
Abstract
Summary: Test occlusion of a patent dural sinus requires careful hemodynamic evaluation. We performed balloon test occlusion of the sigmoid sinus in a patient with an advanced-stage temporal bone malignancy that affected the dominant sigmoid sinus. Before and during the test occlusion, intrasinus pressure was monitored upstream from the balloon via the inner lumen of a double-lumen angioplasty balloon microcatheter. On the basis of the hemodynamic findings, permanent balloon occlusion was carried out without complications.
Radical surgery for extended tumors at the skull base may require sacrifice of the internal carotid artery (ICA) or the affected dural sinuses (1). Balloon test occlusion (BTO) of the carotid artery allows accurate prediction of the outcome of permanent arterial occlusion concerning the development of postprocedural neurologic deficits (2). However, individual tolerance to surgical sacrifice of a patent dural sinus is difficult to assess, and concern regarding potential venous infarction is central to surgical planning (3, 4).
We present a case in which an advanced-stage temporal bone malignancy affected the dominant sigmoid sinus. To evaluate the tolerance to surgical sacrifice, we performed preoperative BTO of the sigmoid sinus, with the measurement of venous pressure upstream from the balloon before and during its inflation. On the basis of the hemodynamic and clinical findings during BTO, permanent occlusion of the affected segment of the sinus with a detachable balloon was carried out to minimize the risk of hemorrhagic complications during surgery. The aim of this study was to determine the value of hemodynamic evaluation during test occlusion of a dural sinus.
Description of the Technique
A 66-year-old female patient presented with a 6-month history of unilateral hemorrhagic otorrhea, otalgia, progressive hearing loss, and vertigo. Otoscopy showed a lesion that completely occluded the external auditory canal, with no visibility of the tympanic membrane. Audiometry demonstrated deafness of the affected ear. Facial nerve function was grade II on the House/Brackmann scale. Biopsy led to the diagnosis of a squamous cell carcinoma.
CT and MR imaging revealed a tumor of the right temporal bone, with extension to the external auditory canal and middle-ear compartments and also erosion of the bony labyrinth and mastoid and destruction of the cortical bone overlying the sigmoid sinus (Fig 1). The tumor was contiguous with the dura of the middle cerebral fossa and the dural wall of the right sigmoid sinus, causing elevation of the middle fossa dura and substantial reduction of the sinus lumen (Fig 2). The contralateral transverse and sigmoid sinuses were patent yet of smaller caliber than the dominant right-sided ones. On the basis of further preoperative evaluation, the tumor was staged a T4 (C2) N2b (C2) M0 (C2), stage 4 lesion according to the modified Pittsburgh tumor staging system (5). Combined surgical resection and irradiation was considered.

CT, bone window, shows destruction of the right mastoid and cortical bone overlying the sigmoid sinus.

Postgadolinium axial T1-weighted MR image reveals an enhancing tumor causing substantial compression of the lumen of the sigmoid sinus.
Planning for surgery involved evaluation of the potential need to sacrifice the sinus to achieve a definitive resection in case of macroscopic tumor invasion. To assess the safety of sigmoid sinus sacrifice, we performed BTO of the sinus with the intention to proceed with permanent balloon occlusion of the affected segment if the test occlusion was well tolerated and if the increase in pressure was less than10 mm Hg. We obtained informed consent from the patient, with the understanding that BTO of the sigmoid sinus was a novel and unproven diagnostic approach.
During endovascular BTO, the patient was conscious, with continuous ECG and blood pressure monitoring under surveillance of an anesthesiologist.
Cerebral angiography of both ICAs and the left vertebral artery via a left femoral approach showed stenosis in the right sigmoid sinus, with 80% narrowing of the lumen; this was consistent with the MR imaging findings (Fig 3). The vein of Labbé drained proximal to the stenosis into the transverse sinus. The superior petrosal sinus was not visualized. The contralateral sinuses were patent yet of decreased caliber.

Right ICA angiogram, frontal projection in the venous phase, demonstrates an 80% stenosis in the proximal part of the dominant right sigmoid sinus.
A 6F sheath was placed in the right femoral vein, and the patient was given systemic heparin to maintain activated clotting times 2–3 times the baseline value. A 6F guiding catheter (Envoy; Cordis, Miami, FL) connected to a continuous flush was directed with a guidewire to the right jugular vein. Control cerebral angiography with fluoroscopic overlay was used for further venous catheterization. A 6 × 20-mm, double-lumen angioplasty balloon microcatheter (Savvy; Cordis) was introduced inside the guidecatheter over a 0.014-in microguidewire (Transend; Boston Scientific/Target, Natick, MA). After the microguidewire was withdrawn, pressure measurements were performed via the inner lumen of the microcatheter, which was connected to a pressure monitor (Hewlett-Packard, Avondale, PA) with a pressure transducer (Smiths, Kirchseeon, Germany).
