
SUMMARY:
The simultaneous presentation of intracranial steno-occlusive disease, Moyamoya disease, or Moyamoya-like vasculopathy and dural arteriovenous fistulas (DAVFs) has been documented in very few case reports worldwide. We aimed to better characterize this association by reviewing the clinical and radiologic findings of 4 patients with concurrent intracranial steno-occlusive disease or Moyamoya-like vasculopathy and DAVFs evaluated in our institution. All 4 patients were of Asian descent. One patient presented with ischemic stroke secondary to intracranial stenosis, 2 presented with symptoms related to the DAVF, and the diagnosis was incidental in the fourth patient. Three patients underwent embolization of the DAVF, which was followed by surgical ligation in 2. One patient underwent extracranial-intracranial bypass for Moyamoya-like intracranial steno-occlusive disease. One patient is being managed conservatively with close follow-up. Our case series details findings in 4 patients with associated intracranial steno-occlusive disease and DAVFs. Further studies and reporting of similar cases are necessary to establish whether this is pure coincidence or if there is indeed a relationship between these 2 conditions, especially in certain ethnic groups.
ABBREVIATIONS:
- DAVF
- dural arteriovenous fistula
- MMD
- Moyamoya disease
Moyamoya disease (MMD), Moyamoya-like vasculopathy, and intracranial steno-occlusive disease are cerebrovascular conditions with a higher incidence in East Asian countries than in the Western Hemisphere.1 Dural arteriovenous fistulas (DAVFs) are relatively uncommon cerebrovascular entities characterized by abnormal shunting between the meningeal arteries and the dural venous sinuses or subarachnoid veins,2 accounting for 10%–15% of intracranial vascular malformations,3 with an incidence as high as 0.29 per 100,000 person-years in Japan.4 There have been very few case reports worldwide documenting the co-occurrence of these 2 disease entities before surgical intervention or head trauma. Here, we describe an institutional series of 4 patients presenting with concurrent Moyamoya-like vascular changes or intracranial steno-occlusive disease and DAVFs.
CASE SERIES
We identified all patients with intracranial steno-occlusive disease, Moyamoya, Moyamoya-like vasculopathy, and DAVFs from a prospectively maintained database of cases evaluated and/or treated by the senior author (G.L.) at our institution between January 2008 and 2023. The diagnosis of idiopathic Moyamoya or Moyamoya-like vasculopathy was made on the basis of the presence of both stenosis or occlusion of the terminal ICA or the proximal middle and/or anterior cerebral artery and an abnormal network of blood vessels on cerebral angiography, according to the 2021 diagnostic criteria for MMD published by the Ministry of Health, Labor and Welfare in Japan.5 More recently, patients underwent high-resolution MR imaging with vessel wall enhancement to distinguish eccentric (more consistent with intracranial atherosclerosis) from concentric (more consistent with idiopathic vasculopathy) enhancing patterns.6,7 The Cognard system was used to classify the type of DAVF, because it is useful for predicting the associated risk and guiding management decisions.8
This retrospective study was reviewed and approved by our institutional review board (19–001663), and all protocols were followed in accordance with institutional review board guidelines. A common denominator of these patients was their Asian ethnicity. Demographics, clinical presentation, and treatment are summarized in the Online Supplemental Data. Angiographic findings are presented in Figs 1–4. MR vessel wall imaging was available for cases 2 and 4, which presented more recently after vessel wall imaging was incorporated into practice at our institution. For these patients, vessel wall imaging demonstrated circumferential vessel wall enhancement involving the distal left ICA in case 2 and lack of any vessel wall enhancement whatsoever in case 4, suggesting a steno-occlusive picture outside intracranial atherosclerosis. For cases 1 and 3, we elected to treat the DAVFs because they were symptomatic, while in case 2, we attempted treatment of the DAVF because of the retrograde cortical venous drainage/venous hypertension and its potential role in aggravating perfusion issues related to the steno-occlusive disease. For case 4, we elected for observation of the DAVF because of its asymptomatic status/incidental finding and potential risks associated with embolization (ie, compromise of retinal blood flow supply) or surgical therapy (brain manipulation in the setting of steno-occlusive disease and marginal perfusion). The steno-occlusive disease in each patient was medically managed with aspirin monotherapy, while patient 2 underwent surgical revascularization for recurrent left-hemispheric infarcts.

