
Article Figures & Data
Figures
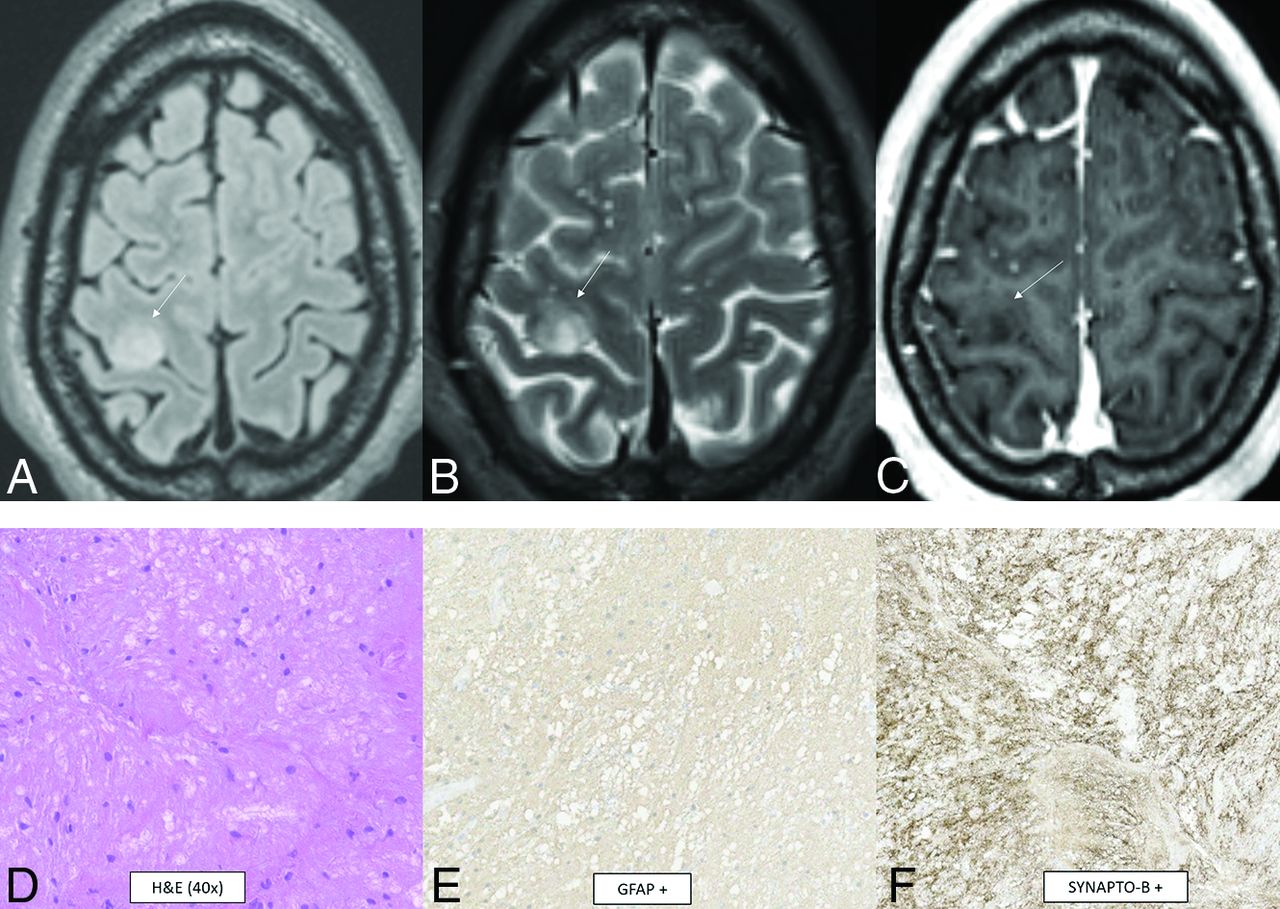
- FIG 1.
Diffuse astrocytoma, MYB- or MYBL1-altered. A cortical T2 FLAIR (A) and T2 (B) hyperintense mass is noted within the right precentral gyrus (arrows) with low T1 signal and no enhancement (C). Histopathology reveals mildly hypercellular white matter with vaguely hypocellular areas and atypical glial cells (D), which are positive for GFAP (E) and synaptophysin (F). Chromosomal microarray analysis revealed a gain of 8q13.1q21.3, disrupting MYBL1. This is a WHO grade 1 tumor.
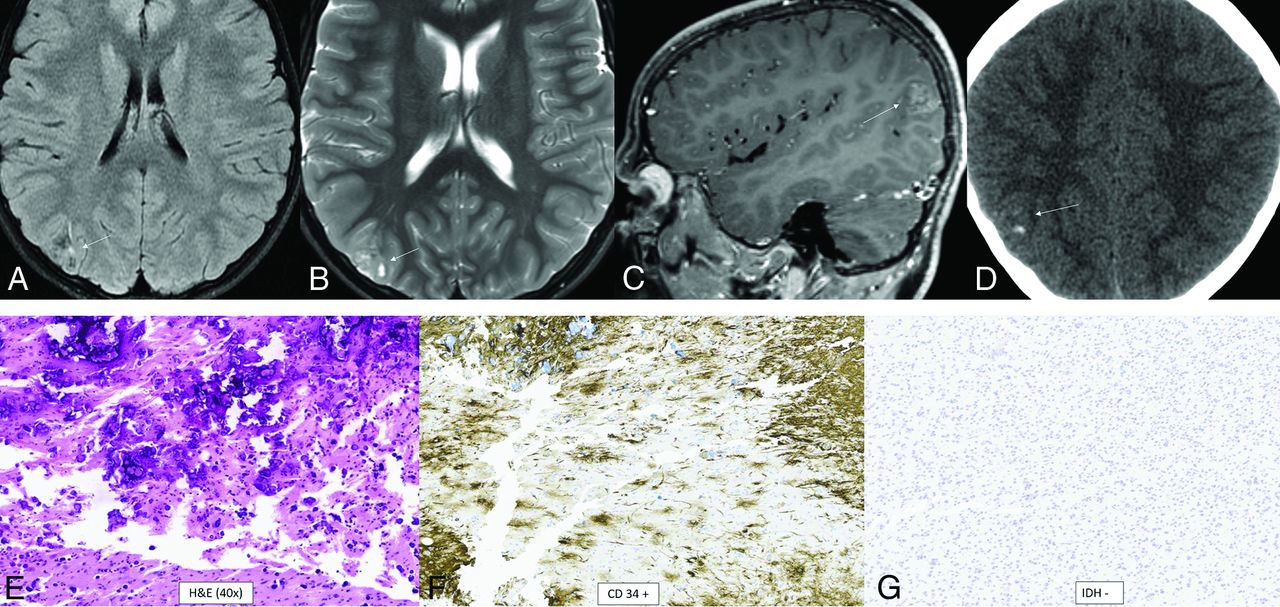
- FIG 2.
