
Abstract
Summary: Percutaneous balloon angioplasty has been found to be useful for the treatment of intracranial atherosclerotic arterial stenosis. Nonetheless, an ongoing risk of this procedure is arterial dissection, which increases the hazards of acute closure, stroke, and restenosis. Stenting of the intracranial vasculature recently has been shown to be feasible in a variety of circumstances. To our knowledge, however, stenting of the middle cerebral artery has not been possible until now primarily because of difficulty with tracking stents across the carotid siphon. We describe the successful treatment of a symptomatic middle cerebral artery stenosis achieved using a balloon-expandable flexible coronary stent.
The use of percutaneous balloon angioplasty for the treatment of intracranial atherosclerotic arterial stenosis is gaining increasing popularity. Earlier reports describing substantial complication rates related to vessel dissection, acute closure, perforation, and rupture are being updated by series with much better procedural outcomes (1–3). In the coronary, peripheral, and extracranial cerebral circulation, stenting has been shown to increase the safety and efficacy of balloon angioplasty for the treatment of arterial lesions (4–7). The introduction of new generation devices has led to a more feasible use of stents for treating lesions in the intracranial vasculature (8–10). Nonetheless, despite these advances, deployment of stents in the intracranial arteries remains a technical challenge.
Case Report
Clinical History
A 59-year-old man suffered multiple episodes of transient right-arm paralysis and speech arrest for 4 months despite treatment with aspirin and optimal doses of Warfarin (Coumadin; Dupont Pharma, Inc., Wilmington, DE). He had experienced a small infarction in the left cerebral hemisphere approximately 18 months earlier and had been found to have a 60% to 70% stenosis of the left middle cerebral artery. He was treated with oral anticoagulants until he developed recurrent symptoms of left-hemisphere ischemia. He had a normal neurologic examination between episodes. Because of the continued recurrence of symptoms despite optimal anticoagulation (international normalized ratio, 2.8) combined with antiplatelet treatment (aspirin 325 mg/day; clopidogrel 75 mg/day), the option of percutaneous angioplasty with stenting was discussed with the patient as part of a protocol approved by the local institutional review board. The procedure was performed successfully, and the patient was discharged the next day after an uneventful hospital course. One month later during a follow-up examination, he noted having had no recurrence of neurologic symtpoms and, in fact, described subjective improvement of his language function.
Technique
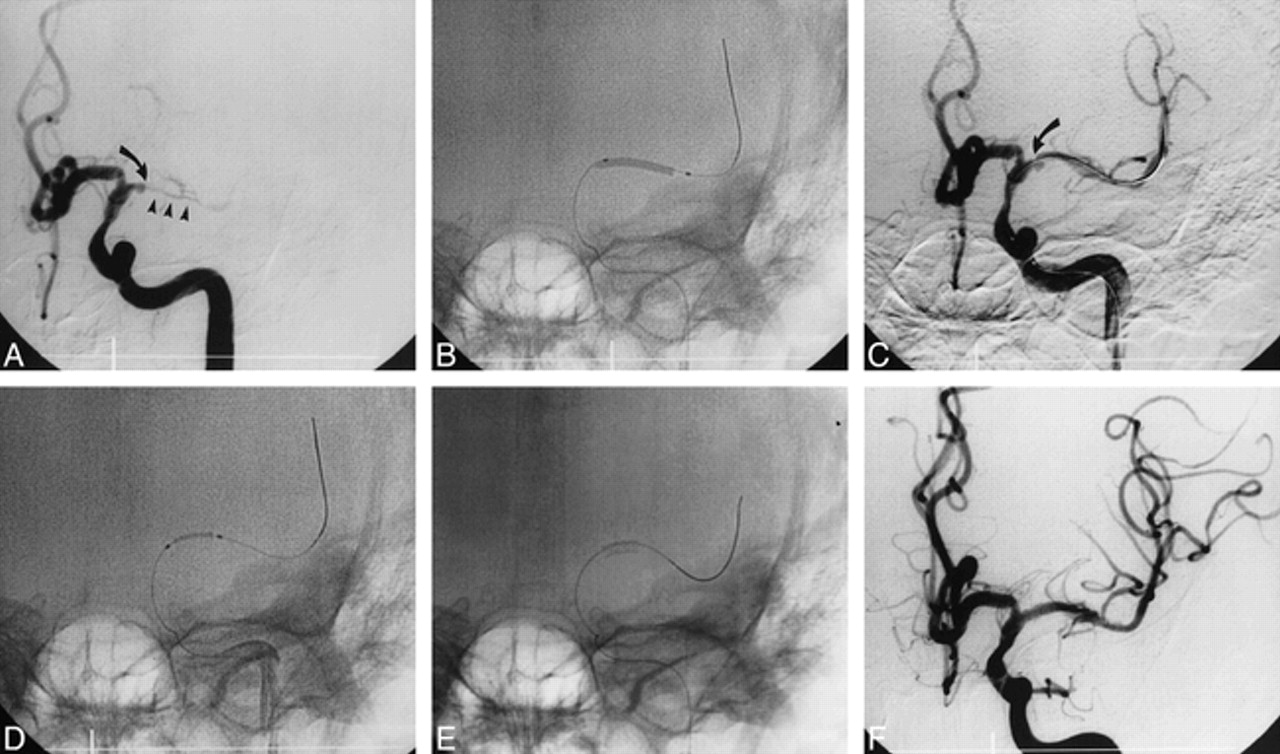
The patient was fully awake during the procedure; he did not receive any sedatives and the operation was performed under local anesthesia only. Percutaneous access was obtained via the fight femoral artery. The left common carotid artery was engaged with a 5F Newton 5 catheter (HN5), which was directed into the artery over a 0.038-inch hydrophilic-coated wire (Glidewire; Meditech, Inc. Watertown, MA). After obtaining a preliminary angiogram, the HN5 catheter was exchanged for a 6F multipurpose guiding catheter (Viking; Guidant Corporation, Inc., Santa Clara, CA), which was positioned in the distal cervical segment of the left internal carotid artery, just proximal to its petrous portion. Preprocedural angiographic images were then obtained in orthogonal planes (Fig 1A). The lesion was crossed with a microcatheter (TurboTracker 18; Target Therapeutics, Inc., Freemont, CA) over a 