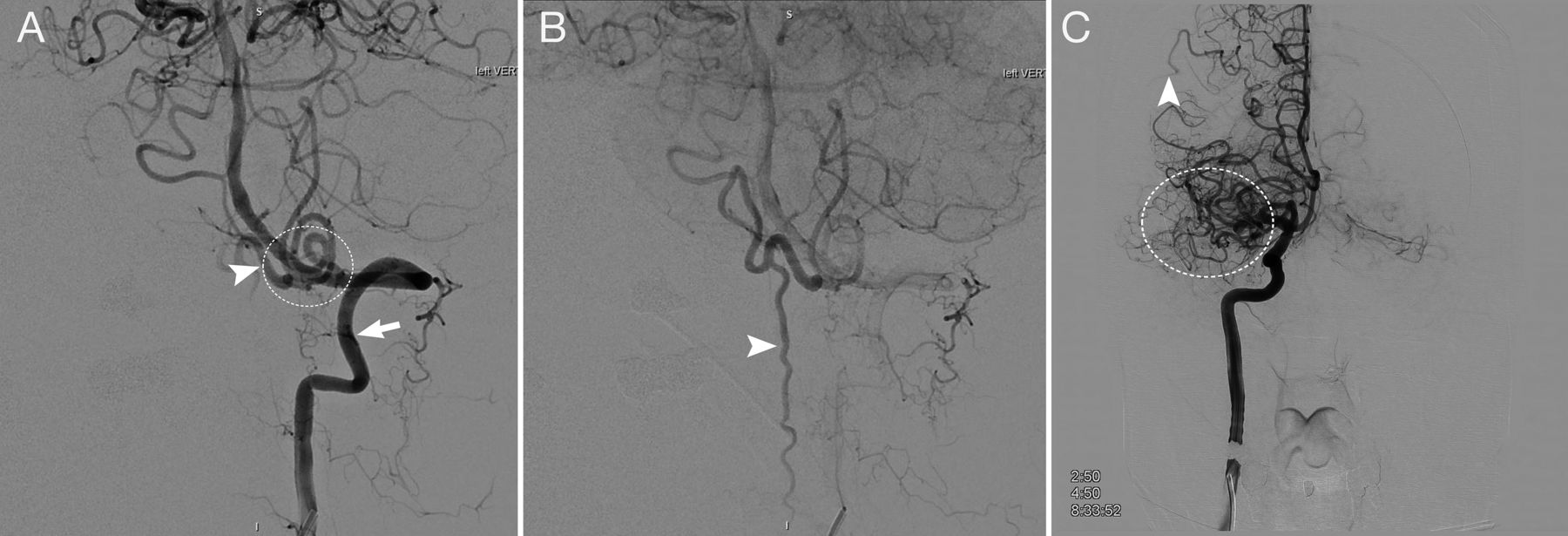
Case 1. A 57-year-old Asian man who presented with several weeks of progressive myelopathy. A, Conventional angiography shows a craniocervical junction AVF (white circle) with a large arterialized draining vein (arrowhead) arising from the dura adjacent to the point where the vertebral artery pierces the dura, supplied by branches of the left vertebral artery (arrow). B, The same injection demonstrates the venous drainage of the fistula down the anterior and posterior spinal veins, which are filled early (arrowhead). C, A right ICA injection, anterior-posterior view shows incidental occlusion of the M1 segment with Moyamoya-like collaterals (white circle) reconstituting the distal MCA territory in addition to leptomeningeal collaterals (arrowhead) from the distal anterior cerebral artery. He underwent surgical ligation of the fistula after failed embolization. The asymptomatic MCA occlusion was treated medically.

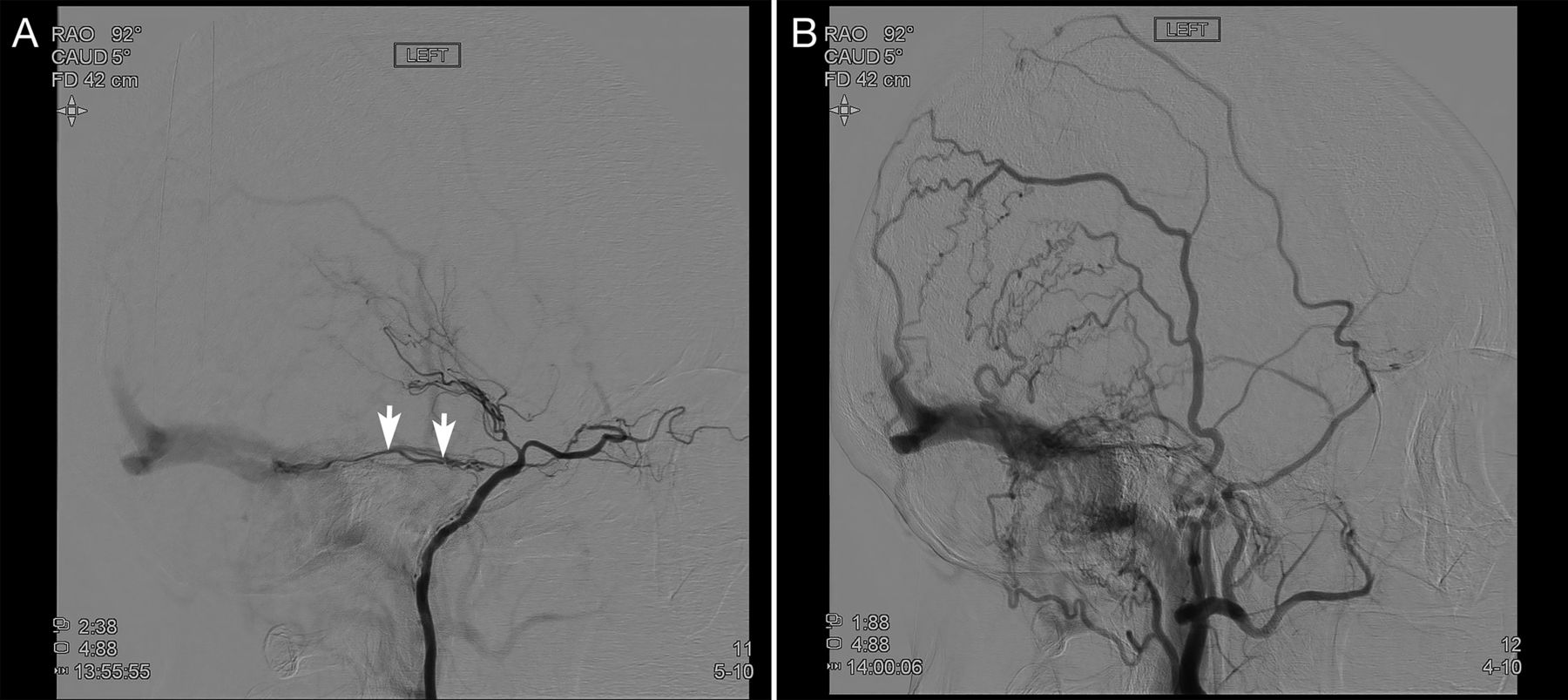
Case 2. A 63-year-old Asian man who presented with multiple left-hemisphere infarcts during 1 year. A, A left common carotid artery injection shows a left sphenoparietal DAVF (circle) supplied by the left middle meningeal artery with exclusive retrograde cortical venous drainage (arrowheads). B, There is delayed filling of the left ICA (arrow), which is occluded distal to the origin of the ophthalmic artery (arrowheads). C, Selective right ICA injection, lateral view, shows severe stenosis of the right supraclinoid ICA (arrows). The patient underwent partial embolization of the DAVF followed by surgical ligation and left superficial temporal artery–to-MCA bypass.

Case 3, A 74-year-old Asian woman who presented with episodic vision loss, papilledema, and cognitive decline. A, Conventional angiography, selective left ICA injection, shows an incidental left supraclinoid ICA occlusion as well as a left transverse-sigmoid junction DAVF with arterial feeders from the left meningohypophyseal artery (arrows). B, External carotid artery injection, lateral view, shows a high-flow transverse-sigmoid sinus DAVF. The DAVF was occluded via a transvenous approach with resolution of symptoms at follow up. Low-dose aspirin was prescribed for the incidental carotid occlusion.

