
Abstract
SUMMARY: Trigeminal neuralgia is a debilitating condition with numerous etiologies. In this retrospective case series, we report a cohort of patients with a rarely described entity, absence of Meckel cave, and propose this as a rare cause of trigeminal neuralgia. A search of the electronic medical record was performed between 2000 and 2020 to identify MR imaging reports with terms including “Meckel’s cave” and “hypoplasia,” “atresia,” “collapse,” or “asymmetry.” Images were reviewed by 2 blinded, board-certified neuroradiologists. Seven cases of the absence of Meckel cave were identified. Seven patients (100%) had ipsilateral trigeminal neuralgia and ipsilateral trigeminal nerve atrophy, suggesting an association between absence of Meckel cave and trigeminal neuralgia. Absence of Meckel cave is a rare entity of unknown etiology, with few existing reports that suggest the possibility of an association with trigeminal neuralgia. Its recognition may have important implications in patient management. Future studies and longitudinal data are needed to assess treatment outcomes and added risks from surgical intervention in these patients.
ABBREVIATION:
- TN
- trigeminal neuralgia
Trigeminal neuralgia (TN) is a debilitating condition resulting in a severely compromised quality of life in affected people.1 It more commonly affects women and has an overall prevalence of 0.07% of the population.2 Treatment of TN revolves around accurate identification of the potential etiology. Advances in neuroimaging, particularly MR imaging, have played a crucial role in assessing various structural causes of TN, such as neurovascular compression, compressive mass, or multiple sclerosis.3 Depending on the suspected etiology, various treatment options may be used, including medication, neurovascular decompression, stereotactic radiosurgery, or percutaneous balloon compression.
A rarely reported entity, absence of Meckel cave, has been described in a few patients with TN, including 2 case reports and 3 patient case series.4⇓-6 Most important, there are only a few reports, to our knowledge, on the absence of Meckel cave in patients other than those with TN. This retrospective study aimed to demonstrate the potential relationship of an absent Meckel cave with TN versus without TN, which may have important diagnostic and treatment implications.
MATERIALS AND METHODS
Study Population and Data Collection
This retrospective observational study was approved by the Mayo Clinic institutional review board. MR imaging brain radiology reports were searched from 2000 to 2020. Search terms included “Meckel’s cave” AND “collapse” OR “atresia” OR “hypoplasia” OR “atretic” or “asymmetry.” The search identified a total of 169 unique records. The search results were manually refined after reading all MR imaging brain reports thoroughly to determine whether patients had any relevant abnormality of a Meckel cave that warranted imaging review. Those with irrelevant abnormalities reported (eg, Meckel cave meningocele) were dismissed, leaving 24 patients with reports that potentially met the inclusion criteria for further imaging review. Additionally, relevant clinical data were collected, including basic demographics, medical and surgical history, and outcomes.
Imaging
All patients underwent MR imaging (3 patients on a 1.5T and 4 patients on a 3T MR imaging scanner). One patient had imaging performed only at an outside facility before any intervention at our institution. All patients had imaging with and without intravenous gadolinium contrast. Six patients had dedicated high-resolution imaging of the posterior fossa that included a high-resolution, heavily T2-weighted sequence (eg, CISS, FIESTA, sampling perfection with application-optimized contrasts by using different flip angle evolution [SPACE sequence; Siemens]).
Image Analysis
All patients with a reported Meckel cave abnormality had their MR imaging independently re-evaluated by 2 board-certified neuroradiologists who were blinded to the clinical information for confirmation of the absence of a Meckel cave and the presence of any additional apparent cause for trigeminal neuralgia, such as neurovascular compression, mass lesion, brainstem lesion, and so forth. A third board-certified neuroradiologist was available to decide discrepancies. Absence of Meckel cave was defined by a complete absence of fluid signal on T2-weighted images. We also evaluated associated congenital or ac-quired abnormalities along the course of cranial nerve V and its major branches, such as skull base abnormalities, atrophy or absence of V2–V3 branches, abnormality in the superior orbital fissure along the course of V1, or atrophy of muscles of mastication. The electronic medical records of included patients were screened for demographics and clinical notes, including the presence of a trigeminal neuralgia diagnosis as well as trigeminal nerve atrophy on imaging. Cross-sectional diameter and the area of each trigeminal nerve were measured in an oblique coronal plane that was aligned perpendicular to the axis of each nerve. The nerve was measured at the midpoint of the cisternal segment of the nerve.