Polymorphous low-grade neuroepithelial tumor of the young. It is a cortical/subcortical mass on T2-FLAIR (A) and T2-weighted images (B) with a cystic (“bubbly”) appearance, some suppression of fluid signal on the FLAIR image, and faint heterogeneous enhancement (C) within the right inferior parietal lobule (arrows). CT shows faint specks of calcification within the lesion (D). Histology demonstrates a relatively well-demarcated low-grade neuroepithelial tumor with prominent dystrophic calcification (E). Tumor cells have oligodendroglial-like morphology and are strongly positive for CD34 (F), with low proliferative activity. Immunohistochemical stain is negative for IDH1 R132H (G) and positive for OLIG2. Chromosomal microarray identified loss of 10q21.3q26.13 disrupting CTNNA3 and FGFR2, representing a FGFR2-CTNNA3 fusion.
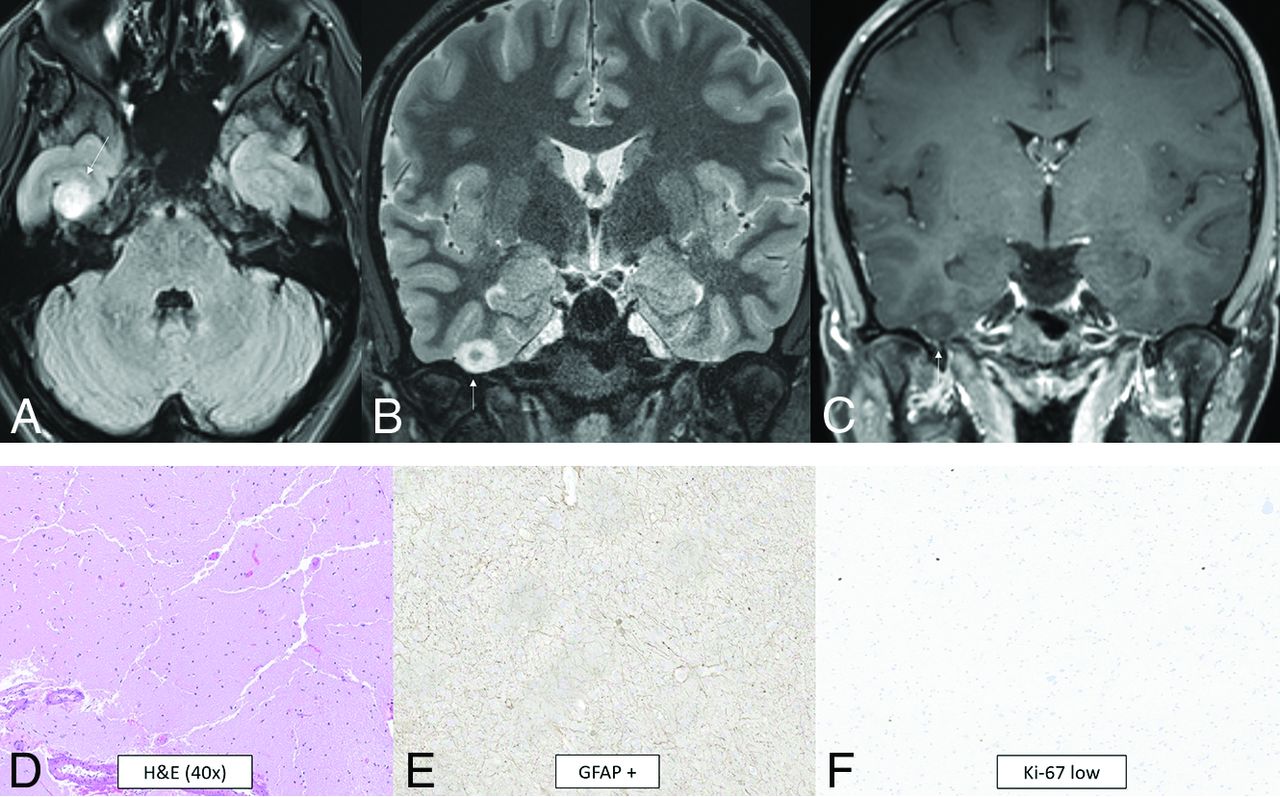
- FIG 3.
Diffuse low-grade glioma, MAPK pathway–altered. A cortical T2-FLAIR (A) and T2-hyperintense mass (B) is noted within the right fusiform gyrus (arrows) with low T1 signal and no enhancement (C). A histologic section shows a diffusely infiltrating glioma of low cellularity with no mitotic activity, microvascular proliferation, or necrosis (D). Immunohistochemical staining is positive for GFAP (E) and shows a low Ki-67 proliferation index (F). Targeted next-generation sequencing identified a QKI-NTRK2 fusion, suggestive of MAPK pathway alteration.