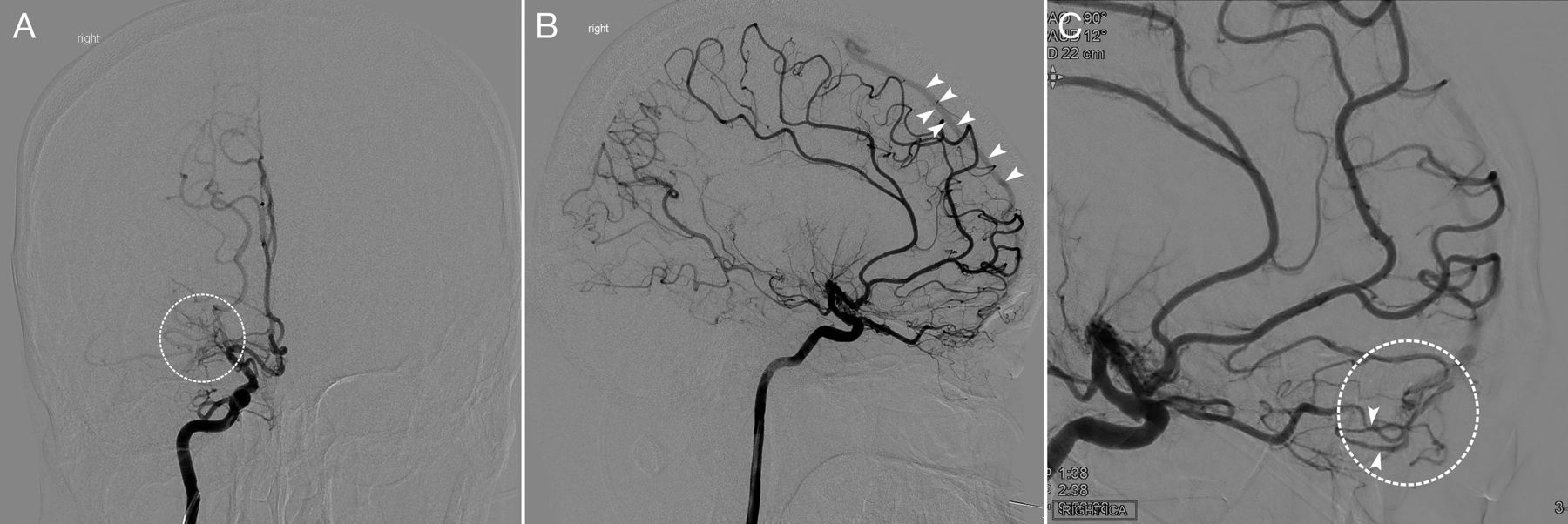
Case 4. A 42-year-old Asian man with right-sided headache. A, Selective right ICA injection, anterior-posterior view, early arterial phase, shows occlusion of the MCA with a Moyamoya network (white circle). B, Selective right ICA injection, lateral view, early arterial phase, shows a lack of opacification in the MCA territory and early filling of the superior sagittal sinus (arrowheads). C, Right ICA selective injection, magnified oblique view, shows enlarged and tortuous distal ophthalmic artery branches (arrowheads) feeding a dural/pial AVF (white circle), with early opacification of a cortical vein draining into the superior sagittal sinus.
DISCUSSION
We describe 4 patients of Asian ethnicity with concomitant idiopathic Moyamoya disease, Moyamoya-like vasculopathy, or steno-occlusive disease and intracranial DAVFs. The rare concurrent appearance of intracranial steno-occlusive disease and DAVFs as seen in our 4 cases has been previously documented in only a few single case reports and usually after surgical therapy or trauma. De novo formation of DAVFs in patients with Moyamoya-like vasculopathy has been observed in a delayed fashion following direct bypass,9,10 indirect bypass,11 and head trauma;12 however, there have been a very few cases of simultaneous presentation in the absence of prior surgery or trauma. These include a patient with unilateral MMD who presented with intraventricular hemorrhage and was found to have an ipsilateral transverse-sigmoid DAVF, which was ultimately treated with endovascular embolization,13 similar to case 3 in our series, as well as ipsilateral cavernous and tentorial DAVFs observed in patients with MMD in China14 and Spain,15 respectively.
A proposed mechanism for the formation of DAVFs in these patients is that aberrant flow dynamics in intracranial steno-occlusive disease leads to an increased demand and decreased perfusion, with the subsequent ischemia triggering an angiogenic response in the dural vasculature, resulting in arteriovenous shunting.16 Indeed, increased expression of proangiogenic factors has been reported in the dura of patients with MMD, including vascular endothelial growth factor17 and fibroblast growth factor.18 These factors are also involved in the formation of DAVFs.19
Of note, all 4 patients in our series are of East Asian ethnicity, suggesting that a genetic association may potentially exist in cases of concurrent intracranial steno-occlusive disease and DAVF. None of the previous case reports we came across specified the patients’ ethnicity, so we could not confirm such an association on the basis of prior literature. Nevertheless, variants of the HLA genes and the RNF213 susceptibility gene have been found to be associated with East Asian patients with MMD.20,21 Unfortunately, the patients included in our study did not undergo genetic testing to evaluate these pathogenic variants; however, this association would be an interesting area of future study. Overall, intracranial stenosis is more prevalent in Asians,22 often with a younger mean age of onset and independent of vascular risk factors compared with Caucasians.23
In our small institutional case series, we describe the simultaneous presentation of the two entities of Moyamoya pattern/steno-occlusive intracranial disease and DAVF in 4 patients of East Asian descent. While our series does not establish causality, future reporting and study of similar cases may further determine whether a potential relationship exists between ethnicity and the concurrence of these cerebrovascular phenomena. As more patients like these are identified, the pathophysiology of these two conditions can be more clearly elucidated and the presence of an underlying genetic association can be investigated.
Acknowledgments
We acknowledge Peggy Chihak and Arielle Davis for their help in formatting the figures and manuscript.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received November 15, 2023.
- Accepted after revision January 15, 2024.
- © 2024 by American Journal of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.