
Abstract
BACKGROUND AND PURPOSE: Spinal CSF leaks cause spontaneous intracranial hypotension. Several types of leaks have been identified, and one of these types is the lateral dural tear. Performing myelography with the patient in the decubitus position allows precise characterization of these leaks. The purpose of the current study was to describe the different variants of spontaneous lateral CSF leaks.
MATERIALS AND METHODS: This retrospective cohort study included a consecutive group of patients with spontaneous intracranial hypotension and lateral CSF leaks who underwent digital subtraction myelography in the decubitus position and underwent surgery to repair the CSF leak between July 2018 and June 2023.
RESULTS: The mean age of the 53 patients (37 women and 16 men) was 35.5 years. Three different variants of lateral CSF leak could be identified. Forty-nine patients (92.5%) had a lateral dural tear associated with the nerve root sleeve. The dural tear was at the axilla of the nerve root sleeve in 36 patients (67.9%) and at the shoulder in 13 patients (24.5%). Four patients (7.5%) had a lateral dural tear at the level of the pedicle that was not associated with the nerve root sleeve. Findings on digital subtraction myelography were concordant with intraoperative findings in all patients. An extradural CSF collection was seen in all patients with a lateral dural tear associated with the nerve root sleeve but in only 2 of the 4 patients with the pedicular variant of a lateral dural tear.
CONCLUSIONS: We identified 3 variants of spontaneous lateral dural tears. Most lateral dural tears are associated with extradural CSF collections and arise from either the axilla (67.9%) or the shoulder (24.5%) of the nerve root sleeve. Lateral dural tears at the level of the pedicle (7.5%) not associated with the nerve root sleeve are uncommon and may require specialized imaging for their detection.
ABBREVIATIONS:
- DSM
- digital subtraction myelography
- SIH
- spontaneous intracranial hypotension
SUMMARY
Previous literature
Spontaneous intracranial hypotension can cause debilitating headaches and various other more or less serious neurologic symptoms. The underlying cause is almost always a CSF leak at the level of the spine and several types of CSF leak have been identified. The lateral dural tear is a well-known type of spinal CSF leak causing spontaneous intracranial hypotension, but this type has not been studied in detail.
Key findings
Digital subtraction myelography and intra-operative observations in 53 patients distinguished three variants of lateral CSF leak, the shoulder and axillary variants associated with the nerve root sleeve and the uncommon pedicular variant not associated with the nerve root sleeve. Extensive extradural CSF collections were present in the great majority of patients but no extradural CSF could be identified on conventional spine imaging in half of the patients with the pedicular type of lateral CSF leak.
Knowledge advancement
Three distinct variants of lateral dural tears can be identified as the cause of spontaneous intracranial hypotension.
Spontaneous intracranial hypotension (SIH) is an increasingly recognized disorder with an incidence of about 4 per 100,00 per year.1,2 In addition to the prototypical symptom of orthostatic headache, a wide variety of other clinical manifestations have been reported.3 In most patients, a spontaneous leak of CSF at the level of the spine is responsible for SIH.3 With the advent of specialized spinal imaging techniques, such as digital subtraction myelography (DSM) or dynamic CT myelography, it has become possible to identify different types of spinal CSF leaks.4 Type 1 CSF leaks are those caused by spontaneous dural tears that occur on the ventral (type 1a) or posterolateral (type 1b) aspect of the thecal sac.4 Type 2 CSF leaks are associated with simple (type 2a) or complex (type 2b [dural ectasia]) meningeal diverticula. Type 3 CSF leaks are CSF-venous fistulas. Type 4 CSF leaks are of indeterminate origin.
Performing myelography with the patient in the lateral decubitus position has allowed precise characterization of lateral dural tears, and we now report the different variants of lateral CSF leaks that we have been able to identify since performing DSM with the patient in the lateral decubitus position.
MATERIALS AND METHODS
This retrospective cohort study was approved by our Medical Center’s institutional review board.
Since January 2001, all patients with SIH evaluated by us in person at Cedars-Sinai Medical Center in Los Angeles, California, have been enrolled prospectively in a registry. Patients evaluated remotely with the use of telehealth were not included. Using this registry, we reviewed the medical records, radiographic studies, and intraoperative findings of a consecutive series of patients with SIH and lateral spontaneous spinal CSF leaks who underwent DSM in the lateral decubitus position and underwent surgery to repair the CSF leak during the 5-year period between July 2018 and June 2023. The diagnosis of SIH was based on the criteria of the International Classification of Headache Disorders, third edition, with minor modifications.3,5 These criteria require objective evidence of SIH, consisting of brain MR imaging showing the stigmata of SIH (ie, pachymeningeal enhancement, brain sagging, or subdural fluid collections), spinal imaging showing a CSF leak (ie, the presence of extradural CSF or a CSF-venous fistula), or low CSF opening pressure (ie, <6.0-mL CSF). The modification consists of also including patients who do not have headaches but whose symptoms are best explained by SIH.
