
Abstract
BACKGROUND AND PURPOSE: One of the perplexing findings of fetal brain MR imaging is white matter T2 hyperintense signal. The aims of our study were initially to determine the main etiologies associated with white matter T2 hyperintense signal, then to examine whether the different etiologies have different ADC values, and, last, to assess the association of white matter T2 hyperintense signal with developmental outcome.
MATERIALS AND METHODS: This was a prospective cohort study of 44 MR imaging scans of fetal brains obtained for suspected brain pathologies at a tertiary medical center during 2011–2015. Clinical data were collected from electronic medical charts. ADC values were measured and averaged in the frontal, parietal, occipital, and temporal lobes. Neurodevelopmental assessments were performed with the Vineland Adaptive Behavior Scales II.
RESULTS: Half of the cases of MRI hyperintense T2 signal of the fetal brain were associated with congenital cytomegalovirus infection. The other half were mainly idiopathic. Thus, the study group was divided to subgroups positive and negative for cytomegalovirus. Both groups had hyperintense signal in the temporal lobe. The group positive for cytomegalovirus had involvement of the parietal lobe. Only this group had increased ADC values in the temporal and parietal lobes. There was no association between the neurodevelopment outcome and the etiologies or ADC values.
CONCLUSIONS: T2 hyperintense signal in fetal brain MRI associated with positive cytomegalovirus infection has increased ADC values in the temporal and parietal lobes, suggestive of brain edema in these areas. However, the association between this finding and neurodevelopment outcome requires further evaluation.
ABBREVIATIONS:
- CMV
- cytomegalovirus
- fbMRI
- fetal brain MRI
- ICC
- interclass correlation coefficient
- VABS
- Vineland Adaptive Behavior Scales II
- WMHS
- white matter hyperintense signal
Fetal brain MR imaging (fbMRI) has been increasingly used in recent years as a means of tracking normal and pathologic fetal brain maturation.1 One of the perplexing findings of fbMRI is white matter T2 hyperintense signal (WMHS). On the one hand, it has been associated with in utero brain pathologies, such as ischemia and cytomegalovirus (CMV) infection.2⇓–4 On the other hand, the validity and relevance of this finding have been questioned.5
In recent years, DWI and its ADC metric have become a quantitative method for evaluation of fetal brain maturation.6 Previous studies showed that ADC values of the developing fetal brain correlate with fetal brain maturation.7⇓⇓⇓–11 Deviation from normal ADC values has been shown to be associated with brain pathologies such as ischemia, CMV infection, and ventriculomegaly.2,12,13 Postmortem studies of animal and human fetuses with hypoxic-ischemic brain injury have demonstrated a transition from low ADC values after the injury to increased values 7 days after the injury. This transition was associated with histologic findings changing from initial cytotoxic edema and swollen astrocytes to vasogenic edema, astrogliosis, and abundance of macrophages.2,14 Thus, ADC and its association with histopathology could be used to test the validity and meaning of T2 hyperintensity.
The aims of our study were initially to determine the main etiologies associated with WMHS, then to examine whether the different etiologies have different ADC values, and, last, to assess the association of WMHS with developmental outcome.
Materials and Methods
Subjects
This was a prospective cohort study of women who were referred for fetal brain MR imaging to our tertiary medical center, Sheba Medical Center, Ramat Gan, Israel, between 2011 and 2015. The cohorts for this study were chosen on the basis of identification of a hyperintense signal on the T2-weighted sequences. Demographic and clinical data were collected from the electronic records of each patient.
Data obtained from the records included maternal history, prenatal screening tests, imaging results from anatomic sonography and MR imaging, maternal CMV status, and perinatal history. Fetal cytomegalovirus infection was confirmed by either amniocentesis performed during pregnancy or by the presence of CMV DNA in neonatal urine or saliva.
The study was approved by Sheba Medical Center, Ramat Gan, Israel, institutional ethics board. Informed consent was obtained from each participant in the study prospectively.