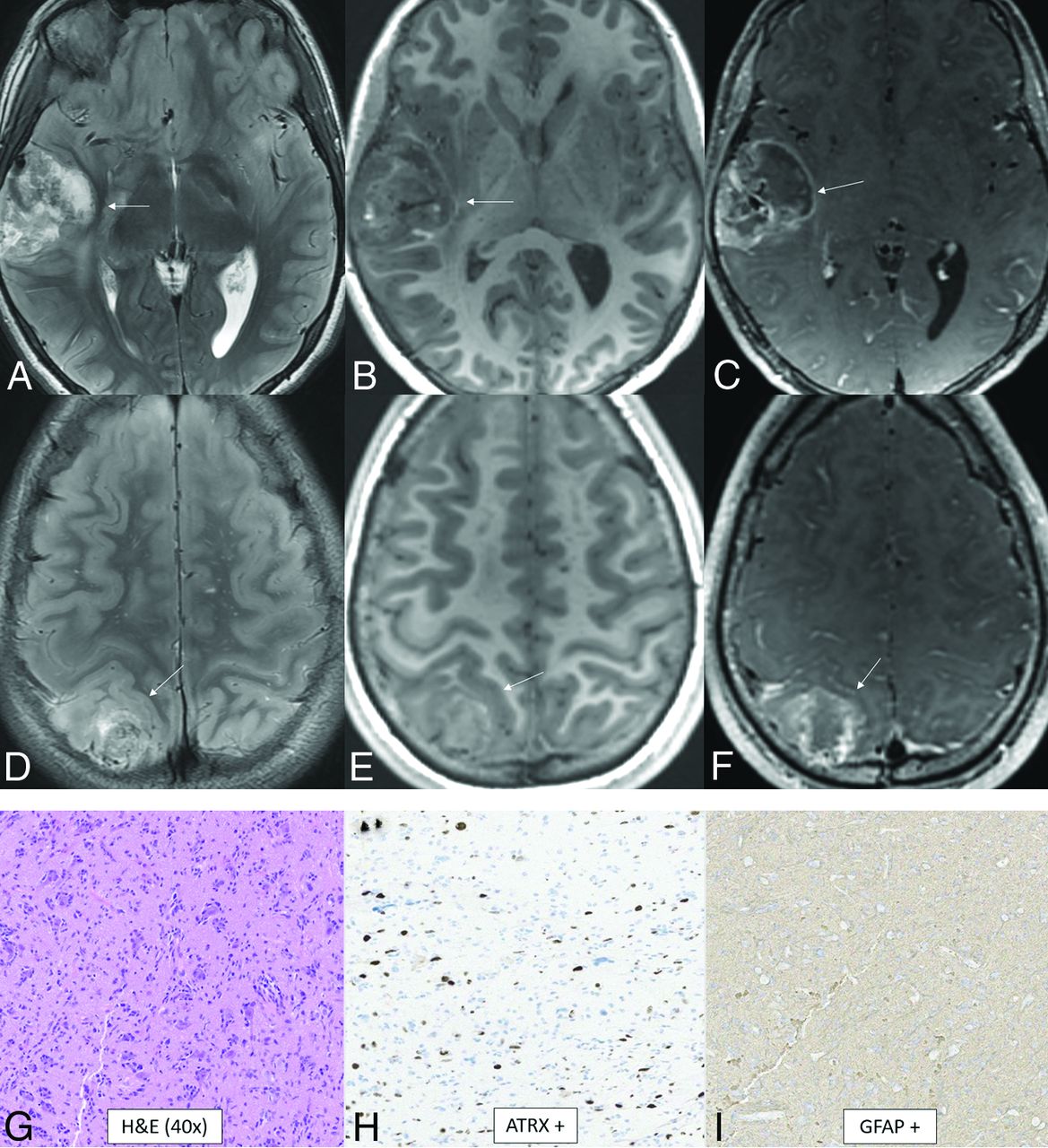
- FIG 4.
Diffuse hemispheric glioma, H3 G34-mutant. Multifocal masses are seen in the right temporal and parietal lobes. The temporal mass shows heterogeneously increased T2 signal (A), heterogeneously low T1 signal with a few foci of T1-hyperintense hemorrhage (B), and heterogenous enhancement (C, arrows). The parietal mass shows similar signal characteristics with heterogeneous T2-FLAIR hyperintensity (D), T1-hypointensity (E), and enhancement (F, arrows). The histologic section reveals an infiltrating glioma with astrocytic morphology (G). Glioma cells are positive for ATRX (H) and GFAP (I) stains and negative for IDH1 R132H and OLIG2. There was a high Ki-67 proliferation index of up to approximately 20%. This immunophenotype suggested a mutation of H3 G34, warranting further genomic evaluation. Next-generation sequencing revealed a somatic mutation in H3-3A (also known as H3F3A). Currently, there are no clinically approved therapies specifically targeting H3-3A mutations.
- FIG 5.
Diffuse pediatric-type high-grade glioma, H3 wild-type and IDH wild-type. MR images demonstrate diffusely infiltrating masses in the bilateral temporal lobes with mild mass effect, T2-FLAIR (A) and T2-hyperintensity (B, anterior arrows), and no enhancement (C). There is additional T2-FLAIR and T2-hyperintensity in the dorsal pons and posterior fossa leptomeningeal enhancement (posterior arrows). Histology reveals a high-grade diffusely infiltrating astrocytoma with high mitotic activity (D). The tumor shows ATRX retention (E) and wild-type IDH status (F) on immunohistochemical stains. Whole-genome methylation analysis showed a match to diffuse pediatric-type high-grade glioma. The tumor was H3 wild-type and IDH wild-type and had a TERT promoter mutation, which was identified on the neuro-oncology targeted next-generation sequencing panel.
