
Abstract
BACKGROUND AND PURPOSE: There is limited discussion in current literature about the normal imaging appearance of the round window. The purpose of this study was to assess the prevalence and imaging characteristics of gadolinium enhancement in the round window niche on MR imaging to the internal auditory canal.
MATERIALS AND METHODS: The presence or absence and laterality of enhancement in the round window niche on MR imaging was retrospectively reviewed in 95 patients from 1 institution. All studies included high-resolution (≤0.5-mm section thickness) pre- and postgadolinium 3D FSE T1 with fat-saturation and postgadolinium 3D FLAIR image sequences. T1 and T2 acquisitions were viewed as coregistered overlays to confirm that enhancement was lateral to the round window membrane within the round window niche. CT was reviewed when available to assess the presence and laterality of soft tissue in the round window niche.
RESULTS: Ninety-five patients with internal auditory canal MRIs were included. Enhancement was present in the round window of 15 of 95 patients (15.8%). Of the 27 patients who underwent CT, 4 (14.8%) had concordant soft tissue on CT and MR imaging enhancement in the round window niche. One patient had MR imaging enhancement within the round window niche without a corresponding abnormality on CT. The absence of soft tissue on CT and the corresponding lack of MR imaging enhancement were present in 22 (81.5%) patients.
CONCLUSIONS: Enhancement can be visualized within the round window niche on MR imaging as an incidental finding. This enhancement probably represents postinflammatory granulation tissue and does not require further intervention. However, the potential for this enhancement to be misdiagnosed as a pathologic process can be a pitfall in MR imaging.
ABBREVIATIONS:
- ENT
- ear, nose, and throat
- FS
- fat-saturation
- IAC
- internal auditory canal
- RW
- round window
- RWN
- round window niche
The round window (RW) is an opening between the middle and inner ear, located along the posterior aspect of the cochlear promontory. It acts as the boundary between the basal turn of the cochlea and the round window niche (RWN) of the mesotympanum. Functionally, the RW vibrates with an opposite phase to vibrations from the oval window, resulting in cochlear fluid movement.1,2
Given the proclivity of middle ear pathologies to affect the ossicular chain and oval window, the RW is often overlooked. Nevertheless, accurate assessment of the RW and RWN is crucial for both diagnostic and preoperative planning purposes.3,4 Overall, isolated RWN pathology is rare, though developmental anomalies, otitis media, otosclerosis, and labyrinthitis ossificans can affect this region.1 Enhancement isolated to the RWN should not be confused with intralabyrinthine schwannomas5,6 or small paragangliomas, which usually arise from the cochlear promontory or extend along Jacobson nerve from the anterior wall of the jugular foramen.7
More commonly, nonmalignant, inflammatory abnormalities are found in this region, including fluid, proteinaceous debris and granulation tissue. These benign findings can demonstrate enhancement on MR imaging and may be confused with more sinister entities. For example, the authors of this study have previously encountered several situations in which enhancement on MR imaging was mistakenly noted to be present at the lateral aspect of the basal turn of the cochlea. Precise localization actually revealed that the enhancement was within the RWN, which excluded the possibility of an intracochlear schwannoma. In the current literature, the expected prevalence of enhancement in the RWN region is unknown. Thus, this study set out to assess the frequency of enhancement in the RWN with correlation of opacification on CT imaging.
MATERIALS AND METHODS
Following institutional review board approval, sequentially obtained internal auditory canal (IAC) protocol MR imaging examinations performed between March 1, 2021, and April 20, 2021, were compiled. MR imaging examinations were obtained on 3T Magnetom scanners (Skyra, Verio, and Prisma; Siemens) and included high-resolution 3D sampling perfection with application-optimized contrasts by using different flip angle evolution (3D SPACE sequence; Siemens) FSE T2 (TR, 1300 ms; TE, 162 ms; section thickness, 0.6 mm), axial T1 SPACE pregadolinium (TR, 600 ms; TE, 30 ms; section thickness, 0.90 mm), 3D SPACE FLAIR (TR, 5000 ms; TE, 345 ms; section thickness, 1.20 mm), and postgadolinium sagittal T1 fat-saturation (FS) SPACE (TR, 650 ms; TE, 14 ms; section thickness, 0.90 mm), which is a part of our institution’s standard IAC protocol. Patients were scanned with a 32- or 64-channel head coil. In total, there were 100 patients who had an IAC MR imaging, with 5 ultimately excluded due to incomplete MR imaging. Of these, 27 (28.4%) patients had a prior temporal bone CT that could be used for evaluation of the presence of soft tissue in the RW.