Our imaging protocol consisted of brain MR imaging and heavily T2-weighted MR myelography.6 DSM was used to accurately localize the exact site of the CSF leak if heavily T2-weighted MR myelography was inconclusive. In all patients, the DSM technique as described by Hoxworth et al7 was used with some minor modifications.8 Briefly, DSM was performed with the patient under general endotracheal anesthesia with deep paralysis and suspended respiration for maximal detail and temporal resolution. Patients were positioned in the lateral decubitus position in a biplane angiography suite, with tilt table capability. Pillows or foam padding was placed to optimize cervicothoracic alignment. Under fluoroscopic guidance, a 22-ga needle was placed midline usually at the L2–3 level, being careful to avoid tenting and subdural injection. Then, the accurate needle position was confirmed with an injection of 0.5 mL of contrast (Omnipaque, 240 mg/mL or 300 mg/mL; GE Healthcare). Patients were then further positioned on the basis of the area of interest, with table tilting to achieve contrast flow to the cervicothoracic spine. Finally, 12 mL of contrast was injected manually, 1 mL per second with suspended respiration for 60–75 seconds, while acquiring biplane subtraction images at 1–2 frames per second. Post-DSM CT was performed within 90 minutes of intrathecal contrast injection. We used multidetector CT units capable of helical scanning with a pitch of 0.51, kV(peak) of 120, milliampere-second, 200–440, depending on the patient’s size. Imaging output consisted of axial 0.625-mm-thick slices with the same intervals, reconstructed to 2.5-mm-thick axial, sagittal, and coronal reformatted images.
Statistical Analysis
The study presents continuous variables with means and SDs, and categoric variables, as absolute numbers and percentages. We compared demographic characteristics by type of leak using the Mann-Whitney U test for continuous variables. χ2 and Fisher exact tests were used for comparisons involving categoric variables. Given the limited sample size, we opted for nonparametric tests. We acknowledge that while opting for nonparametric tests to address distributional concerns in small sample sizes, there remains inherent limitations in the statistical power of these tests to detect a true association. All statistical analyses were performed using SAS, Version 9.4 (SAS Institute).
RESULTS
Study Population
During the study period, 65 patients underwent surgery for a spontaneous lateral spinal CSF leak. Twelve patients were excluded from the analysis because they did not undergo a preoperative DSM in the lateral decubitus position: Five patients had undergone DSM in the prone position, showing the level of the CSF leak, 4 patients had undergone surgery elsewhere but had a persistent CSF leak and the level of the CSF leak had been adequately identified, 2 patients underwent surgery on the basis of heavily T2-weighted MR myelography showing the level of the CSF leak, and 1 patient refused DSM, but conventional CT myelography had identified the approximate level of the CSF leak.
The mean age of the 53 study patients (37 women and 16 men) at the onset of SIH symptoms was 35.5 years (Table 1). Five patients had 2 lateral CSF leaks, and 48 patients had a single lateral CSF leak for a total of 58 lateral CSF leaks.
Cohort demographics and clinical characteristics (N = 53)
Classification of Lateral CSF Leak Variants
Three different variants of lateral CSF leak could be identified (Fig 1). Of the 53 patients, 49 patients (92.5%) had a lateral dural tear associated with the nerve root sleeve. The dural tear was at the axilla (Fig 2 and Online Supplemental Data), caudal to the nerve root sleeve in 36 patients (67.9%) or at the shoulder (Fig 3 and Online Supplemental Data), cranial to the nerve root sleeve in 13 patients (24.5%). Four patients (7.6%) had a lateral dural tear at the level of the pedicle that was not associated with the nerve root sleeve (Fig 4). Findings on DSM were concordant with intraoperative findings in all patients.

Illustration depicting the 3 variants of spontaneous lateral spinal CSF leaks. We found spontaneous lateral CSF leaks to be associated with the axilla of the nerve root sleeve in about two-thirds of patients and associated with the shoulder of the nerve root sleeve in about one-fourth of patients. Uncommonly (7.5%), the lateral dural tear was found at the level of the pedicle and was not associated with the nerve root sleeve.