Statistical Analysis
Simple descriptive statistics such as measures of central tendency and dispersion were calculated using SPSS, Version 20 (IBM). When we compared the mean difference of 2 continuous variables, normality testing (eg, the Kolmogorov-Smirnov test) was run and then the appropriate nonparametric and parametric test was used (eg, paired t test).
RESULTS
Seven patients were identified with an absent Meckel cave (Fig 1) confirmed on MR imaging. Summary information is de-tailed in the Online Supplemental Data. There were 7 women, with a mean age of 46.6 (SD, 14.1) years (range, 36–80 years). Of the 7 patients with an absent Meckel cave, 5 Meckel caves were absent on the right (71.4%) and 2 were absent on the left (28.6%). There was also trigeminal nerve atrophy (Fig 2 and Online Supplemental Data) on the same side as the absent Meckel cave in all 7 patients (100%). The mean cross-sectional area of the trigeminal nerve ipsilateral to the side of the absent Meckel cave (mean, 3.9 [SD, 0.9] mm2) was less than the contralateral one (mean, 6.4 [SD, 1.5] mm2), and this difference was found to be statistically significant on a paired t test (P value < .001). Most important, no other plausible structural causes of TN, such as neurovascular compression, were found in these patients. In all cases, the main branches of the trigeminal nerve (V2–V3) were present and symmetric. Because V1 is commonly not directly visualized on standard MR imaging, evaluation was limited, but no appreciable abnormality was present in the superior orbital fissure.

Postcontrast coronal T1- (A) and coronal T2-weighted SPACE images (B) in 1 patient show the absence of Meckel cave (arrow) compared with the normal side (arrowhead). In another patient, postcontrast coronal T1- (C) and coronal T2-weighted SPACE images (D) show absence of Meckel cave (arrow) compared with the normal side (arrowhead).

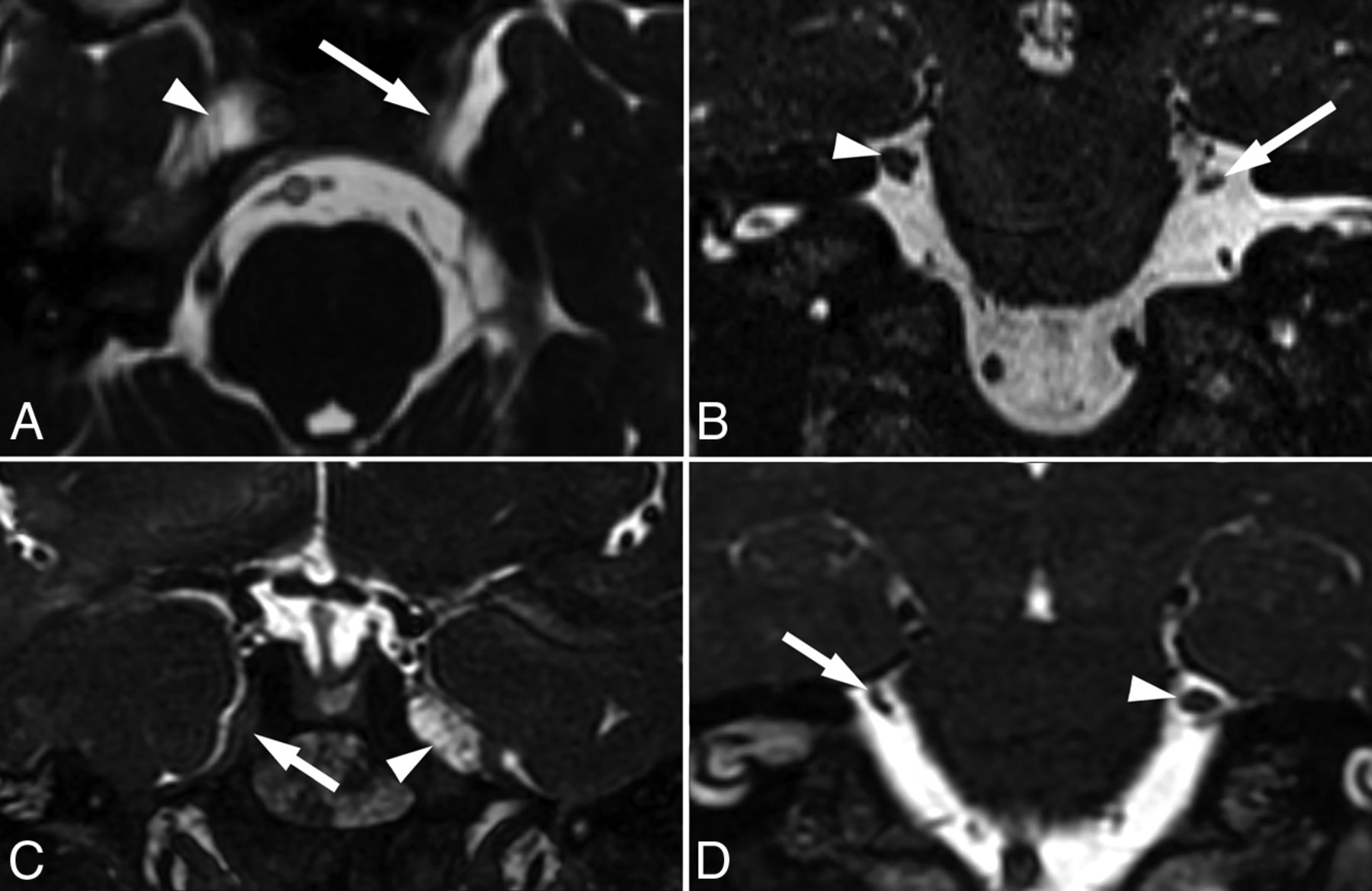
