
Abstract
BACKGROUND: The optimal imaging method for detecting distal medium vessel occlusions (DMVOs) remains undefined.
PURPOSE: The objective of this study is to compare the diagnostic performance of CTA with CTP in detecting DMVOs.
DATA SOURCES: We searched PubMed, EMBASE, Web of Science Core Collection, and Cochrane Central Register of Controlled Trials up to March 31, 2023 (PROSPERO: CRD42022344006).
STUDY SELECTION: A total of 12 studies reporting accuracy values of CTA and/or CTP were included, comprising 2607 patients with 479 cases (18.3%) of DMVOs.
DATA ANALYSIS: Pooled sensitivity and specificity of both imaging methods were compared using a random-effects model. Subgroup analyses were performed based on the technique used in CTA (multi or single-phase) and the subtype of DMVOs (M2-only vs. M2 and other DMVOs). We applied Quality Assessment of Diagnostic Accuracy (QUADAS-2) tool and Grading of Recommendations, Assessment, Development and Evaluation (GRADE) quality assessment criteria.
DATA SYNTHESIS: CTA demonstrated significantly lower sensitivity compared to CTP in detecting DMVOs [0.74, 95%CI (0.63–0.82) vs. 0.89, 95% CI (0.82–0.93), P < 0.01]. When subgrouped into single-phase and multi-phase CTA, multi-phase CTA exhibited higher sensitivity for DMVO detection than single-phase CTA [0.91, 95%CI (0.85–0.94) vs. 0.64, 95%CI (0.56–0.71), P < .01], while reaching similar levels to CTP. The sensitivity of single-phase CTA substantially decreased when extending from M2 to other non-M2 DMVOs [0.74, 95%CI (0.63–0.83) vs. 0.61, 0.95%CI (0.53–0.68), P = .02].
LIMITATIONS: We identified an overall high risk of bias and low quality of evidence, attributable to the design and reference standards of most studies.
CONCLUSIONS: Our findings highlight a significantly lower sensitivity of single-phase CTA compared to multi-phase CTA and CTP in diagnosing DMVOs.
ABBREVIATIONS:
- DMVO
- distal medium vessel occlusion
- EVT
- endovascular treatment
- GRADE
- Grading of Recommendations, Assessment, Development and Evaluation
- mpCTA
- multiphase CT angiography
- QUADAS-2
- Quality Assessment of Diagnostic Accuracy
- SCA
- superior cerebellar artery
- spCTA
- single-phase CTA
- Tmax
- time-to-maximum
Distal medium vessel occlusions (DMVOs),1 also known as medium vessel occlusions,2 refer to the occlusion of arteries with diameters ranging from 0.75 to 2.0 mm. This term generally encompasses segments M2 to M4 of the MCA, A2 to A5 of the anterior cerebral artery, P2 to P5 of the posterior cerebral artery, the PICA, AICA, and superior cerebellar artery (SCA).1
Acute ischemic stroke imaging workflows have been designed to efficiently detect large-vessel occlusions suitable for endovascular treatment (EVT), which is increasingly being offered in DMVOs.3 Noncontrast CT and CTA, without advanced imaging techniques, have been used to identify candidates for EVT, even in the late window.4,5 In contrast, CTP may be time-consuming and is not widely used, particularly in the early window and in primary stroke centers.6 However, incorporating CTP into imaging protocols could improve the detection and, therefore, the treatment of DMVOs, for which the optimal imaging approach is yet to be determined.
The aim of this study was to conduct a systematic review and meta-analysis of diagnostic test accuracy for CTA and CTP in the detection of DMVOs.
MATERIALS AND METHODS
This study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.7 We registered this study in PROSPERO (https://www.crd.york.ac.uk/PROSPERO/) (CRD42022344006) and published a comprehensive protocol detailing the methods.8 Because this a secondary study, no ethics approval was requested. We did not receive any funding or financial support. Aggregate data generated by this study will be available on reasonable request.