Zero pressure was calibrated on the basis of the level in the right atrium. The recorded venous pressure in the sigmoid sinus distal to the stenosis was 12 mm Hg. The microguidewire was then advanced through the stenotic segment, and the tip of the balloon catheter was placed in the sigmoid sinus proximal to the stenosis. Venous pressure in the proximal sigmoid sinus before balloon inflation was 16 mm Hg. The balloon was then gently inflated in 30 seconds by using a manometer filled with a 50:50 mixture of contrast medium and normal saline solution. Inflation pressure did not exceed 1 atm. Angiography demonstrated complete occlusion of the sigmoid sinus (Fig 4). Venous pressure in the proximal sigmoid sinus upstream to the balloon increased to 22 mm Hg. The pressure recordings remained stable during the occlusion period of 30 minutes.

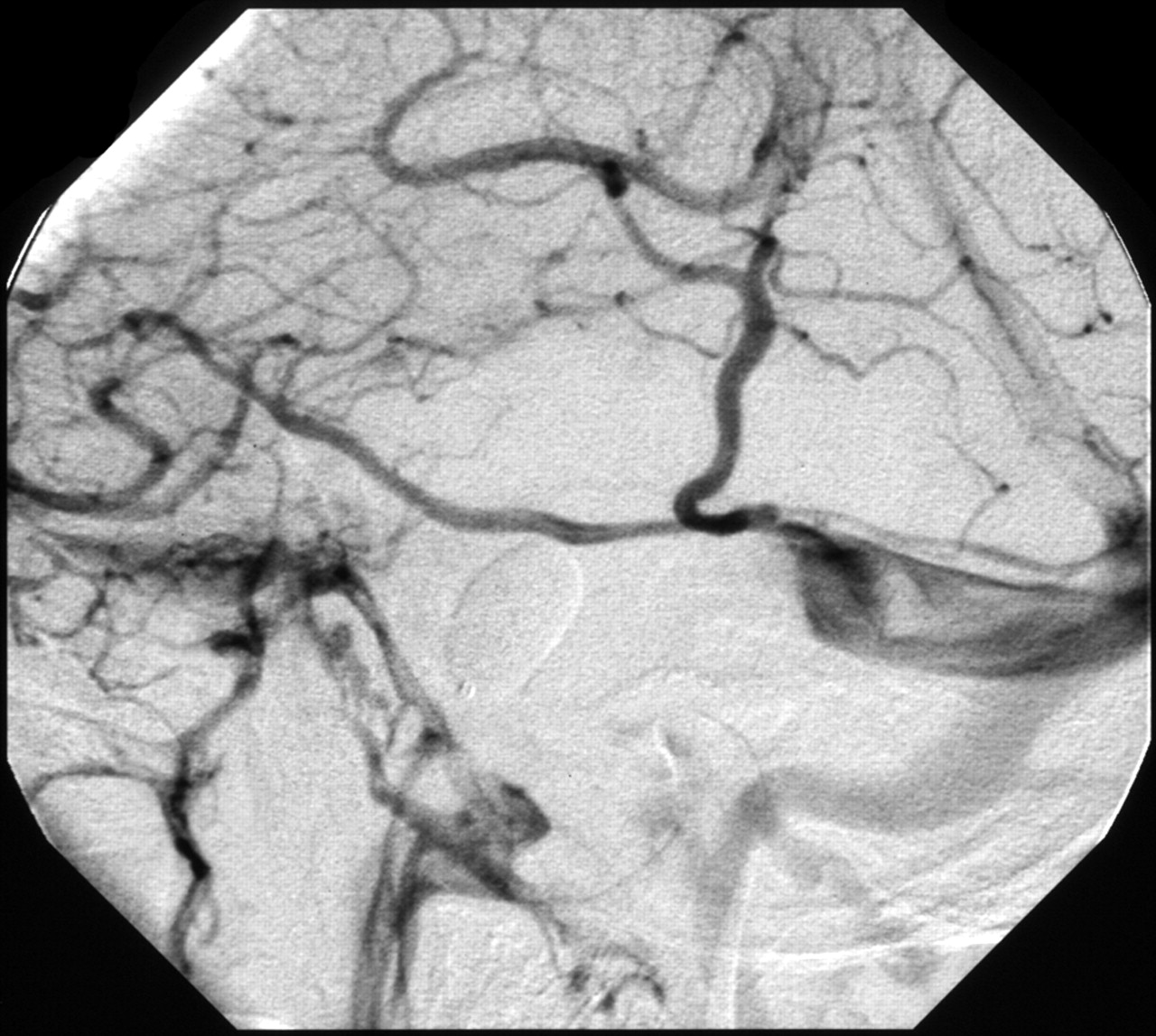
Control right ICA angiogram, lateral projection, obtained during test occlusion of the sigmoid sinus with a double-lumen angioplasty balloon inflated with a mixture of contrast agent and saline shows adequate drainage of the vein of Labbé without delay into the transverse sinus.