A, Axial CISS image shows absence of Meckel cave on the left (arrow) compared with the normal right Meckel cave (arrowhead). B, Coronal CISS image in the same patient shows atrophy of the left trigeminal nerve (arrow) compared with the normal nerve on the right (arrowhead). In another patient, coronal CISS image (C) shows absence of Meckel cave on the right (arrow) compared with the normal left Meckel cave (arrowhead). D, Coronal CISS image in the same patient shows atrophy of the right trigeminal nerve (arrow) compared with the normal nerve on the left (arrowhead).
TN was present in all 7 patients (100%) and was ipsilateral to the absent Meckel cave in all 7 patients (100%). One patient initially presented with facial numbness in a V1 and V2 distribution, which subsequently developed into trigeminal neuralgia in the ensuing years, with progressive nerve atrophy compared with previous scans. There were 2 patients with a reported history of idiopathic intracranial hypertension. One patient was reported to have idiopathic intracranial hypertension and Bell palsy during pregnancy 18 years before the evaluation for TN (11 years before the TN onset) but had no evidence of elevated intracranial pressure at the time of our evaluation. A second patient had a reported history of presumptive idiopathic intracranial hypertension based on clinical symptoms before her evaluation at our institution, but there was no evidence of papilledema on subsequent fundoscopic examination by ophthalmology and no evidence of elevated opening pressure.
Six of 7 (86%) patients were naïve to any interventional treatment technique for TN at the time of identification of the absent Meckel cave. One patient had undergone prior microvascular decompression at an outside institution, and preoperative imaging was unavailable. TN was initially treated medically in all patients using carbamazepine or gabapentin. In some patients, other medications such as tramadol, topiramate, or other benzodiazepines were used. Six patients (85.7%) had follow-up within the 6 months of diagnosis, with 4 having improvement (66.7%) and 2 having no improvement (33.3%) with medical therapy. Three of the 4 with initial improvement subsequently had a recurrence of symptoms and were considered medication refractory.
