
Abstract
Summary: We present gross pathologic autopsy findings of a patient who was treated for two aneurysms with Guglielmi detachable coils (GDCs), and who died 33 months after the procedure. Histologic findings are also presented. In both aneurysms, the coils were firmly attached to the aneurysmal wall, making it impossible to remove them from the sac. The ostium of one aneurysm was covered by collagenous tissue and a single layer of endothelium.
Endovascular treatment with GDCs is an accepted method for treating intracranial aneurysms that otherwise would require more invasive surgery or could not be treated by surgery at all. Nevertheless, there is a paucity of information concerning histopathologic changes of coil-embolized aneurysms in human subjects over a long-term period. We report a case of a patient with two aneurysms that were successfully embolized with GDCs, and studied pathologically 33 months after treatment.
Case Report
A 34-year-old woman, a smoker of 40 cigarettes per day with systemic hypertension, was admitted to our hospital in June 1994 for treatment of a subarachnoid hemorrhage with a Hunt and Hess grade of 1.
CT showed blood in the left sylvian fissure, and a cerebral angiogram revealed bilateral middle cerebral arterial (MCA) aneurysms and a wide-neck right carotid ophthalmic aneurysm. The patient was considered for endovascular therapy, and we performed a successful embolization of the left MCA (probably the aneurysm that hemorrhaged) and the right carotid ophthalmic aneurysm with appropriately sized GDCs (Fig 1). The right MCA aneurysm could not be treated by endovascular therapy after a first attempt, because coils protruded into the parent artery. Surgical clipping was performed at another time.

Left ICA angiogram shows MCA aneurysm before (A) and after (B) embolization with GDC. Right ICA angiogram shows carotid ophthlamic aneurysm before (C) and after (D) embolization with GDC
During the postoperative period, the patient experienced thrombosis of the right renal artery. Laboratory investigation revealed no coagulative dysfunction. The patient was discharged, and a follow-up angiogram was scheduled to occur 1 year after treatment.
In June 1995, the control angiogram showed that the left MCA aneurysm remained fully occluded. Some coil compaction into the dome of the right carotid ophthalmic aneurysm occurred, resulting in recanalization (Fig 2). We tried to embolize this remnant, but this was not possible because coils protruded into the lumen of the parent artery. A follow-up angiogram was scheduled to occur 12 months after this procedure, but the patient refused further angiographic investigation. Clinical examination at that time was within normal limits.

Left ICA angiogram done 1year after GDC treatment of left MCA. Aneurysm remains completely occluded (A). Right ICA angiogram done 1 year after GDC treatment of right carotid ophthalmic aneurysm (B). There is some coil compaction and a small-neck remnant
In March 1997, the patient was admitted to our hospital in a semicomatose state with right hemiparesis. CT showed infarction in the territory of the left internal carotid artery (ICA). Two days after admission, the patient died.
Autopsy Findings
General autopsy revealed severe systemic atherosclerotic disease, pulmonary emphysema, and a sequel of previously documented thrombosis of the right renal artery.
External examination of the brain revealed infarction of the left cerebral hemisphere with subfacial herniation. Three saccular aneurysms were found after removal of the circle of Willis. One was at the level of the origin of the right ophthalmic artery, and the other two were located at the bifurcations of the MCAs.
Gross examination revealed severe atherosclerotic disease of the circle of Willis. There was no evidence of recent bleeding from the aneurysms. Sections through the left MCA and right carotid ophthalmic aneurysm were made, the coils were exposed, and the clip of the right MCA aneurysmal was also removed. The coils were firmly attached in the aneurysmal lumens, and it was not possible to remove them from the sac without compromising the histologic evaluation.
Histologic Study
Microscopic sections of two embolized aneurysms were stained with hematoxylin, eosin, and Masson trichrome after coil removal because a severe compaction made it difficult to obtain histologic slices.
As suggested by gross examination, the fundi of the two aneurysms were filled with a vascular fibrous connective tissue scar that were much more dense on the periphery of the sac where a proliferation of inflammatory cells was evident. Around the margins of the coils there was evidence of increased connective tissue cells, some macrophages, and a foreign-body response indicated by the presence of many multinucleated giant cells (Fig 3). There was no evidence of unorganized friable blood clots in the giant cells (Fig 3).

Pathologic findings of MCA aneurysm fundus. The cast of the coils, removed for cutting purposes, is completely surrounded by richly vascular fibrous tissue more cellular at the periphery of the fundus (star) and around the platinum coils (Hematoxilin and eosin stain; magnification ×200) (A). Many multinucleated foreign body giant cells are stretched along the coil casts, and some were released in the lumen of the coil casts (arrow), probably during coil removal for cutting purposes (Hematoxilin and eosin stain; magnification ×400) (B).