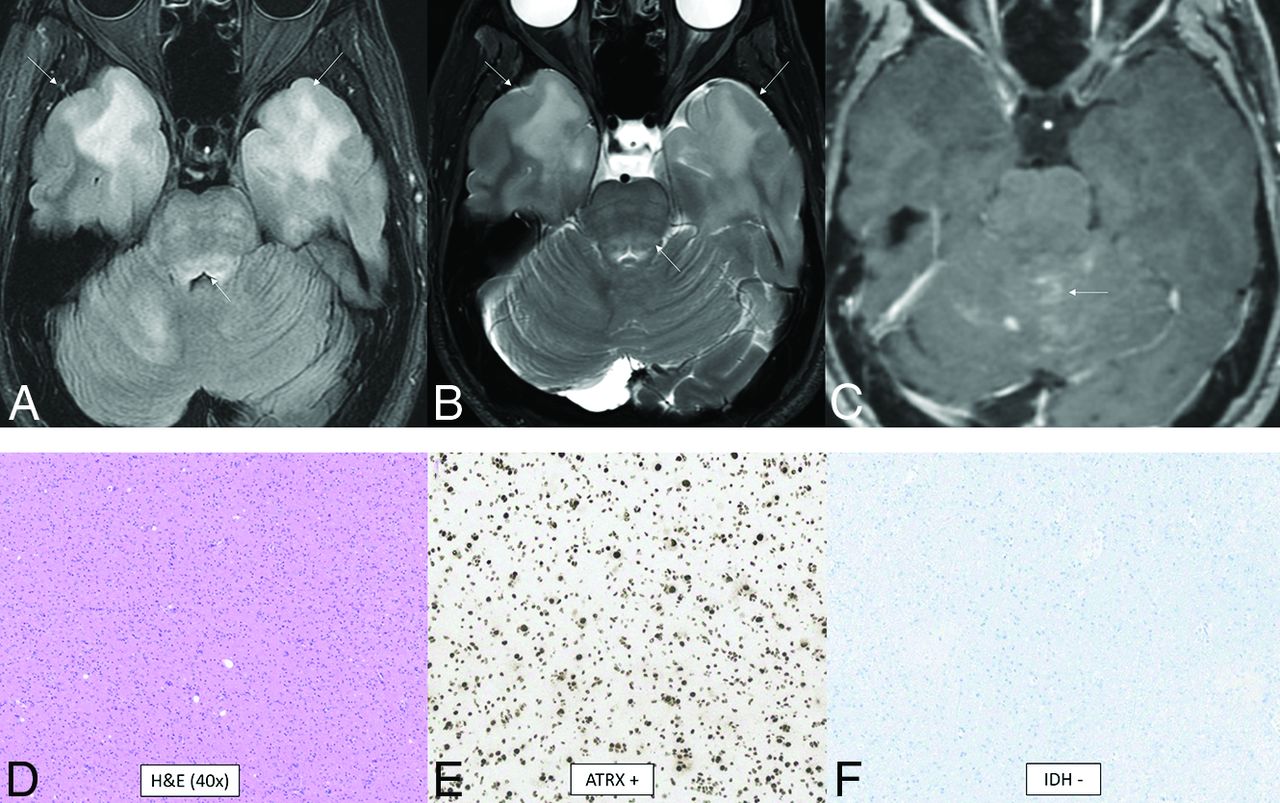
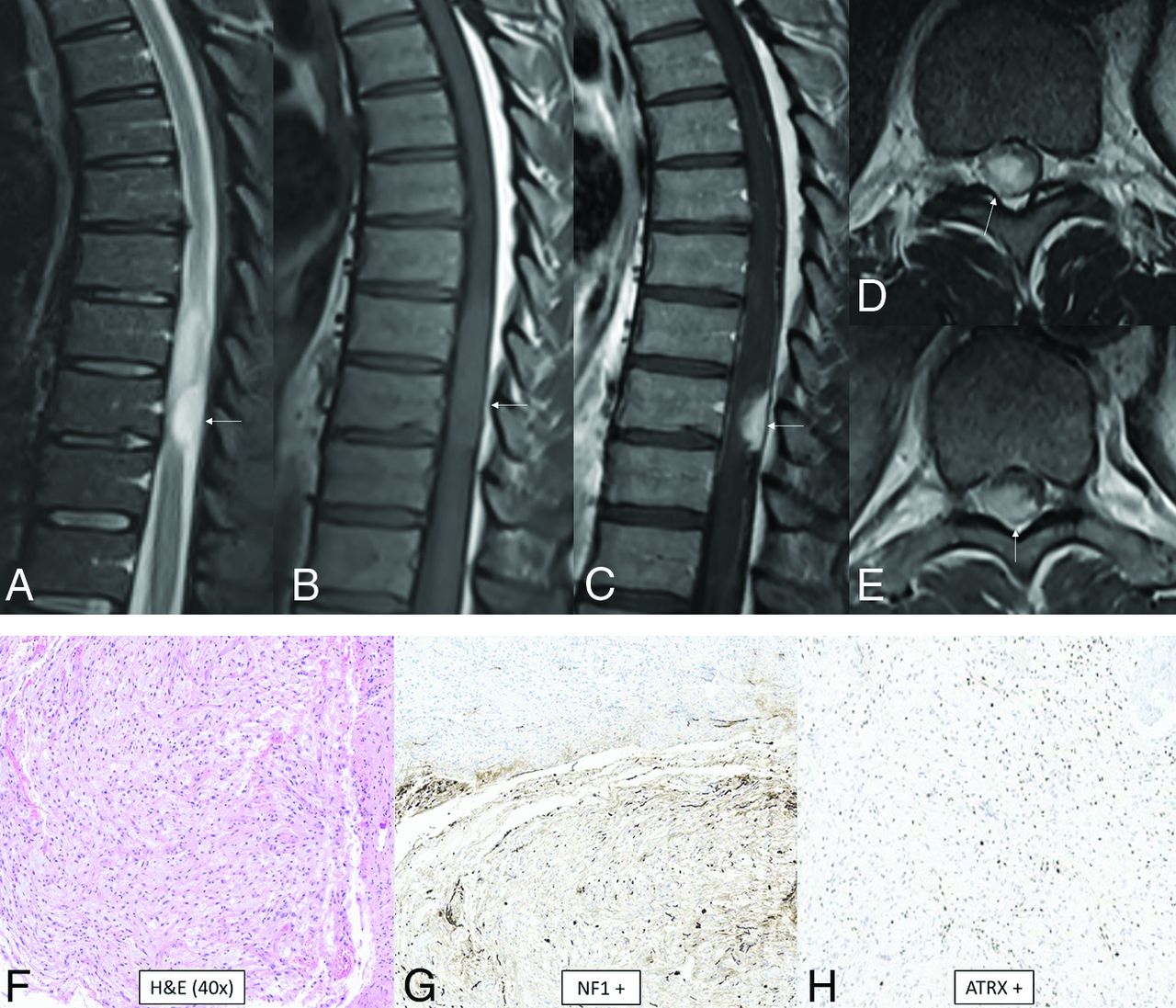
- FIG 6.
High-grade astrocytoma with piloid features. MR images demonstrate an eccentric T2-hyperintense mass (A) along the posterior thoracic cord with low T1 signal (B) and avid enhancement (C–E, arrows). Surrounding intramedullary T2-hyperintensity represents edema and/or tumor infiltration. Histology reveals an astrocytoma with piloid morphology (F), having NF1 (G) and ATRX (H) mutations in association with CDK2NA/B homozygous deletion. Whole-genome methylation profiling showed a match to high-grade astrocytoma with piloid features. Most of these tumors occur intracranially.
- FIG 7.
Diffuse glioneuronal tumor with oligodendroglioma-like features and nuclear clusters (provisional type). CT and MR images demonstrate a large well-circumscribed mass centered at the left atrium with involvement of the left parietal lobe and transcallosal extension to the right hemisphere. The tumor shows T2-hyperintensity (A), T1-hypointensity (B), patchy heterogeneous enhancement (C), and dense calcification (D). The histologic section demonstrates a highly cellular infiltrating glioma with oligodendroglioma-like microcyst formation (arrow, E) and extensive calcification. The tumor cells show moderate, clear cytoplasm and round-to-elongated, irregular, and hyperchromatic nuclei with high mitotic activity. The tumor cells are diffusely positive for OLIG2 (F) and negative for IDH1 R132H (G) and H3 K27M by immunohistochemistry. Whole-genome methylation analysis confirmed the final integrated diagnosis of diffuse glioneuronal tumor with oligodendroglioma-like features and nuclear clusters.