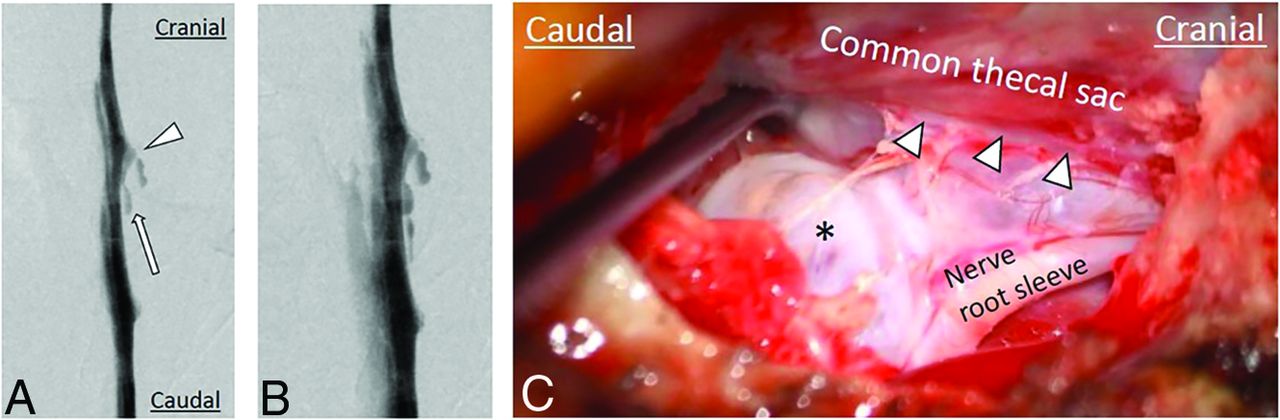
Imaging and intraoperative findings of spontaneous lateral spinal CSF leaks arising from the axilla of the nerve root sleeve. DSMs (A and B) show a lateral CSF leak (arrow) arising caudal to the nerve root sleeve (arrowhead). C, Intraoperative photograph shows a lateral dural tear (arrowheads) caudal to the take-off of the nerve root sleeve with arachnoid (asterisk) protruding through the dural tear.

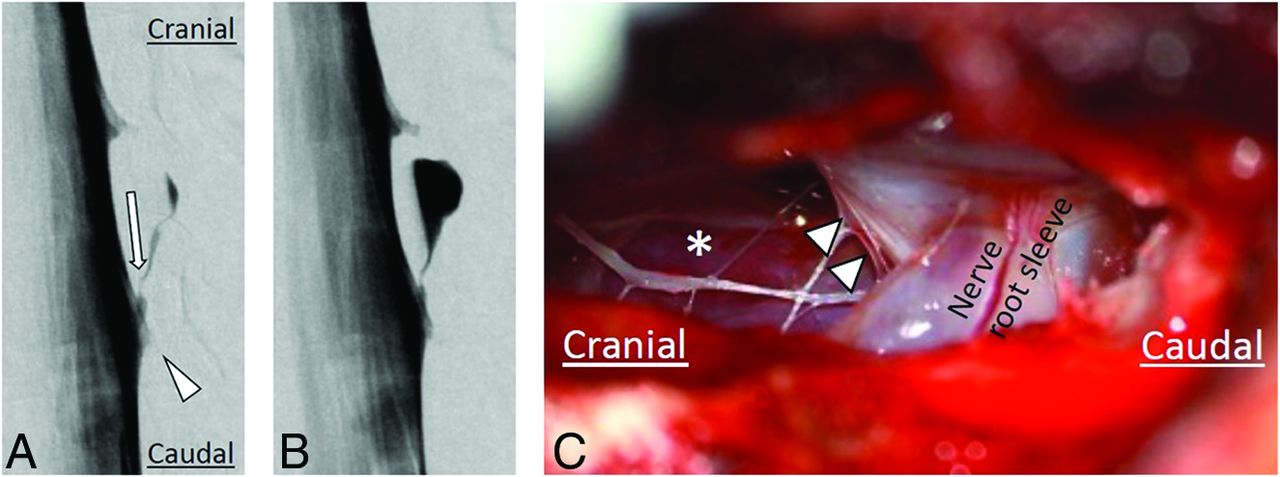
Imaging and intraoperative findings of spontaneous lateral spinal CSF leaks arising from the shoulder of the nerve root sleeve. DSMs (A and B) show a lateral CSF leak (arrow) arising cranial to the nerve root sleeve (arrowhead). C, Intraoperative photograph shows a lateral dural tear (arrowheads) cranial to the take-off of the nerve root sleeve after the arachnoid membrane has been resected, leaving a clear view of the extended extradural space (asterisk).