Because of the lack of a satisfactory specimen, it was only possible to examine the neck area of the right carotid ophthalmic aneurysm. A thick and dense layer of collagen tissue covered the aneurysmal neck, and a single layer of endothelial cells grew over the luminal surface of this connective tissue. Capillary growth proceeded from the lumen of the ICA into the aneurysm via the neck. Endothelial cell lining of these neovessels was continuous with the single layer of endothelial cells present over the surface of collagenous tissue that covered the neck. No endothelial cell layer continuous with the endothelial cells lining of the parent artery was seen (Fig 4).

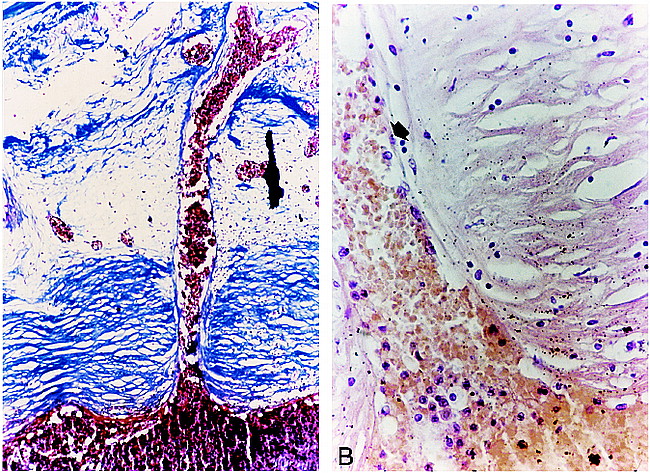
Histologic study of the aneurysm neck.
A, Capillary growth into the aneurysm neck (1) proceeded from the lumen of the ICA (P) via the neck. A thick and dense layer of collagen tissue aligned parallel to the long axis of the parent vessel, covering ostium (C) (Trichrome stain; magnification ×200).
B, Transition zone between the endothelial cell lining of neovessels and endothelial cells line the surface of the collagen tissue covering the neck. The neointima is organized in two layers. The most superficial layer comprises endothelium continuous with neovessels proceding from the lumen of the parent vessel (arrow). The deepest layer of neointima consited of dense vascular and collagenous fibrous tissue (C) (Hematoxilin and eosin stain; magnification ×400).
Discussion
The effects of GDCs in experimental aneurysms have been the subject of a number of animal studies. The results from these studies, however, probably cannot be applied directly to endovascular therapy in humans (1–3). Although GDCs are widely accepted as effective agents for intraaneurysmal coil embolization, there is a paucity of data concerning the long-term, histopathologic changes in coil-embolized aneurysms in humans.
Molineux et al (4) reported autopsy studies of two patients with wide-neck giant aneurysms treated by GDC 2 and 6 months after subtotal occlusion. In the two cases, the process of blood clot resolution into the sac did not occur, the coils were easily removed from the aneurysmal fundus, and there was no evidence of endothelial proliferation at the neck of the aneurysm.
Mizoi et al (5) reported the histologic findings 18 months after GDC embolization of a wide-neck (6-mm), large (2-cm) anterior communicating aneurysm treated in a two-stage embolization with GDC coils with subtotal occlusion. The intraluminal thrombus was poorly organized without fibrous tissue formation, and there was no endothelial proliferation covering the luminal surface of the thrombus.
Horowitz et al (6) presented autopsy findings, including electron and light microscopic studies of a basilar artery aneurysm that was successfully embolized with a GDC coil system 4 weeks before the patient died. The aneurysm's neck and fundus appeared to be isolated from the parent vessel by a thin film of fibrin that suggested the onset of endothelial growth.
In our case, the fundi of the two aneurysms were filled with vascular fibrous connective tissue scars that were much denser on the periphery of the sac. This fibrous tissue was permeated by inflammatory cells. There was no evidence of residual thrombus. Around the margins of the GDC coils there was increased cellularity in the connective tissue. Sections through the neck of one of these aneurysms (right carotid ophthalmic) revealed that the ostium was covered by a neointima organized in two layers. The superficial layer comprised endothelium continuous with that of endothelium extending from the lumen or the parent artery. The deeper layer of neointima consisted of dense, vascular, and collagenous fibrous tissue aligned parallel to the long axis of the parent vessel. These histologic findings are very similar to those reported by Mawad et al in canine aneurysms embolized with GDC coils (3). In our case, however, there was no evidence of smooth muscle cells in the neointima that covered the aneurysmal neck.