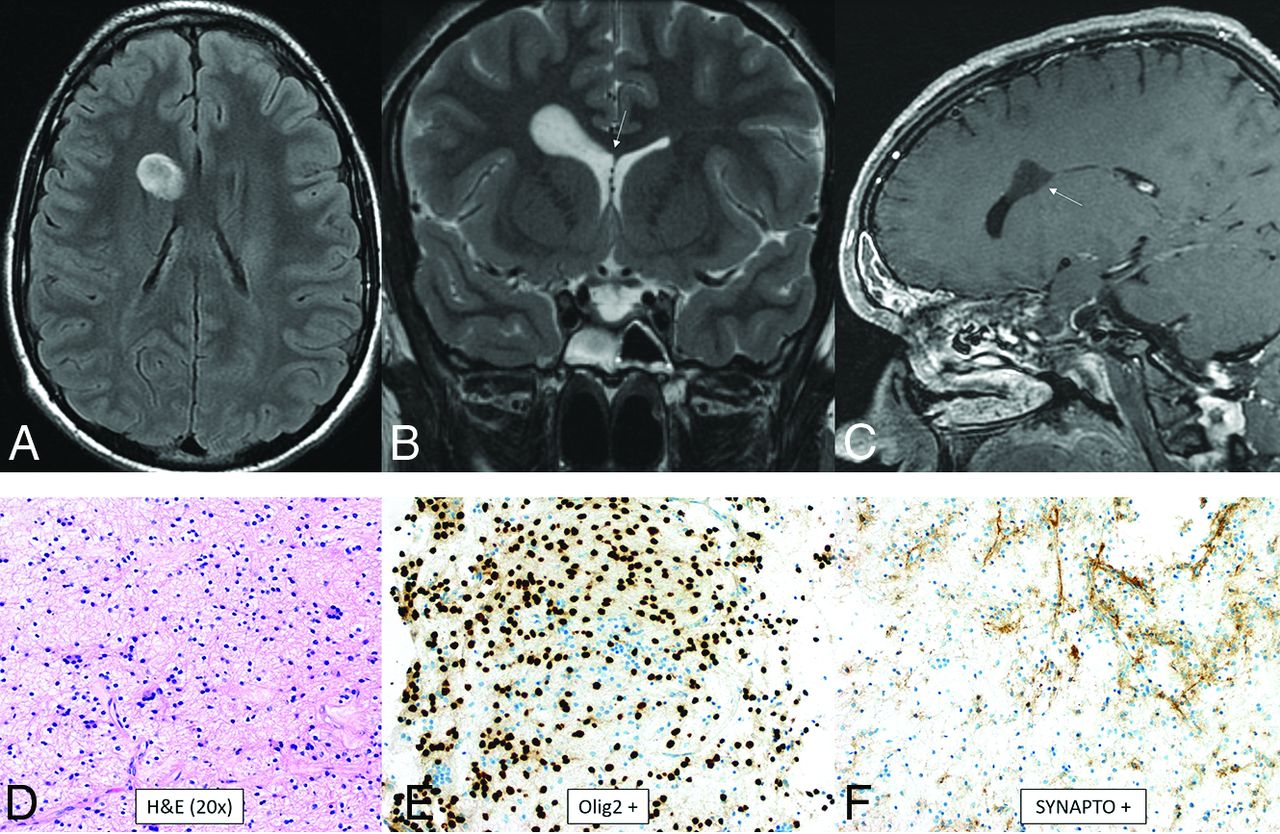
- FIG 8.
Myxoid glioneuronal tumor. MR imaging shows a mass in the right frontal horn region with peripheral T2-FLAIR hyperintensity and relative central T2-FLAIR hypointensity (A), which is slightly hypointense to CSF on the T2-weighted image (B), approaches the septum pellucidum (arrow, B), and does not enhance (C). There is no adjacent edema. Histology shows an oligodendroglioma-like appearance with moderate cellularity and uniform round nuclei with a circumferential arrangement around delicate vessels (D). Immunohistochemical staining is positive for OLIG2 (E), synaptophysin (F), and GFAP and negative for NeuN. This tumor has a PDGFRA p.K385 mutation and lacks FGFR1 abnormalities. Dysembryoplastic neuroepithelial tumor is a histologic mimic but has a mutation of FGFR1.
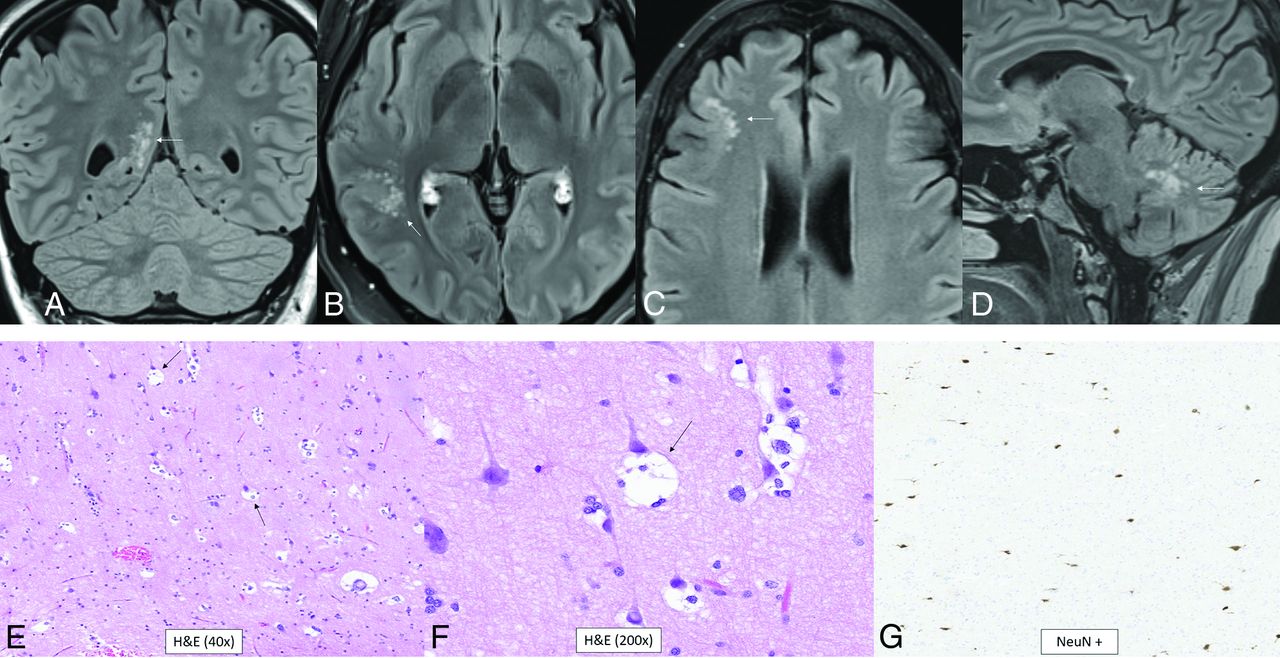
- FIG 9.