After the initial imaging at our institution, 1 patient was treated with microvascular decompression for suspected neurovascular compression with negative findings on imaging due to typical clinical symptoms. Additionally, 1 patient underwent rhizotomy, and 1 had stereotactic radiosurgery. Both patients who underwent surgery had no appreciable neurovascular compression found on exploration (1 before presentation at our facility and 1 at our facility). Both microvascular decompressions ultimately failed after an initial minor improvement. One patient had subsequent balloon compression, and 1 had subsequent stereotactic radiosurgery, which were safely performed. The patient with balloon compression had a positive response to therapy. The patient treated with postoperative stereotactic radiosurgery was lost to follow-up. The patient treated with stereotactic radiosurgery alone had an adequate response, while the patient treated with the rhizotomy had recurrence of TN symptoms.
DISCUSSION
Absence of a Meckel cave is an uncommon imaging finding associated with TN. A few reported cases of this entity have been shown in patients with TN, including 1 case report and a series of 3 cases.4⇓-6 Our case series presents 7 patients with absence of a Meckel cave, in which all subjects had atrophy of the ipsilateral trigeminal nerve and ipsilateral TN. No patients with an absent Meckel cave were asymptomatic. Recognition of this entity as a potential cause of TN may have important diagnostic and treatment considerations.
The Meckel cave is a CSF-filled space approximately 4 × 9 mm wide at its opening and 15 mm in length, located in the middle cranial fossa, serving as a channel for the trigeminal nerve between the prepontine cistern and the cavernous sinus, housing the Gasserian ganglion.7 Neuroimaging of the Meckel cave is frequently performed to identify a potential cause of trigeminal neuropathy. The Meckel cave is involved in a variety of congenital, infectious, inflammatory, vascular, and neoplastic pathologies.7,8
Absence of a Meckel cave is poorly understood and rarely reported. Before our series, few reported cases of an absent Meckel cave have been associated with ipsilateral TN without any prior surgical intervention on the cave.4⇓-6 A hypoplastic or absent Meckel cave has been occasionally described in the setting of congenital hypoplasia or aplasia of the trigeminal nerve; however, these cases have some key differences from our patients.9,10 In contrast to our cohort, patients in these prior reports had symptoms that typically presented in early life and manifested as trigeminal neuropathy rather than neuralgia—commonly anesthesia in the trigeminal distribution and resulting neurotrophic keratitis.9,10 Additionally, 1 patient in our cohort had progressive symptoms correlated with progressive atrophy of the trigeminal nerve, which suggest a potentially acquired etiology. In our institutional records, we found no descriptions of Meckel cave absence or its descriptive equivalents—such as total collapse or aplasia—in subjects without TN or contralateral TN. The evidence thus far, however scant, points to an etiologic implication of this entity in TN. Additionally, the otherwise normal structure and function of the trigeminal nerve and lack of other associated orofacial developmental abnormalities strongly suggest that absence or marked diminution of a Meckel cave is either an acquired contraction or a primary failure of establishment of the subarachnoid space in the cave. None of our patients had a history of craniofacial herpes zoster, meningitis, or other diagnosed inflammatory process. Additionally, only 1 patient had a history of prior intracranial surgery—unfortunately, lack of available preoperative imaging makes it uncertain whether absence of Meckel cave was present before surgery. Most important, the operative note reports that there was an atrophic nerve with no evidence of neurovascular compression. Patients were all also naïve to any direct procedure on the trigeminal nerve or ganglion for TN relief. The onset of TN was also insidious, as typically seen in TN secondary to vascular impingement.
