
Abstract
BACKGROUND AND PURPOSE: The characteristics of hypoperfusion in the supratentorial region of patients with brain stem infarction are unclear. We investigated the relationships between the presence of hypoperfusion and the location, number, and size of the infarcts with xenon contrast-enhanced CT.
METHODS: One hundred five patients with brain stem infarction detected by MR imaging underwent xenon contrast-enhanced CT to measure the regional CBF (rCBF) in the frontal, temporal, parietal, and occipital regions and in the putamen and thalamus. A decrease of more than 10% from the mean rCBF value for normal individuals was considered to indicate hypoperfusion.
RESULTS: Thirty-six patients had supratentorial hypoperfusion. The mean rCBF values (measured in mL/100 g/minute) were as follows: frontal region, 36.2 ± 5.1 (−14.8%, n = 28); parietal region, 42.3 ± 4.7 (−19.1%, n = 29); temporal region, 41.5 ± 2.8 (−12.6%, n = 12); and thalamus, 50.1 ± 3.2 (−19.6%, n = 7). Supratentorial hypoperfusion was associated with pontine infarction in 33 patients (upper pons in 15, middle pons in 18, and lower pons in seven), midbrain infarction in two, and medulla infarction in one. Twenty-three patients had infarcts that were larger than 5 mm, and 11 had infarcts that were 2 to 5 mm. Only two had infarcts that were smaller than 2 mm. Seven patients each had one infarct, 13 each had two, and 16 each had three.
CONCLUSION: Supratentorial hypoperfusion was associated with larger infarcts, with more infarcts, and with pontine infarction.
Crossed cerebellar diaschisis, cerebello-cerebral diaschisis, and pontocerebellar diaschisis are well known (1–6). In contrast, diaschisis in the supratentorial region of patients with brain stem infarction has received little attention (7–10) and may not satisfy the accepted definition of diaschisis, which is the loss of function and electrical activity caused by cerebral lesions in areas that are remote but neuronally connected to the lesion. Moreover, these studies conflict, mainly because a limited number of patients were included and regional CBF (rCBF) was evaluated by single-photon-emission CT (SPECT), which provides only low spatial resolution and does not always measure the absolute value of rCBF. Investigation of such rare supratentorial hypoperfusion requires a suitable method for the measurement of CBF in a large number of patients with brain stem infarction. Xenon contrast-enhanced CT (Xe-CT) has high spatial resolution compatible with positron-emission tomography and can conveniently measure the value of rCBF (11). In this study, we attempted to detect hypoperfusion in the remote areas of the supratentorial region in a large number of patients with brain stem infarction by using Xe-CT to evaluate the incidence, location, and degree of the hypoperfusion.
Methods
This study included 105 patients (69 men, 36 women; age, 43–86 years; mean age, 63.9 ± 9.1 years) who were admitted to Nasu Neurosurgical Center and Kofu Johnan Hospital between 1992 and 1997 with the diagnosis of brain stem infarction based on MR imaging findings of areas of low intensity on T1-weighted images and high intensity on T2-weighted images. Patients with brain stem infarction associated with white matter lesion of grades III and IV (12) and lacunar infarction in the basal ganglia were excluded from this study. Fifteen healthy individuals (nine men, six women; age, 59–79 years; mean age, 65.2 ± 7.6 years) with no history of cerebrovascular diseases or risk factors for cerebrovascular diseases comprised the control group for the rCBF studies. There was no significant difference in mean age between the two groups (12). There was no significant difference in mean arterial blood pressure and arterial carbon dioxide tension between the patients and control subjects. Informed consent was obtained from all control subjects. Patients underwent MR imaging (all patients); MR angiography (41 patients); digital subtraction angiography (29 patients); or both MR angiography and digital subtraction angiography (22 patients); and Xe-CT (all patients). Control subjects underwent only MR angiography.
MR imaging was performed at 0 to 12 days (mean, 3.7 days) after onset. MR imaging used a spin-echo protocol for T1-weighted imaging with 600/15 (TR/TE) and for T2-weighted imaging with 300/80 in the orbitomeatal plane with 7.5-mm section thickness (1.5-T MRT-200 Fx-super system; Toshiba, Tokyo, Japan). The display matrix was 256 × 256. The locations of the brain stem infarcts were classified into six groups: midbrain, upper pons, middle pons, lower pons, medulla, and combinations. The number of infarcts and infarct sizes (smaller than 2 mm, 2–5 mm, or larger than 5 mm) were also observed.