Multinodular and vacuolating neuronal tumor. Four different patients with pathology-proved (A, and E–G) and radiologic (B–D) diagnoses. T2-FLAIR images show small, subcortical clusters of hyperintense nodules with no edema or mass effect (A–D, arrows). Histology shows “neuronal” tumor cells with eosinophilic cytoplasm (E), multiple intracytoplasmic vacuoles that markedly enlarge the cytoplasm (arrows, E and F), and perineuronal satellitosis. There is positive NeuN staining of the viable normal scattered pyramidal neurons with negative staining of the tumor cells (G).
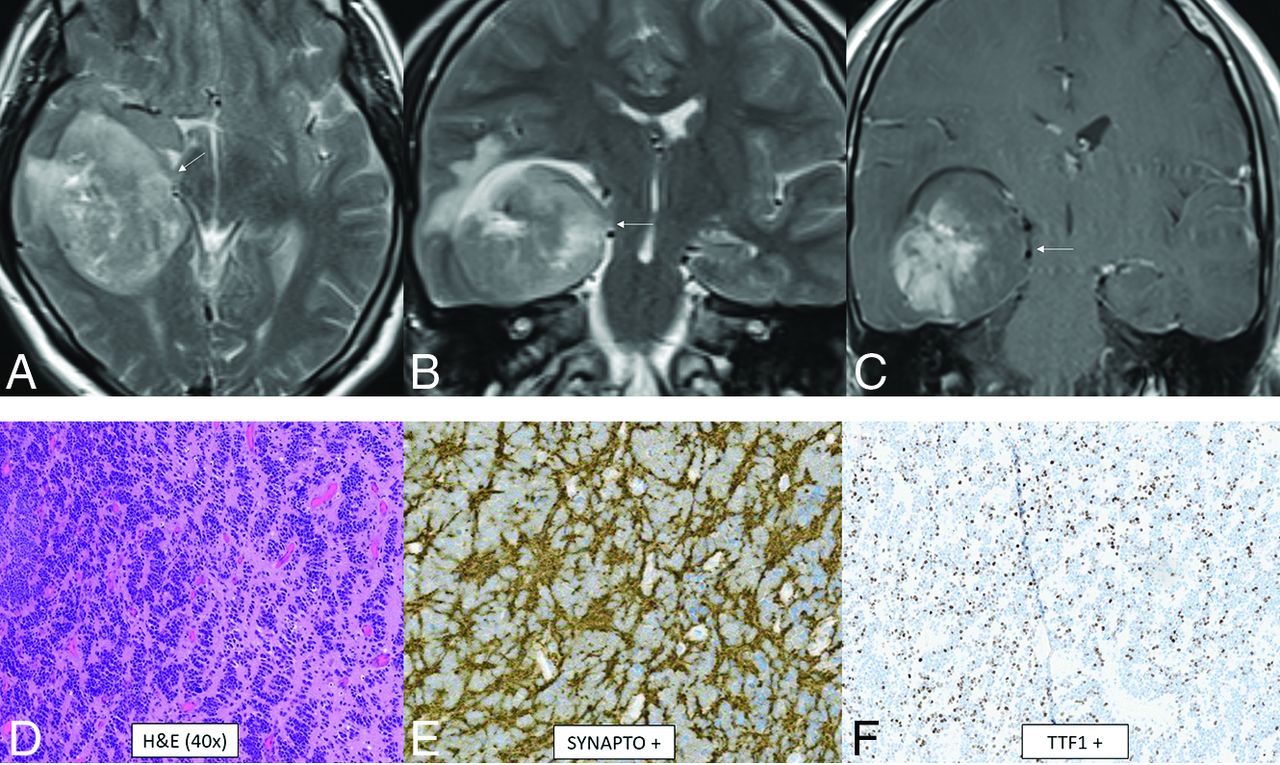
- FIG 10.
CNS neuroblastoma, FOXR2-activated. MR images show a large cortical and subcortical well-circumscribed expansile mass in the right temporal lobe involving the hippocampus (arrows) with T2-hyperintensity (A and B) and patchy enhancement (C). Histology shows a highly cellular infiltrating neuroepithelial neoplasm with a complex pattern, including an undifferentiated and extensive spongioblastoma pattern with brisk mitotic activity (D). On immunohistochemistry, the tumor shows divergent differentiation with expression of synaptophysin (E), OLIG2, and TTF1 (F). Whole-genome methylation profiling indicated a match to CNS neuroblastoma, FOXR2-activated.