Capillary growth into the thrombus is probably the first step to the normal resolution of an aneurysm. This is followed by progressive invasion of inflammatory cells and deposition of vascular, fibrous connective tissue. If this does not occur, the process of clot resolution may be incomplete. In human aneurysms, the wall of the aneurysm has poor vascularity, is surrounded by an avascular subarachnoid space, and capillary regeneration may be slow. In our case, new vessel growth proceeded from the lumen of the parent vessel, but there was no evidence of vessels proceeding from the aneurysmal walls, as some investigators have reported (4).
There appears to be a simultaneous, progressive deposition of vascular, fibrous connective tissue into the aneurysm that, in our case, was much denser on the periphery and neck of the aneurysms as well as in the surrounding coils. The latter may have promoted the fibroblast invasion that, in turn, stimulated collagen production and the formation of mature connective tissue. The presence of mature cell growth around the aneurysmal periphery and coils might suggest that dense packing of intracranial aneurysms with GDCs enhances mature scar formation into the aneurysmal sac. The proliferation of a dense layer of collagen in the neck is probably the normal response of scar tissue during the maturation process in areas of stress that, in the case of intracranial aneurysms, could be represented by the blood flow pulsatility of parent vessels in this zone.
In this case report, we have demonstrated that complete resolution of blood clot occurred in two aneurysms examined 33 months after GDC treatment. Mature scar tissue formed in the aneurysmal lumens. In one of these aneurysms, we also were able to confirm the presence of a single layer of endothelial cells over the luminal surface of dense collagenous tissue that covered the aneurysmal neck. This was in the aneurysms in which angiographic examination 1 year earlier had demonstrated the presence of a small-neck remnant.
Conclusion
The principal concern in the follow-up of patients treated with GDC coils is the long-term clinical and angiographic effectiveness of this treatment. Our findings are encouraging for the use of the GDC technique and the improvement of embolic coil treatments for the enhanced healing of intracranial aneurysms. It is also important that efforts are made to obtain additional autopsy data from patients treated with GDC coils to assess the degree of occlusion and to understand better the effect of coil design on the formation of fibrosis and endothelization of the neck.
Footnotes
↵1 Address reprint requests to Enrique Castro, MD, Sección de Neurorradiología, Hospital General Universitario Gregorio Marañon, c/o Dr. Esquerdo, No 46, 28007 Madrid, Spain.
References
- Received April 17, 1998.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Mechanisms of Healing in Coiled Intracranial Aneurysms: A Review of the Literature
- A history of detachable coils: 1987-2012
- In Vivo Experimental Intracranial Aneurysm Models: A Systematic Review
- Cerecyte versus Platinum Coils in the Treatment of Intracranial Aneurysms: Packing Attenuation and Clinical and Angiographic Midterm Results
- Computerized Assessment of Angiographic Occlusion Rate and Coil Density in Embolized Human Cerebral Aneurysms
- Stent-Assisted Reconstructive Endovascular Repair of Cranial Fusiform Atherosclerotic and Dissecting Aneurysms: Long-Term Clinical and Angiographic Follow-Up
- Brain Aneurysms and Arteriovenous Malformations: Advancements and Emerging Treatments in Endovascular Embolization
- Matrix and Bioabsorbable Polymeric Coils Accelerate Healing of Intracranial Aneurysms: Long-Term Experimental Study
- Histological Findings in Ruptured Aneurysms Treated with GDCs: Six Examples at Varying Times after Treatment
- Endovascular Microcoil Gene Delivery Using Immobilized Anti-adenovirus Antibody for Vector Tethering
- Cellular Responses of Bioabsorbable Polymeric Material and Guglielmi Detachable Coil in Experimental Aneurysms
- Role of Electrothrombosis in Aneurysm Treatment with Guglielmi Detachable Coils: An In Vitro Scanning Electron Microscopic Study
- Delivery of Human Vascular Endothelial Growth Factor with Platinum Coils Enhances Wall Thickening and Coil Impregnation in a Rat Aneurysm Model
- Delayed Reconfiguration of a Guglielmi Detachable Coil Mass Associated with Late Occlusion of an Adjacent Aneurysm and Parent Vessel
- Endovascular Treatment of Ruptured Posterior Circulation Cerebral Aneurysms : Clinical and Angiographic Outcomes
- INTERVENTIONAL NEURORADIOLOGY