Xe-CT examination was performed at 0 to 24 days (mean, 6.8 days) after onset using an Xpeed CT scanner (Toshiba). Patients and control subjects inhaled a mixture of 30% xenon in oxygen for 4 minutes, during which a series of 8-second CT scans was obtained parallel to the orbitomeatal line. Circular regions of interest (ROI) with a diameter of 1.0 cm were selected for patients and for normal individuals (three ROI in each of the frontal, temporal, parietal, and occipital regions and two ROI each in the putamen and thalamus). Great care was taken so that the ROI did not include white matter in the frontal, temporal, parietal, or occipital regions (Fig 1). Values of rCBF were calculated by averaging fi values in these ROI. An AZ-7000 image processing system (Anzai Corp., Tokyo, Japan) was used to calculate rCBF values with the end tidal chamber scan method. The confidential image was used to detect motion artifacts. The 6 × 6 filter was also used. During the procedure, xenon and carbon dioxide concentrations in the expired gas were monitored. The xenon concentrations in arterial blood flow were estimated from the end tidal xenon concentration and hematocrit value. CBF values were calculated by fitting the Ketty equation to the time-attenuation curves of brain CT number and arterial CT number using the least-squares method (11).

Circular regions of interest with diameters of 1.0 cm were placed in the frontal, temporal, parietal, and occipital cortices and also in the putamen and thalamus.
A decrease of more than 10% from the mean rCBF value of normal individuals was considered to indicate significant supratentorial hypoperfusion (13–15). The relationship between the occurrence of supratentorial hypoperfusion and the location, number, and size of infarcts in patients and the difference in rCBF values between patients and normal individuals were evaluated. Statistical analysis was conducted using the Student t test, and Bonferroni analysis was conducted after the analysis of variance test.
Results
Thirty-six (34.3%) of the 105 patients had supratentorial hypoperfusion. Supratentorial hypoperfusion was detected in one ROI in each of 11 patients, in two ROI in each of nine patients, and in three ROI in each of 16 patients. Supratentorial hypoperfusion occurred most frequently in the frontal (28 cases) and parietal (29 cases) regions and was much less common in other regions. Supratentorial hypoperfusion was recognized ipsilateral to the brain stem infarction.
Supratentorial hypoperfusion was associated with pontine infarction in 33 of the 36 patients. The other patients had midbrain (two) and medulla (one) infarction. Infarction was located in the middle pons in 18 of the 33 patients, in the upper pons in 15 patients, and in the lower pons in seven patients. Twenty-three patients had infarcts larger than 5 mm, and 11 patients had infarcts that were 2 to 5 mm. Only two patients had infarcts smaller than 2 mm. Seven patients each had one infarct, 13 patients each had two infarcts, and 16 patients each had three infarcts (Table).
Location, size, and number of infarctions, clinical signs, and presence of arterial lesions in the 36 patients with supratentorial diaschisis
The mean CBF values were measured in mL/100 g/minute and are presented herein. The mean CBF values in normal individuals (n = 15) were as follows: frontal region, 42.5 ± 4.3; parietal region, 52.3 ± 4.1; temporal region, 47.5 ± 3.9; occipital region, 43.1 ± 4.8; thalamus, 62.3 ± 5.6; and putamen, 42.4 ± 3.7. The mean CBF values in patients with supratentorial hypoperfusion were as follows: frontal region, 36.2 ± 5.1 (−14.8%, n = 28); parietal region, 42.3 ± 4.7 (−19.1%, n = 29); temporal region, 41.5 ± 2.8 (−12.6%, n = 12); and thalamus, 50.1 ± 3.2 (−19.6%, n = 7). The mean CBF value in the frontal region of patients with hypoperfusion and upper pontine infarction was 37.1 ± 3.9 (n = 9) and in patients with middle pontine infarction was 35.8 ± 4.2 (n = 8). The mean CBF value in the parietal region of patients with hypoperfusion and upper pontine infarction was 43.6 ± 4.5 (n = 9) and in patients with middle pontine infarction was 42.8 ± 5.1 (n = 9). There were no significant differences based on location of infarction. The mean CBF value in the frontal region of patients with infarcts that were 2 to 5 mm was 36.8 ± 5.1 (n = 7) and in patients with infarcts that were larger than 5 mm was 33.2 ± 2.7 (n = 19). The mean CBF value in the parietal region of patients with infarcts that were 2 to 5 mm was 45.9 ± 5.2 (n = 10) and in patients with infarcts that were larger than 5 mm was 42.2 ± 2.9 (n = 18). There were no significant differences based on size of infarct. The mean CBF value in the frontal lobe of patients with two infarcts was 36.2 ± 3.5 (n = 10) and with three infarcts was 35.1 ± 2.8 (n = 13). The mean CBF value in the parietal region of patients with one infarct was 46.8 ± 5.2 (n = 7), with two infarcts was 40.3 ± 3.9 (n = 8), and with three infarcts was 38.2 ± 4.1 (n = 11). There was a significant difference between mean CBF values with one infarct and with two and three infarcts (analysis of variance, F = 15.70; P = .0001; Bonferroni t = 2.58202). A representative case is shown in Figures 2 through 4.