Regarding the alternative possibility of primary failure of development of the CSF space in the cave, the onset of TN late in life may be due to changes in dural compliance and thickness, leading to progressive compression of the ganglion with aging.11 Experimental constriction of the peripheral nerves has been shown to result in cytokine-mediated sensitization of the dorsal root ganglion by up-regulation of voltage-gated sodium channels. A similar mechanism has been suspected in compressive radiculopathy by herniated discs.12 The arachnoid membrane continues from the posterior fossa into the Meckel cave, forming a CSF compartment within the cave, and extends along the nerve rootlets anteriorly to the Gasserian ganglion. The presence of surrounding CSF appears to play a critical role in the physiology and health of the sensory ganglia. Dorsal root ganglia of the spinal cord are also surrounded by a thin layer of CSF carried along the perineural sheath, and transport of intrathecal India ink particles and gene vector particles to the dorsal root ganglia is well-established.13
Schwann cell damage, loss of peripheral myelin, and endothelial and smooth muscle degeneration with increased collagen in the wall of the trigeminal arterioles have all been reported in patients with TN.14 Loss of surrounding CSF could lead to impairment of normal myelin and vascular repair mechanisms in the ganglia. CSF may be a normal pathway for clearance of proinflammatory cytokines such as tumor necrosis factor-α, which are known to upregulate voltage-gated sodium channels leading to the increased or ectopic firing of ganglionic neurons.15 Collapse of a Meckel cave is known to occur in spontaneous intracranial hypotension secondary to CSF hypovolemia. Facial pain and dysesthesia commonly accompany headache in spontaneous intracranial hypotension. It is entirely conceivable that the loss of CSF in a Meckel cave could play a similar role in developing trigeminal nerve hypersensitivity in spontaneous intracranial hypotension.
Our cohort had a mean age of 46.6 years, and all were women. This is in agreement with the previous reported mean ages of patients with classic TN (53 years) and secondary TN (43 years).16,17 Likewise, the incidence of TN is higher in women.18,19 The clinical presentation was similar to the more common etiologies. All patients presented with the classic electric shock-like pain along the nerve distribution and had various stimuli beyond the region of pain triggering their episodes. Most interesting, 1 patient presented with symptoms of trigeminal neuropathy with facial numbness along the V2 and V3 distributions 6 years before development of TN. On imaging, this patient had progressive trigeminal nerve atrophy across the time course of developing TN symptoms.
TN in these cases appeared to be mostly refractory to medical and procedural treatment. Microvascular decompression was not helpful in alleviating TN, and a better symptomatic response was observed after balloon compression or stereotactic radiosurgery. It is conceivable that inflation of the balloon might restore the CSF space in a Meckel cave.
Several limitations are noteworthy. The small number of patients and retrospective nature of the study limit the ability to determine causation of the absence of a Meckel cave with TN, though 100% of patients did have TN. Additionally, few surgical interventions were performed with no randomization or blinding. Thus, appropriate management of these patients cannot be completely determined, and future studies will be needed to better understand treatment outcomes. There were also limitations with imaging, such as lack of standardized protocol with 1 patient not having high-resolution CISS-like sequence or the equivalent.
CONCLUSIONS
Absence of Meckel cave is a rare entity associated with TN. Our study highlights 7 cases, adding to the previous literature of 4 cases. Despite our findings, the etiology remains unknown, and further studies and longitudinal data are needed to assess various treatment outcomes and added risks in patients. Importantly, the decision to pursue balloon compression of the ganglion versus radiation or microvascular decompression should be carefully considered, and neuroimaging plays a vital role in diagnosing this rare entity.
Footnotes
A. Jain and M.S. Muneer contributed equally to this work.
Disclosures: Erik H. Middlebrooks—UNRELATED: Consultancy: Varian Medical Systems Inc, Boston Scientific Corp. Sanjeet S. Grewal—UNRELATED: Consultancy: Medtronic, Boston Scientific Corp.
References
- Received January 20, 2021.
- Accepted after revision April 20, 2021.
- © 2021 by American Journal of Neuroradiology




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.