0.014-inch, floppy-tipped, hydrophilic-coated wire (Transcend; Meditech, Inc., Natick, MA). Injection of contrast material through the microcatheter confirmed its intraluminal position. A second 0.014-inch exchange-length floppy-tipped microwire (Luge; SciMed, Inc., Boston, MA) was introduced through the microcatheter, and its tip was positioned in the insular portion of the middle cerebral artery to ensure maximal support, allowing tracking of the balloon and stent. The stenosis then was predilated with a 2 × 20-mm coronary balloon catheter (Ninja; Cordis, Inc., Miami Lakes, FL) at 4 atm for 20 seconds (Fig 1B). Improvement of the vessel lumen was obvious, because it was the irregularity of the plaque that caused the stenosis (Fig 1C). Then, a 2.5 × 8.0-mm coronary stent (Multilink Duet; Guidant Corporation, Inc.) was advanced over the exchange wire (Fig 1D) and deployed in the middle cerebral artery origin by inflating the balloon to 9 atm (Fig 1E), with optimal angiographic results (Fig 1F). No neurologic events occurred during the procedure or during the postoperative period prior to discharge. The patient had been premedicated with aspirin and clopidogrel. These medications have been continued throughout the follow-up period, which by February 2000 amounted to 11 months. Treatment with Warfarin was discontinued after the procedure. Angiographic follow-up at 10 months showed no restenosis.

A, Anteroposterior (AP) view of stenotic middle cerebral artery (curved arrow). Note significant attenuation of distal portion of vessel (arrowheads). Most proximal portion of vessel shows ulcerated plaque, almost giving the appearance of an aneurysmal dilatation.
B and C, AP view of vessel during (B) and after (C) balloon angioplasty. Note improved patency but significant irregularity with recoil of lumen (curved arrow, B) after the procedure. The ulcerative character of plaque is better displayed in this view.
D–F, AP view of coronary stent prior (D), during (E), and after (F) deployment in the middle cerebral artery. Note smooth appearance of the lumen, with obliteration of the plaque ulcer at the end of deployment.
Discussion
Arterial stenting is a well-established technique for the treatment of atherosclerotic lesions of the coronary, iliac, and renal vasculatures. Its use in the cerebral arteries, however, has been largely confined to the extracranial portions of the vessels (4–7). In the past, the use of stents to support angioplasty of the intracranial arteries has been limited by the inability of the existing stents to track well into the intracranial portion of the vasculature. More recently, however, several authors have demonstrated the feasibility of stent deployment in the intracranial arteries (8–11). Despite these reports, the middle cerebral artery has remained a technical challenge primarily because of the difficulty with tracking the existing stents across the internal carotid siphon. Our case illustrates the feasibility of elective stenting of the middle cerebral artery, but our success needs to be examined critically with regard to the anatomic and technical circumstances that led to a successful procedure.
Despite our success, it would be irresponsible to give the impression that the smoothness of this procedure is the rule rather than the exception. In fact, of all the intracranial stents we have deployed (at this point, approximately 50), this is the only middle cerebral artery we have treated. On two other occasions, we attempted to track stents distal to the carotid siphon and were unsuccessful both times. Nevertheless, the experience we gained in other vessels has taught us some fundamental principles that optimize the chances of successfully completing this type of procedure.
