation patients.
Hypoperfusion resulting from impairment of cerebral blood flow has been documented in patients with significant cervicocerebral stenosis (42, 43). Subsequent revascularization with carotid endarterectomy or angioplasty has been shown to improve cerebral blood flow (44–46). Studies of cerebral blood flow after stent placement, however, are limited and have used ultrasonography of large vessels to demonstrate blood-flow improvement after stent placement (47). Positron-emission tomography (PET) O2 extraction is another means to evaluate cerebral blood flow, but the limited availability and access to PET scanners make this a difficult possibility and further emphasizes the promise of CT/MR methods. The results of this study are similar to previous reports showing improved cerebral perfusion after stent placement; however, our results are unique in that we used dynamic cerebral perfusion imaging and also included intracranial stent patients. Dynamic perfusion imaging is an increasingly available and useful technique in the initial evaluation of patients with stroke that can be integrated with traditional vascular and parenchymal imaging tests (48–50).
Another point that this study suggests is that patients with both anterior and posterior circulation stenoses show cognitive improvement after stent placement. Furthermore, the patients in the anterior circulation group with improved perfusion after stent placement showed a stronger association with cognitive improvement. Several studies have documented the cognitive deficit of patients with cerebrovascular stenosis (5, 6, 51, 52). Others have shown the cognitive improvement of patients after carotid endarterectomy (3, 4, 53, 54). Patients undergoing extracranial-intracranial bypass surgery have also benefited cognitively by this revascularization procedure (55). Our study validates the idea that many patients with cervicocerebral stenosis have cognitive dysfunction and that anterior and posterior circulation revascularization with stent placement improves cognition. Cognitive improvement after stent placement in the posterior circulation is less clear, likely because of small patient population in this study and the relatively limited role of the posterior circulation in the higher functions tested by our questionnaire.
In this study, patients who were stented on an elective basis had greater cognitive improvement than did patients who were stented urgently. This suggests that patients who are stented urgently could show cognitive improvement; however, the improvement might be to a lesser degree as compared with patients treated on an elective basis. One explanation for lesser degree of cognitive improvement in patients who are stented urgently could be that this group of patients presented with an already poor neurologic examination from an acute infarction that could make cognitive improvement difficult.
One possibility for the lack of baseline perfusion abnormality before stent placement could be related to degree of vessel stenosis. In our study, patients with perfusion abnormality had a higher vessel stenosis (81.7%) as compared with patients without perfusion abnormality (73%; P = .03). Another explanation for lack of perfusion abnormality before stent placement could be presence of functional circle of Willis. Among the patients without prestent perfusion abnormality, four of five had a functional circle of Willis. Collateralization from leptomeningeal vessels or retrograde ophthalmic artery flow, which has been studied, could also account for the absence of perfusion abnormality (56). In patient 5, lack of perfusion deficit before stent placement could be explained by the fact that there were bilateral carotid stenoses, which would make the perfusion symmetrical. Also, CTP has limited volume coverage, which could miss the affected area and evaluation of the posterior fossa with MRP has T2* limitations due to the skull base.
Risk of future stroke in presence of stenosis relates to embolic and hemodynamic causes. Perfusion at rest can only show potential hemodynamic derangement and does not indicate risk from emboli. Therefore, this would be expected to be an imprecise indicator of global stroke risk, even if a perfect measurement tool. This stresses the need for global imaging assessment including detailed vascular imaging.
This study has several limitations. Some of the cases were evaluated with CT perfusion (n = 14) and some with MR perfusion (n = 7); however, the initial and poststent perfusion imaging for 83% of the cases was the same technique. The perfusion scans were evaluated qualitatively based on color differences of a standard rainbow scale. The time to clinical and imaging follow-up was not the same for all patients. The IQ-CODE, even though clinically used for cognitive evaluation, has not been previously tested in a clinical study such as this. Also, the IQ-CODE questionnaire was administered directly to five patients because of unavailability of a close contact. Finally, this study is retrospective with a small population of patients and lacks a medically treated control group.
These observations illustrate the potential ill effects of vascular stenosis beyond the more obvious risks of hemodynamic or embolic stroke. Chronic hypoperfusion can lead to chronic cognitive dysfunction, either on a persistent or intermittent basis. The resting perfusion examinations done in our patients are limited in that they provide only a snapshot of resting flow in one position at one moment in time. Because CT and MR perfusion measurements are done with patients recumbent, this may represent optimal perfusion conditions. Intermittent periods of even more severe regional oligemia than shown in our perfusion examinations might be expected due to blood pressure fluctuations related to daily activities, assumption of upright postures, medication, hydration status, and other factors.
In conclusion, this study suggests that patients harboring cervicocerebral stenosis especially of the anterior circulation with a corresponding perfusion abnormality derive a cognitive benefit from cerebral revascularization when treated on an elective basis before a cerebrovascular event. This pilot study supports the theory that physiologic and neuropsychological criteria for identifying patients with cervicocerebral stenosis are needed so that early therapeutic intervention can be instituted before a devastating stroke occurs. Currently, there is an ongoing prospective study on this subject matter at our institution.
References
- Received November 14, 2004.
- Accepted after revision January 26, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Considering Psychological and Cognitive Factors in Interventional Neuroradiology: A Systematic Literature Review
- The association between vertebrobasilar insufficiency and the risk of dementia: a nationwide register-based retrospective cohort study in Taiwan
- Improvement of working memory after stenting for cervicocerebral artery stenosis
- Hemodynamic Alterations in Vertebrobasilar Large Artery Disease Assessed by Arterial Spin-Labeling MR Imaging
- The Role of Carotid Artery Stenting and Carotid Endarterectomy in Cognitive Performance: A Systematic Review
- New Brain Lesions After Carotid Stenting Versus Carotid Endarterectomy: A Systematic Review of the Literature