Imaging and Clinical Review
The IAC MRIs were independently reviewed by 2 fellowship-trained neuroradiologists with Certificates of Added Qualification. The neuroradiologists independently reviewed the postcontrast 3D SPACE FSE T1 coregistered with 3D SPACE FSE T2 to localize the RWN and determine the presence or absence and laterality of enhancing granulation tissue (Fig 1). CT scans of patients ranging from 3 days to 19 years before the MR imaging were also assessed when available for the presence or absence and laterality of soft tissue in the RWN. Discrepancies were resolved via consensus review. Demographic information including age, sex, surgical history, and ear, nose and throat (ENT) diagnosis was obtained from the institution’s electronic medical records for the entire cohort.

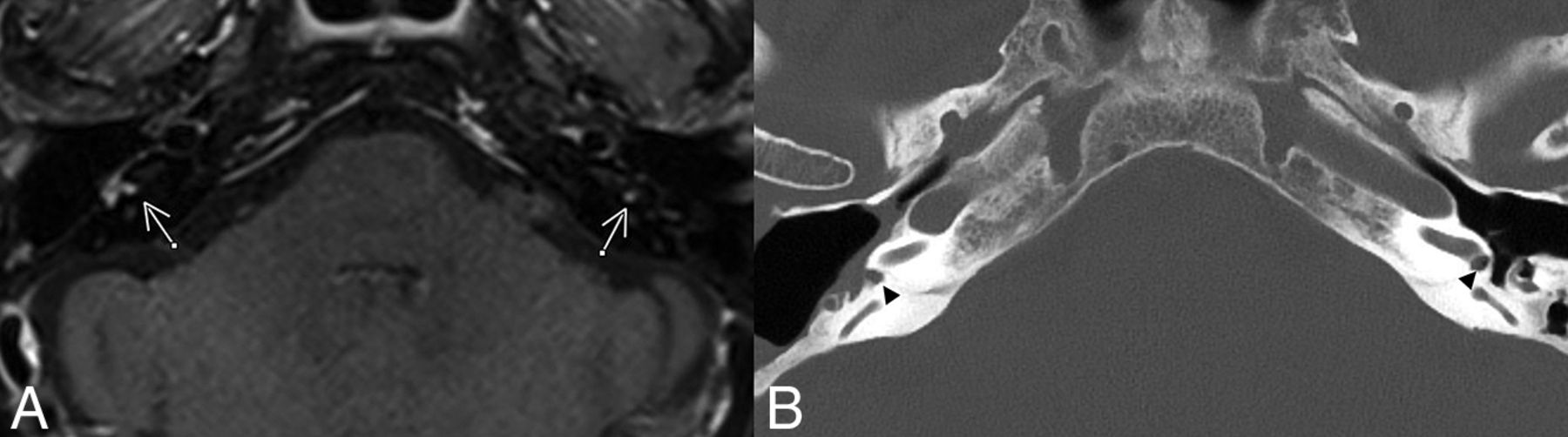
Example of enhancing granulation tissue in the RW. A, Axial postcontrast FS T1WI demonstrates enhancement present bilaterally in the RWs (arrows). B, Axial head CT with thin-section bone window reconstructions demonstrates a right-sided canal wall-down mastoidectomy for resection of a cholesteatoma. Opacification of the round windows can be seen bilaterally, correlating to the area of enhancement (arrowheads).