The first issue is patient selection, and we cannot overemphasize the impact of an anatomically “friendly” intracranial carotid artery. In our patient, the curve of the carotid siphon had a rather smooth configuration, greatly facilitating stent tracking. Along these lines, we have found that it is almost imperative that the guiding catheter be as distal as possible in the cervical internal carotid artery and that the exchange guidewire be sufficiently distal in the middle cerebral artery to allow its support segment to be across the carotid siphon. It has been our experience that this does not cause undue discomfort for the patient. These recommendations clearly highlight the difficulty of treating patients with redundant extracranial internal carotid arteries, with coils and kinks that are likely to limit the ability to advance the guiding catheter close to the base of the skull. Also, once the exchange guidewire is anchored, the choice of interventional material is guided by the anatomic characteristics of the vessel being treated. Just as with conventional balloon angioplasty, we choose balloons that are undersized for the vessel treated, and our preference is a hydrophilic-coated moderately compliant coronary balloon. The one used in this case is clearly too long (ie, 20 mm), and we had to use it because we did not have a shorter one (ie, 10–15 mm) available that particular day. We chose to predilate the lesion, not only to facilitate crossing and deployment of the stent, but also as a means to test the response of the vessel to the balloon expansion, to assess the trackability of the interventional equipment, and to gauge the effect of balloon inflation on the patient. Another important point relates to the use of the microcatheter to cross the lesion. Although we do not use this technique routinely, it has certain advantages. The microcatheters are generally more trackable than the coronary balloons, thus allowing the distal access necessary to anchor the exchange wire. This is important because most exchange support wires are not optimal for crossing lesions initially owing to their overall stiffness, lesser torqueability, and tip characteristics.
The choice of stent is also guided by its trackability, deliverability, and flexibility after deployment. The Multilink Duet is a balloon-expandable stent with a tubular design consisting of multiple rings connected with multiple links to enhance hoop strength, while allowing longitudinal flexibility. It is an improved version of the original Multilink stent, allowing more visibility, excellent radial force, little recoil (<5%), and minimal shortening (<3%). We have found this stent to be easily deliverable to almost any intracranial location (Gomez CR et al, unpublished data). The only disadvantage we have seen is that the balloon must be expanded to 9 to 10 atm to assure stent detachment. Otherwise, its deployment and wide range of sizes makes it a very suitable stent for intracranial treatment purposes.
The demonstration of carotid endarterectomy as an effective method for reducing the risk of stroke in patients with significant extracranial atherosclerotic carotid artery lesions has made carotid revascularization the standard of care for these patients (12). Nevertheless, until recently, for patients with lesions that are not readily accessible to surgery, medical therapy has been the only therapeutic option. The existing literature suggests that the incidence of stroke in patients with middle cerebral artery stenosis is higher than that of patients with extracranial carotid stenosis, approaching 8% to 10% per year (13, 14). Also, approximately two thirds of these patients present with an unheralded stroke (14). The inherent risk of vessel dissection, however—distal embolization or rupture—has limited the widespread use of intracranial balloon angioplasty despite recent reports of increased patency rates and good outcomes (3, 15). Our case demonstrates that stenting of the middle cerebral artery is feasible, at least in selected cases, with current coronary technology. Whether stenting of this vessel is better than conventional balloon angioplasty or not remains to be determined.
Two issues that remain concern restenosis and acute occlusion. Clearly, stenting of smaller vessels is accompanied by a greater potential for restenosis. Part of this problem is related to the greater effect of natural intimal proliferation upon a smaller reference diameter, and we have called attention to this fact in relation to vertebral artery stenting (16). On the other hand, one of the factors associated with restenosis after coronary intervention is the degree of residual stenosis after the procedure. Here, it is possible that stenting proves superior to balloon angioplasty because of the improved angiographic outcomes. Also, the smaller lumen of the vessel increases the likelihood of acute thrombosis with complicating ischemia. In our experience, the best protective strategy against this problem is effective blockade of platelet aggregation by means of the combination of aspirin and clopidogrel.
Footnotes
↵1 Address for correspondence: Camilo R. Gomez, MD, Comprehensive Stroke Center, 1202 Jefferson Tower, 625 South 19th Street, Birmingham, AL 35294.
References
- Received August 10, 1999.
- Accepted after revision December 2, 1999.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Percutaneous transluminal angioplasty and stenting (PTAS) in patients with symptomatic intracranial vertebrobasilar artery stenosis (IVBS)
- Reporting standards for angioplasty and stent-assisted angioplasty for intracranial atherosclerosis
- Long term clinical and angiographic outcomes with the Wingspan stent for treatment of symptomatic 50-99% intracranial atherosclerosis: single center experience in 51 cases
- Reporting Standards for Angioplasty and Stent-Assisted Angioplasty for Intracranial Atherosclerosis
- The NIH registry on use of the Wingspan stent for symptomatic70-99% intracranial arterial stenosis
- Emerging Endovascular Therapies for Symptomatic Intracranial Atherosclerotic Disease
- Predictors of Ischemic Stroke in the Territory of a Symptomatic Intracranial Arterial Stenosis
- Elective stenting for symptomatic middle cerebral artery stenosis presenting as transient ischaemic deficits or stroke attacks: short term arteriographical and clinical outcome
- Stenting of Symptomatic M1 Stenosis of Middle Cerebral Artery: An Initial Experience of 40 Patients
- Urgent endovascular revascularization for symptomatic intracranial atherosclerotic stenosis
- Vertebral and Intracranial Artery Angioplasty
- Angioplasty and stenting for stroke prevention: Good questions that need answers
- Intracranial Cerebral Artery Disease as a Risk Factor for Central Nervous System Complications of Coronary Artery Bypass Graft Surgery