Search Strategy, Selection, and Data Collection
We conducted a systematic search of the PubMed (including MEDLINE), EMBASE, Web of Science Core Collection, and Cochrane Central Register of Controlled Trials to identify relevant primary studies reporting on the diagnostic accuracy of CTA and/or CTP (interpreted in conjunction with CTA or separately) for the detection of DMVOs. The search was performed from the inception of the databases until March 31, 2023. We used various combinations of the following terms: “acute ischemic stroke,” “distal vessel occlusion,” “medium vessel occlusion,” “distal medium vessel occlusion,” “M2,” “M3,” “M4,” “A2,” “A3,” “A4,” “A5,” “P2,” “P3,” “P4,” “P5,” “posterior inferior cerebellar artery,” “PICA,” “anterior inferior cerebellar artery,” “AICA,” “superior cerebellar artery” or “SCA” artery occlusions, “CT angiography,” “CT perfusion,” “perfusion imaging” and database-specific subject headings (eg, Medical Subject Headings [MeSH] terms). Detailed search strategies for each database can be found in the published protocol.8 We also scanned gray literature, references of selected studies, and reviews on the subject for missing articles.
Two authors (J.A.S, and A.S.) independently reviewed articles retrieved from the systematic search performed. We collected the following variables: study design, date, authors, index and reference tests, sample size, location of DMVOs, and either individual data or summary estimates of sensitivity, specificity and, when available, the number of true-positive, true-negative, false-positive, false-negative, positive predictive values, and negative predictive values of CTA and/or CTP. Data extracted were reviewed and validated by a third reviewer (S.B.C.).
Quality of Evidence and Risk of Bias
Two investigators assessed the risk of bias for each individual study independently (J.A.S, and A.S.) via the Quality Assessment of Diagnostic Accuracy (QUADAS-2) tool.9 We used Grading of Recommendations, Assessment, Development and Evaluation (GRADE) quality assessment criteria for diagnostic accuracy studies.10,11 To assess publication bias, we performed a funnel plot and a complementary Deek test.12
Data Synthesis and Statistical Analysis
The statistical analysis was performed following the Cochrane Handbook for Systematic Reviews of Interventions.13 A bivariate model was used to combine sensitivity and specificity data and calculate 95% confidence regions around the summary operating points. The consistency and heterogeneity of the included studies were assessed using the Higgins I2 statistic (low heterogeneity, ≤25%; moderate, between 25% and 50%; and high, >75%). Data synthesis was performed using a random effects model to provide a more conservative estimate of the overall diagnostic performance.
Subgroup Analysis
We divided the studies on the basis of whether they used single-phase CTA (spCTA) or multiphase CTA (mpCTA). Additionally, we categorized the studies on the basis of the occlusion site composition of their study samples because 2 subgroups were clearly identified. The first included studies exclusively included M2 occlusions in their DMVO samples, while the second subgroup included studies with more heterogeneous samples, encompassing various types of DMVOs.
RESULTS
We identified 5378 unique studies. Twelve studies met the inclusion criteria for our analysis. The PRISMA flow chart is presented in Fig 1. The selected studies, summarized in the Online Supplemental Data, involved a total of 2607 patients, among whom 479 (18.3%) were identified as having DMVOs. The distribution of DMVOs is presented in the Table, with a predominance of M2 occlusions observed (312 patients, 65.1%). Eight studies14⇓⇓⇓⇓⇓⇓-21 included patients with acute ischemic stroke within 24 hours of symptom onset, two22,23within 12 hours, and two24,25 within 9 hours. The evaluation of the images involved >79 different readers with varying levels of experience. All studies14⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓-25 provided information on CTA. Two studies investigated the combination of CTP and spCTA versus spCTA only;15,19,24 1 study compared CTP with spCTA and separately tested the diagnostic accuracy of CTP alone.20 Eleven studies14⇓⇓⇓⇓⇓⇓⇓-22,24,25 provided data on spCTA, and 4 studies14,21⇓-23 provided data on mpCTA. Between-study heterogeneity was observed in the sensitivity of the CTA studies (I2 = 70%, P < .01), while the heterogeneity was low in the CTP studies (I2 = 0%, P = .81).