Imaging and intraoperative findings of spontaneous lateral spinal CSF leaks arising at the level of the pedicle. DSM (A) shows a small, defined lateral extradural CSF collection (arrow) at the level of the pedicle, not associated with the nerve root sleeve. Axial T2-weighted MRI (B) shows a corresponding small extradural CSF collection (arrow) that was not visible on post-DSM CT (C). The intrathecal contrast on the post-DSM CT is faint, possibly limiting the sensitivity of leak detection. Intraoperative photograph (D) shows a lateral dural tear (arrowheads) with arachnoid billowing out (asterisk) through the dural defect. DSMs (E–G) show a lateral dural tear (arrow) at the level of the pedicle, not associated with the nerve root sleeve, resulting in an extensive CSF leak, with CSF spreading in both cranial and caudal directions (arrowheads). Intraoperative photographs (H and I) show a linear dural tear (arrowheads) without arachnoid protruding through the dural tear. The underlying spinal cord is visible after spreading the dural tear (H).
Patients with a lateral dural tear at the shoulder of the nerve root were younger (mean age, 28.9 years) than those with a lateral dural tear at the axilla of the nerve root (mean age, 38.1 years) or at the level of the pedicle (mean age, 32.8 years) (P = .029), but there were no differences in sex or symptom duration (Table 2).
Characteristics per leak type
An extradural CSF collection was present on heavily T2-weighted MR myelography as well as post-DSM CT in all 49 patients with a lateral CSF leak associated with the nerve root sleeve (Online Supplemental Data). The extradural CSF collection was extensive, extending over 3–21 spinal levels in 45 patients but confined to a single spinal level in 4 patients. In 2 of these 4 patients with a confined extradural CSF collection, prior imaging had shown an extensive extradural CSF collection indicating considerable-but-incomplete improvement of the CSF leak. Among the 4 patients with the pedicular variant of a lateral CSF leak, an extensive extradural CSF collection was present in 1 patient, a small confined extradural CSF collection could be identified on heavily T2-weighted MR myelography but not on post-DSM CT in 1 patient, while neither heavily T2-weighted MR myelography nor post-DSM CT could demonstrate an extradural CSF collection in 2 patients (Fig 4 and Online Supplemental Data). Dynamic CT myelography with the patient in the lateral decubitus position was not performed in any of these patients.
The extradural CSF collection was symmetric and nonlateralizing in 14 patients (27.5%), bilateral but asymmetric lateralizing to the side of the lateral CSF leak in 24 patients (47.1%), and unilateral in 13 patients (25.5%).
Five patients (9.4%) had 2 lateral CSF leaks, and 48 patients (90.6%) had a single lateral CSF leak, for a total of 58 lateral CSF leaks. Multiple lateral CSF leaks were identified in 3 (23.1%) of the 13 patients with a CSF leak at the shoulder of the nerve root sleeve, in 2 (5.6%) of the 36 patients with a CSF leak at the axilla of the nerve root sleeve, and in none of the patients with a pedicular type lateral CSF leak (P = .128). The variant of a lateral CSF leak was the same in each of these 5 patients, ie, 3 patients had 2 lateral CSF leaks at the shoulder of the nerve root sleeve and 2 patients had 2 lateral CSF leaks at the axilla of the nerve root sleeve.
Most lateral CSF leaks (58.6%) in this study were found in the lower thoracic spine (Table 1). We found no evidence of a calcified lesion associated with a lateral dural tear in any patient.
We found the coexistence of a spontaneous lateral CSF leak and a CSF-venous fistula in one (7.7%) of the 13 patients with a lateral CSF leak at the shoulder of the nerve root sleeve and in 2 (5.6%) of the 36 patients with a lateral CSF leak at the axilla of the nerve root sleeve (Online Supplemental Data).
Surgical Repair
At surgery, a lateral dural tear could be identified in all patients, and the dural tear was repaired with sutures (7-0 Gore-Tex; W. L. Gore & Associates) and/or a muscle graft in 3 (5.2%) and with titanium aneurysm clips (Yasargil; B. Braun) in 55 (94.8%) of the 58 lateral CSF leaks.
Postoperative Imaging
Postoperative imaging with heavily T2-weighted MR myelography or high-resolution spine MRI was performed in all patients and showed complete resolution of the extradural CSF collection in 55 (98.2%) of the 56 CSF leaks that had been associated with an extradural CSF collection (Online Supplemental Data). Of the 2 patients with the pedicular variant of a lateral CSF leak that was not associated with an extradural CSF collection, SIH symptoms and brain MRI stigmata of SIH resolved postoperatively in one patient, and postoperative DSM was performed in the other patient, showing resolution of the lateral CSF leak (Online Supplemental Data).