During the procedure, the patient felt comfortable and developed no neurologic deficits or headache. Control angiography showed drainage of the vein of Labbé to the contralateral sinus without any delay compared with the deep cerebral venous system. After deflation and removal of the balloon, control angiogram was performed; the results ruled out any procedure-related injuries.
On the basis of the hemodynamic and clinical findings during BTO, we proceeded with permanent balloon occlusion of the affected segment of the sinus with a detachable balloon (Goldbal, Balt, France). Angiography demonstrated occlusion of the sigmoid sinus at the level of tumoral compression and confirmed patency of the jugular bulb via drainage of the inferior petrosal sinus and basilar plexus.
After the endovascular procedure, systemic anticoagulation was continued for 48 hours. The patient was kept well hydrated and under surveillance in an intermediate care unit. She did not develop any postprocedural neurologic deficits. Control angiography after 48 hours confirmed occlusion of the affected sigmoid sinus and patency without thrombotic alterations of the adjacent sinuses and the vein of Labbé (Fig 5).

Control right ICA angiogram 2 days after permanent occlusion of the sigmoid sinus with a detachable balloon demonstrates patency of the transverse sinus with drainage of the vein of Labbé and jugular bulb via drainage of the inferior petrosal and basilar plexus.
Three days after sigmoid sinus occlusion, the patient underwent surgical resection consisting of subtotal petrosectomy with removal of the otic capsule, total parotidectomy, and ipsilateral posterolateral neck dissection. The tumor extended into the external auditory canal and middle ear compartments, the mastoid, and the bony labyrinth. There was elevation of the middle fossa dura and impression of the sigmoid sinus but no macroscopic tumor infiltration of these structures. The tumor could be separated in a plane of cleavage from the middle and posterior fossa dura and the medial wall of the sigmoid sinus. The dura was kept intact to protect the underlying nervous and venous structures of the cerebellopontine angle and to avoid intracranial hemorrhage and CSF leaks. Preoperative occlusion of the affected segment of the sinus allowed rigorous separation of the tumor from the medial sinus wall without the risk of hemorrhagic complications in case of sinus injury. The external auditory canal was closed as a blind sac, the cavity was obliterated with abdominal fat and covered by an inferior transposition of the temporalis muscle.
Postoperatively, the patient had no new neurologic deficits and was scheduled for subsequent radiation therapy. CT and MR imaging confirmed complete resection of the tumor and revealed no signs of venous infarction.
Discussion
In cases of advanced-stage temporal bone carcinoma, both extensive resections and high-dose irradiation are recommended (6). Although the prognosis of a patient with a T4/stage 4 lesion is grim, survival is better when clear surgical margins can be achieved (5). When an individual situation is assessed, the justified use of radical surgery must be weighted against potential morbidities that may result from facial nerve or ICA resection or the need to sacrifice the dominant sigmoid sinus, as in the present case.
If a dural sinus is completely occluded because of tumor invasion, adequate venous collaterals have developed and the affected sinus can be excised without ensuing venous complications (7). If the affected sinus is still patent, however, the risk of sinus occlusion is high, especially in the posterior two-thirds of the superior sagittal sinus and the dominant transverse or sigmoid sinus; this situation entails the risk of intracranial hypertension and venous infarction (3, 4, 7). Obstructed flow of the vein of Labbé classically results in a hemorrhagic infarction in the lateral aspect of the temporal lobe and constitutes a life-threatening complication with high morbidity and mortality rates (8).