PRISMA flow chart.
| Characteristics | n = 2607 |
|---|---|
| DMVOs (No.) (%) | 479 (18.3) |
| Type of DMVO | |
| M2 (No.) (%) | 312 (65.1) |
| M3/M4 (No.) (%) | 52 (10.9) |
| A2/A3/A4 (No.) (%) | 23 (4.8) |
| P2/P3/P4 (No.) (%) | 42 (8.8) |
| PICA (No.) (%) | 2 (0.42) |
| SCA (No.) (%) | 1 (0.21) |
| Unspecified without M2a | 24 (5.0) |
| Unspecified with M2b | 23 (4.8) |
Distribution of the DMVOs assessed in the selected studies
QUADAS-2 and GRADE revealed an overall high risk of bias and a low quality of evidence (Online Supplemental Data). The funnel plot (Online Supplemental Data), along with Deek test, did not reveal any publication bias for the studies reporting on CTA (Deek: t = −0.09, df =13, P value = .93). In the case of CTP studies, the Deek test could not be performed (<10 studies).
In all studies that used CTP, including one exclusively with an M2 occlusion sample,15 diagnostic accuracy in the detection of DMVOs was significantly higher compared with spCTA using either CTP alone through territorial time-to-maximum (Tmax) evaluation19 or CTP in a combination with spCTA (Online Supplemental Data).15,24 The specificity remained similar. Three studies directly compared the accuracy of DMVO detection in spCTA versus mpCTA. Of these, two14,22 reported improved accuracy as well as shorter detection times when mpCTA was used. One that evaluated only M2 occlusions21 reported no differences (Online Supplemental Data).
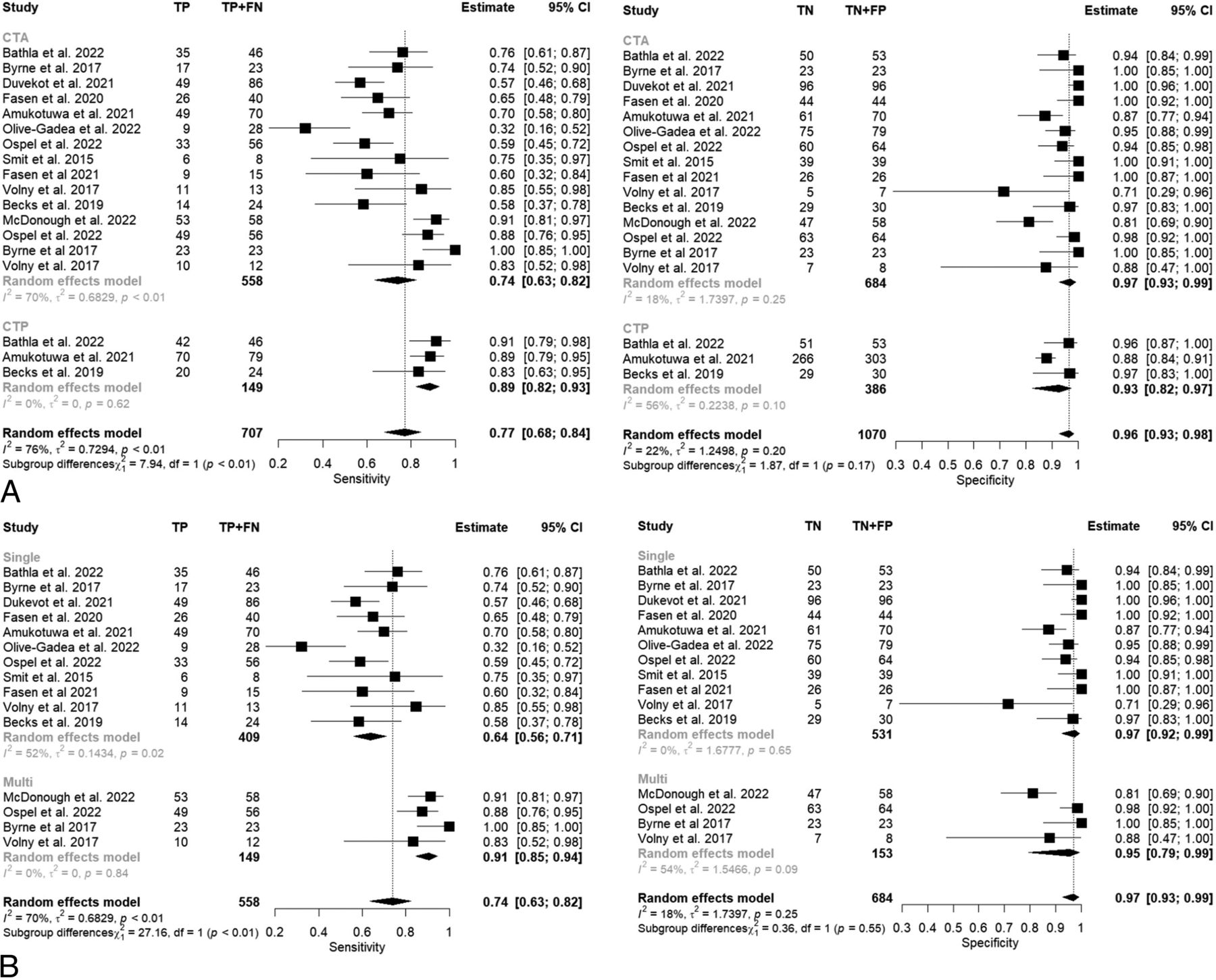
In the meta-analysis, we observed that CTA had significantly lower sensitivity than CTP for the detection of DMVO (0.74; 95% CI, 0.63–0.82 versus 0.89; 95% CI, 0.82–0.93; P < .01) (Fig 2, part A). Subgroup analysis revealed that mpCTA had significantly higher sensitivity for DMVO detection compared with spCTA (0.91; 95% CI, 0.85–0.94 versus 0.64; 95% CI, 0.56–0.71; P < .01) (Fig 2, part B), while achieving levels similar to those