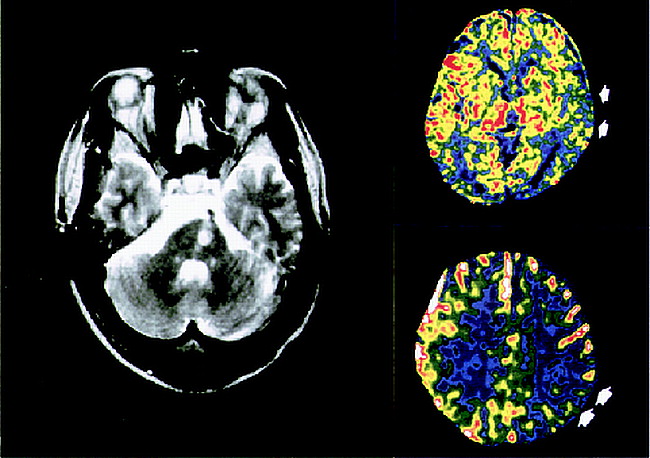
MR image of a 70-year-old man with right hemiparesis and dysarthria shows left middle pontine infarct of 4.5 mm. Xe-CT scans show left parietotemporal hypoperfusion (arrows).

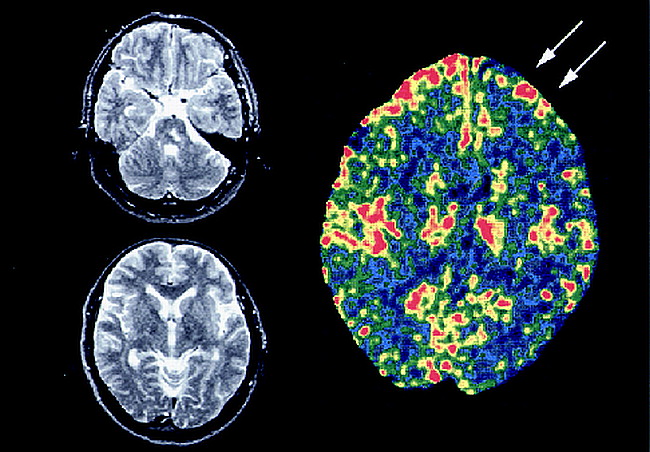
MR images of a 56-year-old woman with mild right hemiparesis show left upper pontine infarct of 40 mm but no lacunar infarction in the supratentorial region. Xe-CT scan shows left frontal hypoperfusion (arrows).

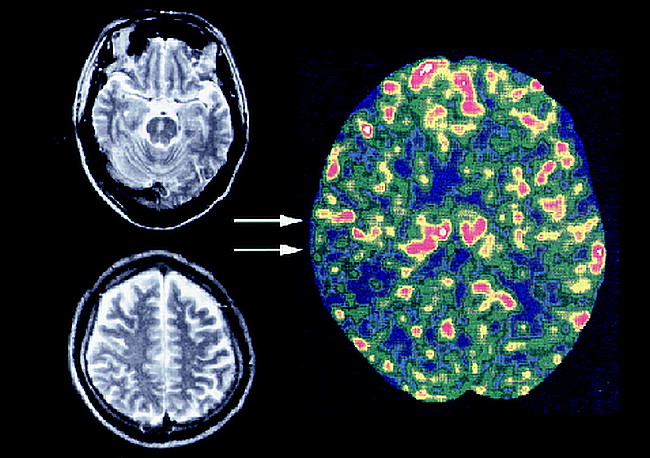
MR images of a 65-year-old man with sensory disturbance and dysarthria show right middle pontine infarct of 5.5 mm but no infarction in the supratentorial region. Xe-CT scan shows right temporal hypoperfusion (arrows).