In our case, preoperative MR imaging demonstrated substantial tumor-related narrowing of the lumen of the dominant right sigmoid sinus, but epidural compression and tumor invasion could not be differentiated. The indication for BTO was based on the potential need to sacrifice the sigmoid sinus to achieve definitive tumor resection. Permanent balloon occlusion of the affected segment of the sinus was planned to reduce the risk of hemorrhagic complications during surgery.
Sinus occlusion testing with both surgical and endovascular techniques has been reported. Spetzler et al (9) and Schmid-Elsaesser et al (3) described intraoperative monitoring of sinus pressure to assess the tolerance to sinus occlusion by measuring stump pressure via a surgically placed transducer during test clamping of the involved sinus segment. Endovascular techniques comprise blind BTO with a latex balloon attached to the tip of a microcatheter and BTO with pressure measurements via a double-lumen angioplasty balloon microcatheter (4, 10). Blind BTO has been performed before endovascular sacrifice of the transverse sinus for treatment of a dural arteriovenous fistula to assess tolerance to occlusion of cortical vein drainage within the dural sinus (10). The use of a no-end-hole balloon microcatheter does not allow pressure measurements, and distal navigation of this balloon is sometimes difficult.
Houdard et al (4) introduced BTO with a noncompliant double-lumen angioplasty balloon by using the inner lumen of the balloon microcatheter for pressure measurements during occlusion testing of the straight sinus. The reliability of blood pressure measurements via microcatheters was established in experimental and clinical applications by Duckwiler et al (11).
Endovascular BTO requires systemic anticoagulation to prevent thrombotic complications and careful manipulation to avoid venous rupture or dislodgement of fragments of the tumor in cases of intraluminal tumor growth (7). The advantages of endovascular techniques compared with surgical testing rely on the angiographic assessment of collateral venous drainage during test occlusion and on the possibility to perform neurologic examinations during the procedure. The use of a double-lumen balloon microcatheter additionally allows us to record venous pressure at different sites and thus determine a preexisting pressure gradient due to tumor compression and the gradient changes during balloon inflation.
Clinical examination alone without hemodynamic assessment during BTO of a venous sinus does not allow accurate prediction of the tolerance to permanent sinus occlusion. Both the anticipated neurologic deficits and their rate of onset are ill defined. Sekhar et al (1) reported a patient who underwent BTO without intrasinus pressure measurement and subsequent permanent occlusion of the sigmoid sinus in preparation for radical temporal bone resection. Eight minutes after permanent occlusion, the patient became comatose as a result of severe brain swelling and hemorrhages. The patient made a fair recovery after ventriculostomy and cerebellectomy.
Several factors influence intracranial venous pressure, in particular the patient’s position, the degree of neck inclination, and the level and type of anesthesia (3). With regard to hemodynamic evaluation during sinus occlusion testing, the determination of a preexisting pressure gradient across a stenosis and the recording of pressure changes during test occlusion are more relevant than the absolute values.
The interpretation of intrasinus pressure measurements depends on the anatomic localization. Schmid-Elsaesser et al (3) considered any increase in superior sagittal sinus stump pressure during surgical test occlusion as insufficiency of collateral venous drainage. The hemodynamic situation in the transverse or sigmoid sinus, however, is different. It can be assumed that, during sigmoid sinus occlusion, an increase in pressure proximal to the obstruction is necessary to redirect flow to the contralateral sinus. Surgical experience provides data concerning the rise in pressure that can be tolerated. Spetzler et al (9) performed intraoperative measurements of sinus pressure during temporary occlusion in preparation for surgical sacrifice of the transverse or sigmoid sinus and proceeded to permanent sinus occlusion as long as the rise in pressure was below 10 mm Hg. There were no complications related to venous occlusion following this technique. Sekhar et al (12) performed saphenous graft bypass from the sigmoid or transverse sinus to the jugular vein when the increase in sinus pressure was more than 5 mm Hg.
We found a pressure gradient of 4 mm Hg across the tumor-induced stenosis in the sigmoid sinus and an increase of pressure upstream from the balloon during test occlusion of 6 mm Hg; this remained stable throughout the occlusion period of 30 minutes. Endovascular BTO allowed us to perform control angiography as a further means of hemodynamic evaluation. In our case, the angiograms did not show any signs of venous stasis or delay of drainage of the vein of Labbé.
Conclusion
Endovascular BTO with hemodynamic evaluation is a promising technique for assessing tolerance to sinus sacrifice. Further observations are required to confirm the reliability of this technique.
References
- Received June 15, 2004.
- Accepted after revision July 12, 2004.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.