of CTP (0.91; 95% CI, 0.85–0.94 versus 0.89; 95% CI, 0.83–0.93; P = .68) (Fig 2, parts A and B). A pooled analysis including mpCTA and CTP (Online Supplemental Data) studies showed high sensitivity (0.90; 95% CI, 0.86–0.93) compared with spCTA (0.64; 95% CI, 0.56–0.71; P < .01). The specificity analysis did not reveal any differences except when comparing the specificity of CTA + CTP versus CTP-only (territorial Tmax) 0.98; (95% CI, 0.93–0.99) versus 0.88 (95% CI, 0.84–0.91; P < .019).

Forest plot of the pooled sensitivity and specificity of CTA and CTP (A) and CTA (spCTA) and mpCTA (B) in the diagnosis of DMVOs. TP indicates true positive; FN, false negative; TN, true negative; FP, false positive.
When comparing accuracy values provided by studies that included only M2 occlusions and those that included other DMVOs as well, we observed a significant decrease in sensitivity including non-M2 DMVO occlusions through spCTA (0.74; 95% CI, 0.63–0.83 versus 0.61; 0.95% CI, 0.53–0.68; P = .04) (Fig 3 part A). This decline in sensitivity did not occur with either mpCTA or the inclusion of CTP (Fig 3, parts B and C).

Forest plot of the pooled sensitivity and specificity of CTA (spCTA) (A), mpCTA (B), and CTP (C) in studies including only M2 occlusions versus others including other DMVOs. TP indicates true positive; FN, false negative; TN, true negative; FP, false positive.
Also, the pooled sensitivity of the 3 spCTA studies15,17,21 that included only M2 occlusions was 0.74 (95% CI, 0.63–0.83). In contrast, the sensitivity of the single M2-only CTP study15 was 0.91 (95% CI, 0.79–0.98; P = .03).
DISCUSSION
Our study provides consistent evidence for a higher sensitivity in detecting DMVO with mpCTA or CTP compared with spCTA (with or without cross-reference to spCTA). This study represents the first systematic review specifically addressing the diagnosis of this subtype of acute ischemic stroke.