RESULTS
There were 95 (53 women; 55.8%) patients who made up the cohort, with 190 RWNs evaluated on MR imaging. The average patient age was 58 years (range, 18–84 years) (Table 1). In total, RWN enhancement was noted on the MR imaging of 15/95 patients (15.8%). Twenty-seven patients had a CT scan. There were 4 (14.8%) patients who had RWN enhancement on MR imaging and corresponding abnormal opacification on CT within the RW. A single patient had RWN enhancement on MR imaging without a corresponding abnormality on CT. The remaining 22 (81.5%) patients did not have an abnormality in the RWN on MR imaging or CT (Table 2).
Summary of patient demographics, reasons for initial ENT visit, and relevant medical history relating to temporal bone
Summary of MR imaging and CT findings
Hearing loss was the most common presentation, comprising 51 patients (53.7%), while tinnitus, dizziness, temporal bone mass, and headache represented the remainder of the presentations (Table 1). Twenty-four patients (25.3%) were found to have a mastoid effusion on MR imaging, 6 of whom also had RW enhancement on MR imaging. Eight patients (8.4%) had an operation on their temporal bones before their MR imaging. Two patients (2.1%) were noted to have granulation tissue in the RW on their chart, one based on imaging and the other on surgical assessment. Both patients were found to have enhancement on MR imaging and soft tissue on CT in the RW.
DISCUSSION
The purpose of this study was to evaluate the prevalence of enhancement in the RWN on high-resolution MR imaging. We found that enhancement in the RW on MR imaging is not uncommon. It is present in 15.8% of cases, even without past surgery. Although CT was not available for all patients in this study, 1 of 5 patients who did have a CT scan and had RWN enhancement on MR imaging did not have a concordant abnormality on CT. To our knowledge, this represents the first description of incidental enhancement in the RWN on MR imaging.
Enhancement of the RWN is a potential pitfall in the imaging evaluation of this region and should not be confused with pathology when observed as an isolated finding. On MR imaging, RWN enhancement will be located lateral to the RW membrane at the level of basal turn of the cochlea. Coregistration with thin-section 3D T2WI or correlation with any concurrent CT imaging will localize the abnormality to the RWN, excluding the possibility of pathology, such as an intralabyrinthine schwannoma or a small glomus tympanicum.
Prior studies describing the anatomic appearance of the RWN on imaging are scarce. Veillon et al8 discussed some normal and pathologic RW and RWN findings on CT. They highlighted the importance of imaging in the detection of otosclerotic foci, congenital stenosis, and perilymphatic fistula. Other studies in the literature have described the anatomic landmarks of the RW to guide cochlear implantation procedures.9
Roßberg et al,10 in their retrospective study of conebeam CT examinations in 27 patients before treatment with intratympanic steroids, found granulation tissue obscuring the RWN in 15% (4/27) of patients, similar to our results with a larger cohort. Schachern et al11 found histologic evidence of granulation tissue in the RWN following experimentally induced otitis media in a cat model. In his postmortem study of 26 temporal bones in patients with a history of chronic otitis media, Djeric12 found histologic evidence of fibroproliferative or granulation processes in the RWN in all cases. In most of these cases, the inflammatory changes were characterized by cellular debris and cystic spaces containing acidophilic fluid. This finding probably explains the increased T2 signal in the RWN that we observed in several cases of RWN contrast enhancement (Fig 2).