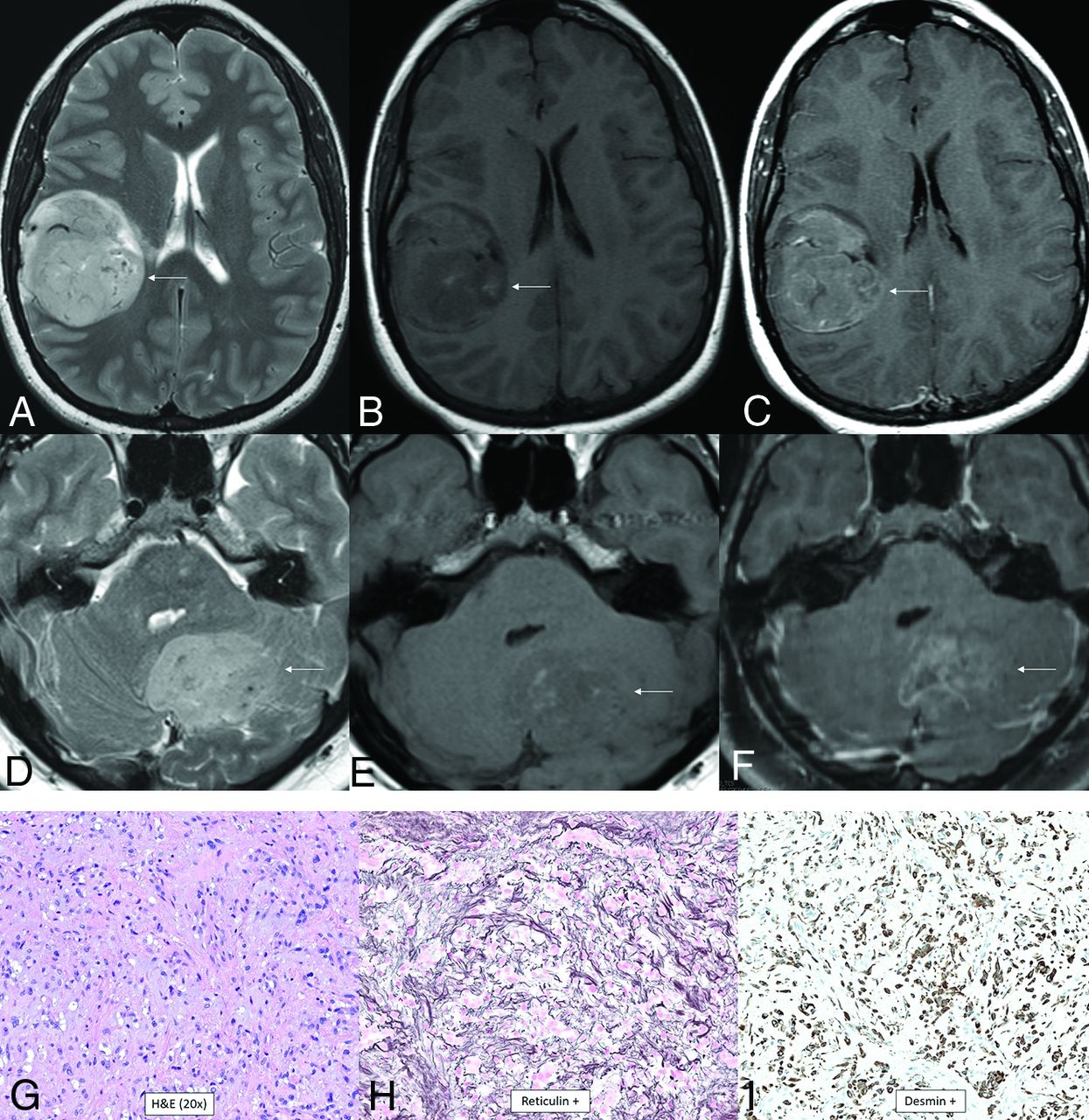
- FIG 11.
CNS tumor with BCOR internal tandem duplication. In 1 patient (A–C), there is a large well-circumscribed mass in the right posterior frontal lobe with heterogeneous T2-hyperintensity and prominent intratumoral vessels (A), heterogeneous T1-hypointensity (B), and enhancement (C, arrows). In a different patient (D–F), there is similar signal and morphology of a mass centered in the left cerebellar hemisphere on the T2-weighted (D), T1-weighted (E), and T1-weighted postcontrast (F) images (arrows). Histology from the first patient is characterized by relatively uniform nuclei, perivascular arrangement of tumor cells (rosette formation), and necrosis without microvascular proliferation (G). Immunohistochemical stains demonstrate OLIG2 positivity (H) and consistent NeuN positivity (I). Next-generation sequencing identified a frameshift mutation in BCOR, and chromosomal microarray demonstrated a segmental chromosomal loss disrupting BCOR.
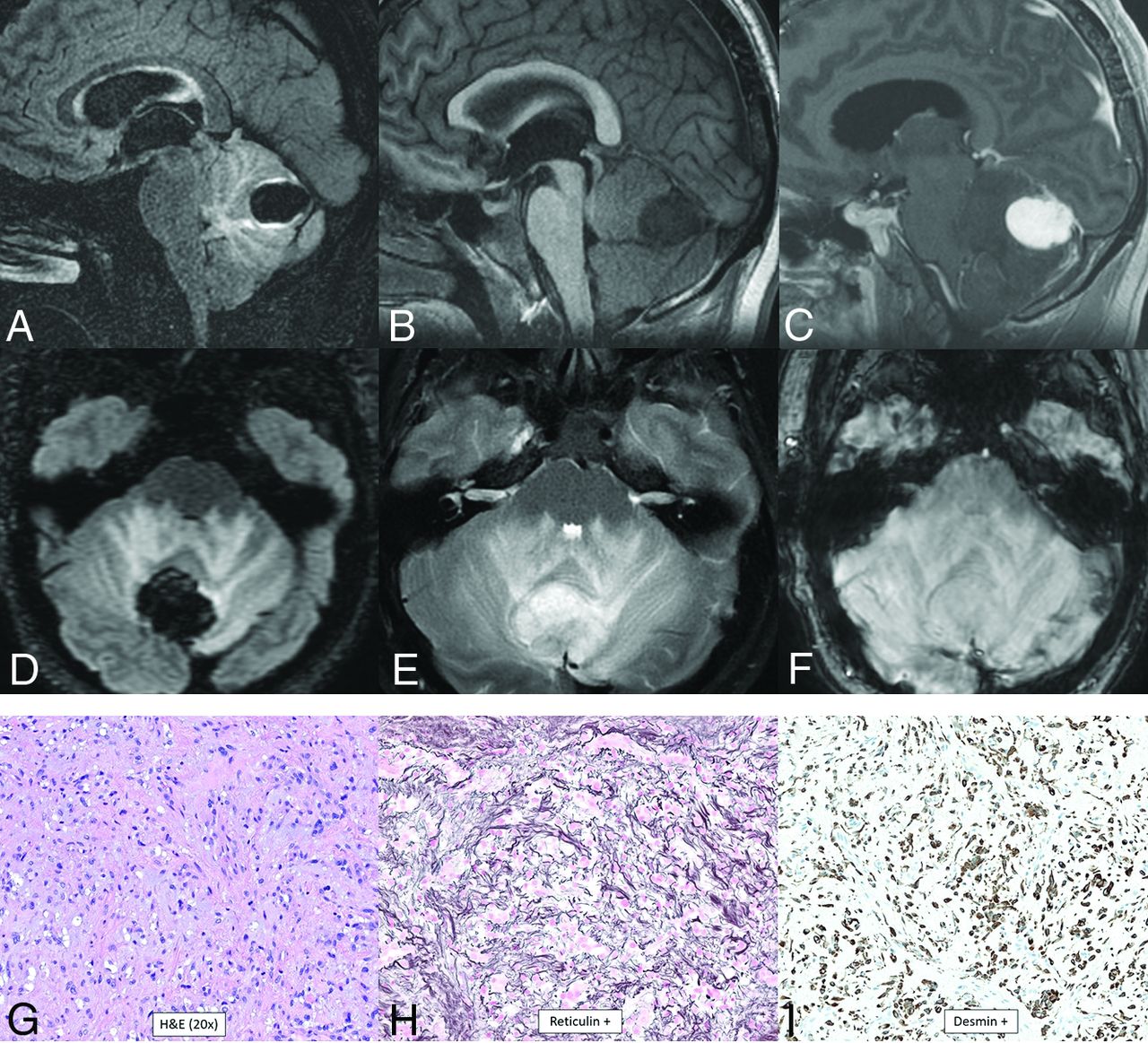
- FIG 12.