The pooled sensitivity of spCTA from 4 studies that included only M2 occlusions15,18,21,25 was higher than the sensitivity of spCTA retrieved from 8 studies14,16,17,19,20,22⇓-24 that included other vessels within their DMVO sample. This finding indicates the challenge of detecting occlusions beyond the M2 territory using this imaging method. Most interesting, this decrease in sensitivity from M2-only to M2 +other DMVOs studies does not appear to occur in mpCTA or CTP. However, it is important to exercise caution when interpreting these findings because there was a single M2-only study with CTP21 and only one with mpCTA.15
Even when restricting the analysis to M2-only studies, the comparison among the pooled sensitivity of 3 studies with spCTA with 1 CTP study favors the latter. This finding, while acknowledging the limitations imposed by the number of included studies in this subanalysis, highlights the potential limitations of single-phase CTA in a particular DMVO detection scenario in which there is a higher likelihood of a safe and effective thrombectomy, because it is already routinely performed.26
No differences in terms of specificity were found, except for the higher specificity of CTA + CTP compared with CTP-only. However, only 1 study19 provided data for CTP-only. Relying solely on the territorial Tmax delay parameter, which was used to infer the presence of a DMVO, may result in false-positives.
No studies compared mpCTA with CTP. A between-study comparison yielded similar accuracy values. However, it is worth noting a slight difference in the included occlusions, because 2 CTP studies19,24 included M4, P4, PICA, AICA, and SCA that were not part of the occlusion sample in the mpCTA studies.
Our findings indicate that spCTA lacks sensitivity to reliably exclude DMVOs treatable by EVT, such as M2 occlusions, and imaging protocols should include either mpCTA or CTP because they offer the highest sensitivity. CTP should be complemented with CTA to increase specificity.
Future studies investigating the diagnostic accuracy in DMVOs should be performed on unselected patients, ideally with a prospective design, and provide clear data on reference standards that should be standardized and preferably be DSA. With the aim of establishing the optimal DMVO imaging workflow, studies should also include data on stroke workflow metrics. Additionally, studies may explore information that can be extracted from imaging beyond diagnosis, such as assessing collateral status, given the growing interest in the assessment of collateral status to guide treatment.5 One study27 has already demonstrated the relevance of quantitatively measuring collaterals with CTP in DMVO.
Strength of Evidence and Limitations
The overall strength of evidence was considered low (Online Supplemental Data) because it was downgraded in the risk of bias and indirectness categories. Between-study heterogeneity was substantial in the sensitivity values provided by CTA studies. This finding is attributed to the grouping of spCTA and mpCTA studies into the same category. Splitting spCTA and mpCTA studies reduces heterogeneity as shown in Fig 2. The risk of bias was considered high in the patient-selection domain due to study design and/or the reference standard in 8 studies14⇓⇓⇓-18,21,23,25 as illustrated in the Online Supplemental Data. A notable limitation was the determination of the reference standard. Only 215,20 of the 12 studies included DSA as part of the reference standard, as in the protocol developed by Sousa et al,8 because this examination is generally reserved for cases in which EVT is expected and to diagnose secondary DMVOs (ie, migration of a previous large-vessel occlusion). These 2 studies included a total of 437 patients and compared spCTA with CTP, and their findings were congruent with the remaining studies. Because DSA is considered the most sensitive technique for DMVO detection by consensus,1 its unavailability as a reference standard in most of the studies may have overestimated the accuracy of CTA and/or CTP. In fact, hypo- and hyperperfusion in CTP may also occur in recently recanalized arteries.28 Eight of the 12 studies used as a reference standard a combination of several imaging methods that included follow-up imaging in which it is unexpected that a DMVO goes unnoticed. Moreover, from a clinical perspective, the important aspect is not the exact accuracy values of each imaging technique but rather their comparative performance and the preferred diagnostic workflow. In this regard, this study provides consistent insights.
CONCLUSIONS
Imaging workflows incorporating multiphase CTA and CTP demonstrate significantly higher sensitivity in the diagnosis of DMVOs compared with single-phase CTA, particularly, but not exclusively, in arteries beyond the M2 segment of MCA.
Footnotes
J.A. Sousa and A. Sondermann contributed equally and should be listed as co-first authors.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received August 3, 2023.
- Accepted after revision October 31, 2023.
- © 2024 by American Journal of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.