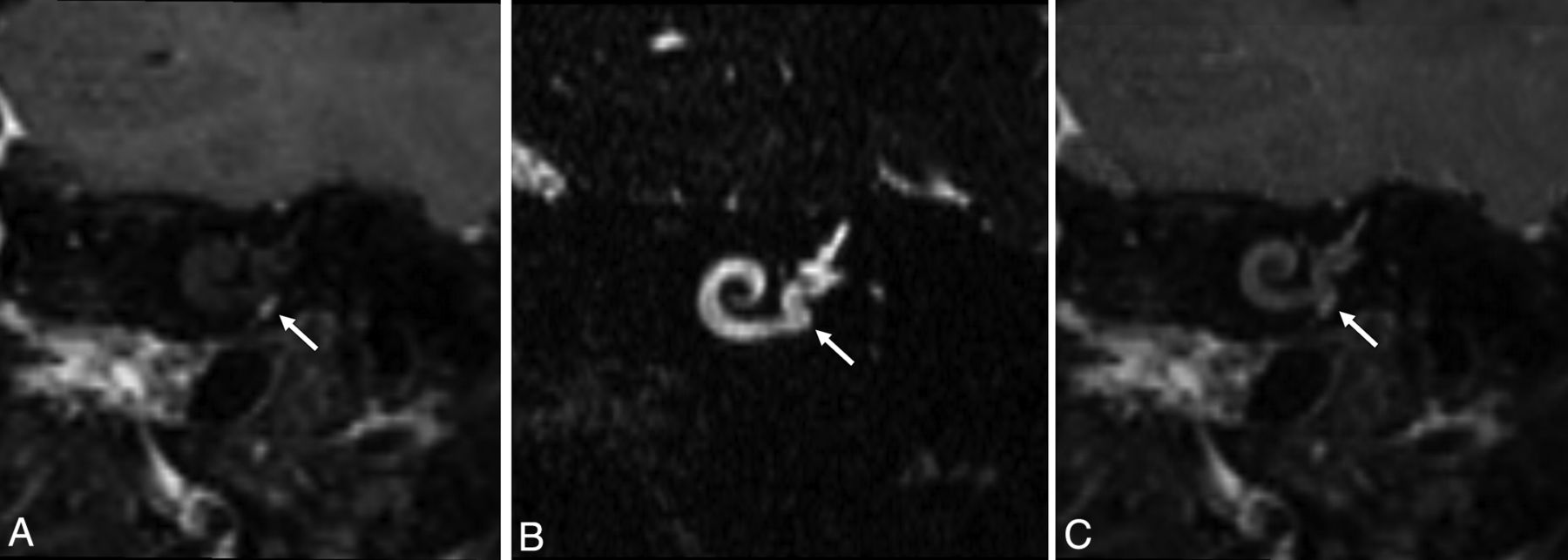
A, Postcontrast FS T1WI reconstructed in the Stenvers view demonstrates focal contrast enhancement. B, Thin-section 3D SPACE T2WI reconstructed in the Stenvers view demonstrates fluid signal throughout the basal turn of the cochlea as well as hyperintense signal lateral to the RW membrane (white arrow). Specifically, there is no filling defect within the basal turn of the cochlea. C, Coregistered overlay of the 3D SPACE T2WI and postcontrast FS T1WI illustrate that the enhancement is located lateral to the basal turn and entirely within the RWN (white arrow). Without the aid of the T2 SPACE and coregistration, it would be possible to misdiagnose a small intralabyrinthine schwannoma in the basal turn or a glomus tympanicum. The white arrow in A is the focal enhancement.
The differential diagnosis of isolated RWN enhancement on MR imaging is quite limited. Several of our cases demonstrated inflammatory changes elsewhere within the middle ear and mastoid air cells, supporting the diagnosis of granulation tissue (Fig 1). Intralabyrinthine schwannomas can extend into the RWN from the basal turn of the cochlea, but no evidence of cochlear enhancement on T1 or filling defects on T2 was observed in any of our cases. Tumor extension into the RWN can be seen with skull base meningiomas or paragangliomas, but again no evidence of adjacent skull base tumor was observed in this cohort.
This study has several limitations. First, it was conducted at a single institution, and the imaging reviewed was retrospective. Next, a small minority of patients had CT images available for comparison reviews. Finally, there was not surgical confirmation in all cases with imaging abnormalities. However, given prior reports of granulation tissue at this location and surgical confirmation of granulation tissue in 1 patient with RWN enhancement on MR imaging, it is likely that the MR imaging and CT findings of this cohort also represent granulation tissue.
CONCLUSIONS
Enhancement in the RWN is well-seen on high-resolution MR imaging and can be a potential pitfall in the interpretation of imaging. In the absence of other findings, the enhancement likely represents granulation tissue and may likely not require further imaging or intervention.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received August 29, 2022.
- Accepted after revision December 31, 2022.
- © 2023 by American Journal of Neuroradiology




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.