Intracranial mesenchymal tumor, FET-CREB fusion–positive (provisional type). Sagittal (A–C) and axial (D–F) MR images demonstrate a lobulated circumscribed mass along the superior vermis. The mass is markedly T2-FLAIR hypointense (A and D), T1-hypointense (B), homogeneously enhancing (C), and T2-hyperintense (E), with marked surrounding vasogenic edema. There is a lack of hypointensity within the tumor on the susceptibility-weighted image (F). Histology demonstrates a mesenchymal neoplasm with low-grade features (G), with staining positive for reticulin (H) and desmin (I), markers of connective tissue and muscle, respectively. The marked T2-FLAIR hypointensity corresponding to the area of homogeneous enhancement is an atypical appearance.
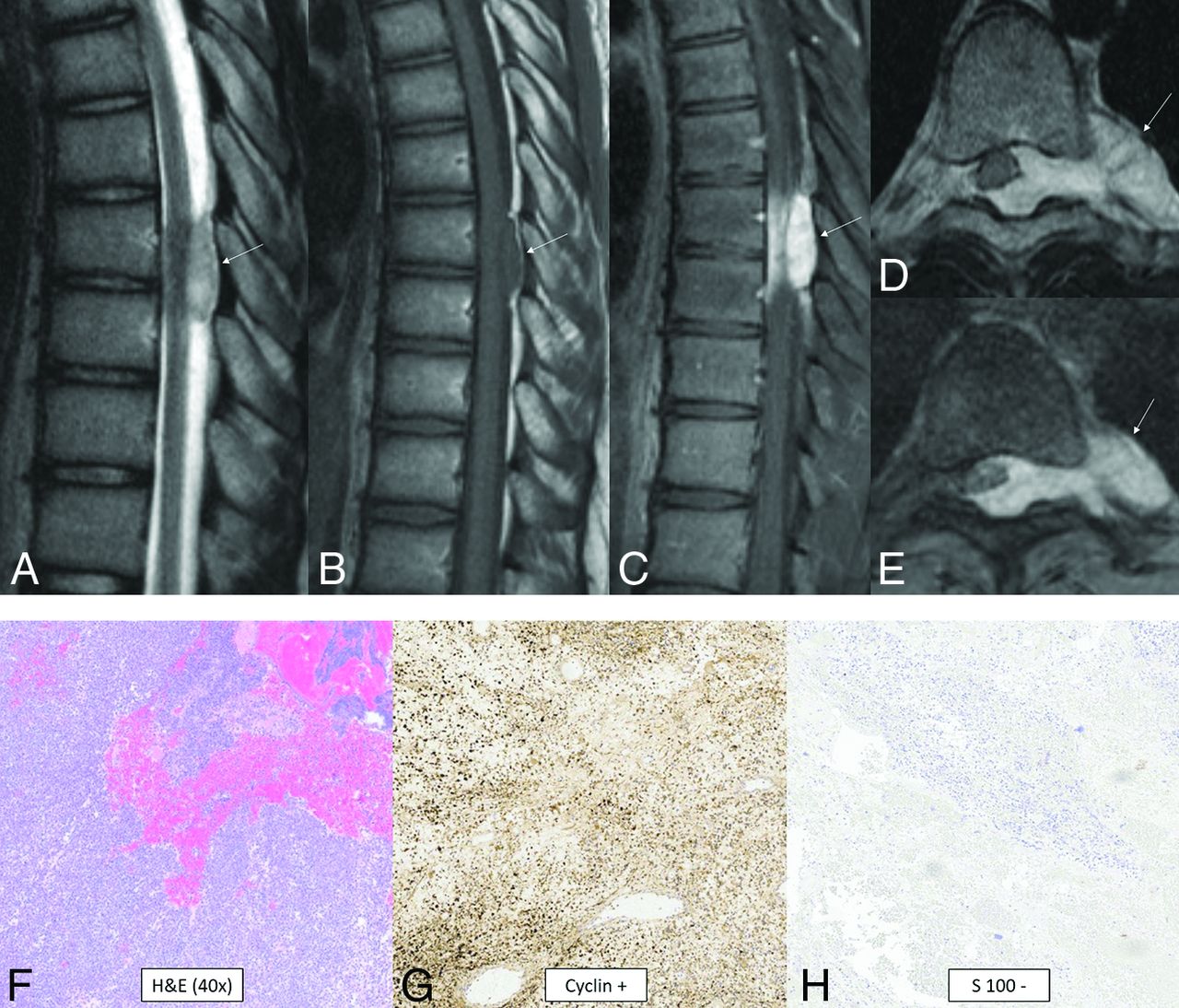
- FIG 13.
CIC-rearranged sarcoma. MR images reveal a small well-circumscribed peridural mass in the midthoracic region (arrows). The mass is T2-hyperintense (A), T1-isointense (B), and avidly enhances (C–E). The tumor extends through the left neural foramen into the paraspinal space and also exerts moderate mass effect on the cord, displacing it to the right (D and E). Histology reveals small, round, sarcomatous cells (F) with molecular stains of neoplastic cells positive for cyclin (G), calretinin, WT1 (focal), and CD99 (patchy) and negative for S-100 (H), CK, EMA, desmin, and synaptophysin. Fluorescence in site hybridization showed a balanced rearrangement of the CIC locus in 91% (181/200) of the nuclei.

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Mesenchymal Nonmeningothelial Tumors of the CNS: Evolving Molecular Landscape and Implications for Neuroradiologists
- Imaging Features of Primary Intracranial Sarcoma with DICER1 Mutation: A Multicenter Case Series
- High-Grade Astrocytoma with Piloid Features: A Dual Institutional Review of Imaging Findings of a Novel Entity