DISCUSSION
In this study, we identified 3 different variants of spontaneous lateral spinal CSF leaks. Most CSF leaks are associated with the nerve root sleeve, and these can be divided into 2 variants, those at the axilla, caudal to, or at the shoulder, cranial to the nerve root sleeve. No significant differences were found in sex distribution or the duration of symptoms between these 2 variants, but the same variant being observed among all patients with multiple lateral CSF leaks and the significant age difference suggest that these may be 2 distinct types of lateral CSF leaks.
The variant we observed at the level of the pedicle that was unrelated to the nerve root sleeve has, to our knowledge, not been described previously. We have only been aware of this variant since 2022, and it is possible that previously, we have failed to identify this particular variant of lateral CSF leak on DSM. Of the 4 patients we have encountered so far, an extensive extradural CSF collection was present in only 1 patient. In the other 3 patients, the appearance of the lateral leak was subtle but clearly visible on DSM, while a small amount of extradural CSF was visible on heavily T2-weighted MR myelography in only 1 of these 3 patients, and no extradural CSF was visible on post-DSM CT in any of these 3 patients. Thus, in addition to the CSF-venous fistula,9⇓-11 the pedicular variant of a lateral CSF leak may be the second type of CSF leak that may require specialized imaging such as DSM or dynamic CT myelography. DSM has excellent spatial resolution of only 300 μm (0.3 mm). None of our patients were investigated with primary lateral dynamic CT myelography.
We found the extradural CSF collection associated with the lateral dural tears to be lateralizing in about three-fourths of patients, facilitating the choice of positioning of the patient for DSM (left or right side down). We did not observe a clear sidedness to the location of the lateral dural tear that could help decide positioning of those patients with symmetric nonlateralizing extradural CSF collections.
Identifying the different variants of lateral CSF leaks may have some practical implications for both directed percutaneous procedures, ie, blood or fibrin glue patching, as well as for a more tailored surgical approach to the lateral CSF leak, especially with the more recently developed minimally invasive tubular approaches.12,13 Targeted percutaneous fibrin glue and/or blood patch procedures are based on traditional nerve block and epidural injection techniques, which were developed with the goals of minimal risk of nerve injury, intrathecal puncture, or vascular injections. A traditional subpedicular “safe triangle” approach targets the anterior superior aspect of the neuroforamen.14 The safety of the safe triangle approach has been questioned recently due to the location of the radicular or radiculomedullary artery in the anterior-superior quadrant of the neuroforamen.
An alternative approach targets the Kambin triangle, a region described in the context of accessing intervertebral discs for surgery.15,16 The Kambin triangle describes an area overlying the posterolateral disc that is bounded by the inferior vertebral body at its base, the exiting spinal nerve root at the hypotenuse, and the traversing nerve root or dura at the vertical leg.15,16 The relative location of lateral tears has significant implications on the optimal choice that combines efficacy with minimal neurovascular injury risk. The safe triangle approach may be more effective with the shoulder variant of the lateral tear and not suitable for the axillary or pedicular variants.
In this study, we were able to confirm the presence of a lateral dural tear in all patients in accordance with the findings on DSM. In the past, we have classified many of these patients as having leaking spinal meningeal diverticula.4 However, the lateral dural tear is the primary pathology with the arachnoid billowing out through the dural tear, giving the appearance of a leaking meningeal diverticulum, while the actual site of CSF leakage often occurs around the arachnoid diverticulum at the edges of the lateral dural tear.
After achieving good success with identifying CSF-venous fistulas with DSM performed with the patient in the lateral decubitus position since April 2018,17 we have been performing DSM in the lateral decubitus position for suspected lateral CSF leaks since July 2018. Other investigators have also reported their positive experience with myelographic techniques in the lateral decubitus position for the identification of lateral CSF leaks.18⇓⇓⇓⇓⇓-24 Prior studies have generally not mentioned the exact anatomic site of the lateral CSF leak except for 1 study showing 4 of 4 lateral CSF leaks occurring at the level of the axilla of the nerve root sleeve19 and other reports noting that lateral CSF leaks typically occur at the shoulder25 or axilla26 of the nerve root sleeve.
CONCLUSIONS
Using DSM in the lateral decubitus position, we identified 3 variants of lateral dural tears among patients with SIH. Most lateral dural tears are associated with extensive extradural CSF collections and arise from either the axilla or the shoulder of the nerve root sleeve. Lateral dural tears located at the level of the pedicle that are not associated with the nerve root sleeve are uncommon and may require specialized imaging for their detection.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received December 12, 2023.
- Accepted after revision February 15, 2024.
- © 2024 by American Journal of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
{kind=link}