Discussion
Hypoperfusion was detected in the supratentorial region of 34.3% of patients with brain stem infarction. The causative factors that lead to one third of the patients having supratentorial hypoperfusion remain unknown, but the size, number, and location of the brain stem infarcts may affect the occurrence of hypoperfusion. A SPECT study found that the frequency of the supratentorial diaschisis was 33.3% in patients with brain stem infarction (7). These incidences are somewhat lower than those found in patients with crossed cerebellar diaschisis, which ranges from 50% to 70% (1, 16–22). We found that supratentorial diaschisis frequently occurred in the frontal and parietal regions but rarely in the putamen and occipital regions. SPECT has also disclosed that supratentorial hypoperfusion occurs in the ipsilateral frontoparietal region (7). Our results also disclosed that supratentorial hypoperfusion was recognized in the ipsilateral side. Supratentorial hypoperfusion, however, was also recognized at the ipsilateral side in patients with midbrain and upper pontine infarction and at the contralateral side in patients with middle pontine to medulla infarction (23). The cause of this discrepancy is unknown and presumably depends on the different methods employed. Fiber connections between the cortex and pons arise from the frontal, temporal, parietal, and occipital cortices. The most important contributions, however, arise in areas 4, 3, 1, 2, and 5 in the monkey (24), which may explain the location of supratentorial diaschisis. Supratentorial diaschisis was most commonly associated with pontine infarction (91.7%), more frequently with middle and upper pontine infarction than with lower pontine infarction. The relationship between the sites of infarction and supratentorial diaschisis is unclear. Two patients with midbrain infarction had diaschisis (in the frontoparietal region and the frontoparietal temporal region), and one patient with medulla infarction also had frontoparietal thalamic diaschisis. Two previous patients with lateral medullary infarction had hemispheric hypoperfusion (8).
A greater number of infarcts was significantly associated with severe hypoperfusion. Although there was no significant difference, larger infarct size tended to be correlated with severity of hypoperfusion. Large or multiple infarcts are likely to involve the fiber connections between the cortex and pons and lead to hypoactivity in the cortex.
Supratentorial hypoperfusion was associated with a decrease from −12.6% to −19.6% in rCBF compared with the values of normal individuals. The values of normal individuals were selected rather than the values of normal areas in the patients because areas that seemed to be normal may also have had hypoperfusion considering that the contralateral side was found to be hypoperfused (23). The reduction was high in the parietal region and thalamus. The reduction in the thalamus might be caused by deactivation of the corticothalamic pathway. The SPECT asymmetry index showed that the reduction varied from −2.77% to −5.36% in patients with upper pontine infarction (7) and from 25% to 45.7% compared with the opposite side in patients with crossed cerebellar diaschisis (22). Nevertheless, these results cannot be simply compared because the standard of measurement is different.
Conclusion
The severity of supratentorial hypoperfusion was not related to the location of the infarction; there was no significant difference in the frontal and parietal regions between patients with upper and middle pontine infarction. Larger infarction tended to be associated with more severe hypoperfusion, but there was no significant correlation. Severity of hypoperfusion was also significantly associated with number of infarcts. Although no correlation between hypoperfusion and infarction volume was observed in patients with crossed cerebellar diaschisis (25), a larger number of infarcts will cause more damage to connection fibers and may lead to severe reduction of rCBF in patients with supratentorial hypoperfusion.
Footnotes
↵1 This work was presented in part at the Joint 3rd World Stroke Congress and 5th European Stroke Conference, Berlin, Germany, 1996.
↵2 Address reprint requests to Nobuhiko Miyazawa, MD, Department of Neurosurgery, Yamanashi Medical University, 1110 Shimokatoh, Tamaho-machi, Nakakoma-gun, Yamanashi 409-3898, Japan.
References
- Received October 29, 1998.
- Accepted after revision June 22, 1999.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.