MR Imaging Scans
Fetal brain MR imaging was performed using a 1.5T system (Optima MR450w with GEM Suite; GE Healthcare, Milwaukee, Wisconsin). Single-shot fast spin-echo T2-weighted sequences in 3 orthogonal planes were performed using a half-Fourier technique (NEX = 0.53) with the following parameters: section thickness, 3 or 4 mm; no gap; flexible coil (8-channel cardiac coil). FOV was determined by the size of the fetal head with a range of 24 × 24 to 30 × 30 cm; acquisition time was between 40 and 45 seconds (matrix, 320 × 224; TE, 90 ms; TR, 1298 ms; pixel bandwidth, 122 Hz/pixel; specific absorption rate values, 1.1–1.7 W/kg). A DWI sequence in 1, 2, or 3 orthogonal planes was then performed, with a 40-cm FOV, b-values of 0 and 700 ms, and a slice thickness of 4 mm with no gap. All MR images were obtained by the same protocol at our institution and assessed by a specialist in fetal sonography and a neuroradiologist expert in MR imaging as previously published.15
Target Variables
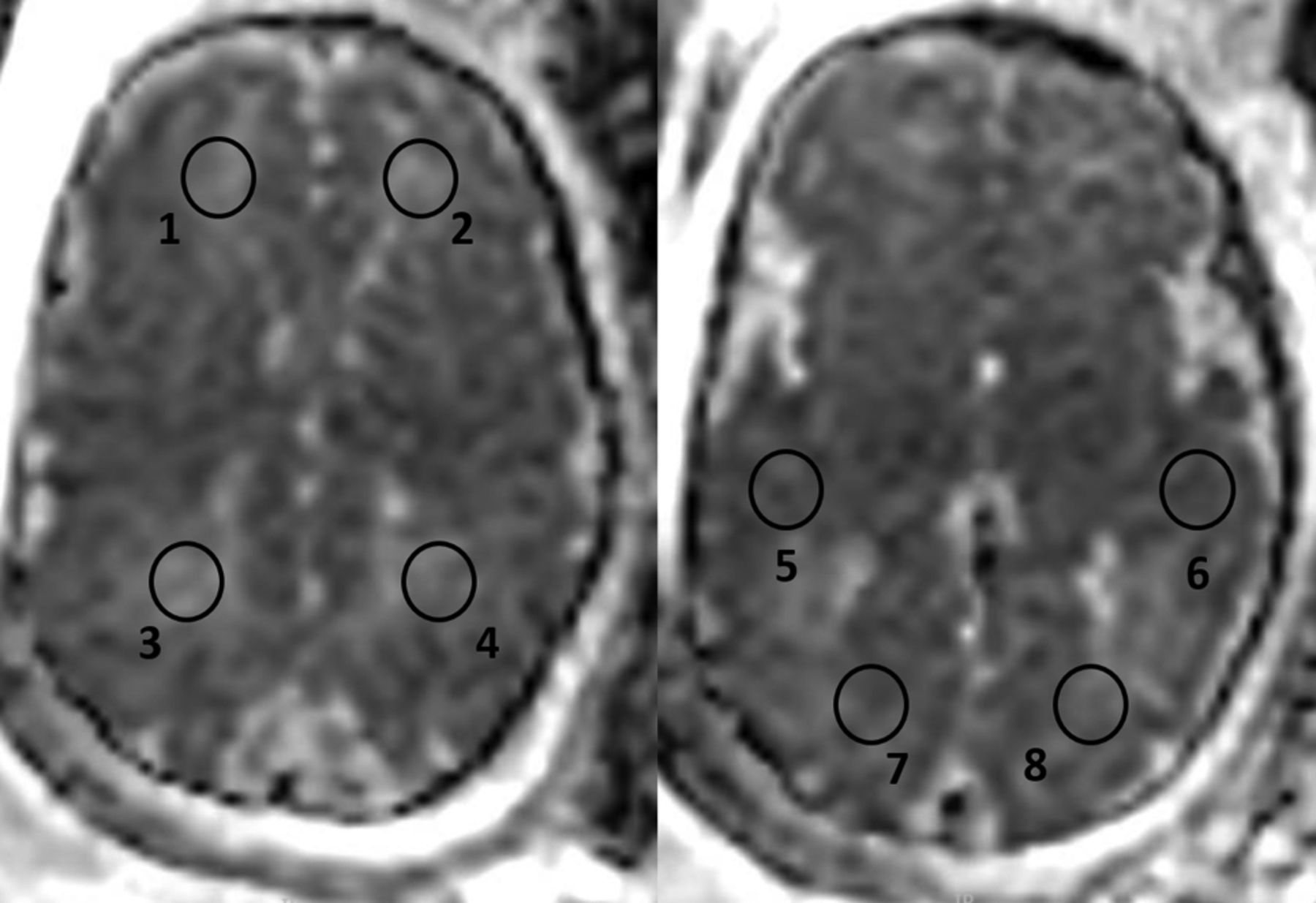
ADC calculation was performed on 8 circular ROIs: 2 on the white matter of both frontal, parietal, temporal, and occipital lobes. A circular ROI was used, placed over the desired anatomic area, ranging from 75 to 98 mm2, similar to that accepted in the recent literature.11 Examples of ROI placements over the various anatomic areas can be seen in Fig 1. The ROIs were placed with the following anatomic considerations: Frontal lobe ROIs were placed in the anterior part of the frontal lobes above the lateral ventricles, parietal lobe ROIs were placed in the posterior part of the parietal lobes above the lateral ventricles, temporal lobe ROIs were placed anterior to the temporal horns, and occipital lobe ROIs were placed posterior to the lateral ventricles. The ADC was calculated using IntelliSpace workstation software (Phillips Healthcare, Best, the Netherlands; https://www.usa.philips.com/healthcare/solutions/clinical-informatics/enterprise-imaging-pacs).

ADC calculation was performed on 8 circular ROIs: 2 on the white matter of both frontal (1, 2), parietal (3, 4), temporal (5, 6), and occipital lobes (7, 8). A circular ROI was placed over the desired anatomic area, ranging from 75 to 98 mm2.
White Matter T2 Hyperintense Signal
WMHS is a subjective interpretation of the signal from the fetal brain white matter on T2 sequences, made by the radiologist. This diagnosis is established when specific areas of the brain white matter appear hyperintense in comparison with other areas or with that expected according to the gestational age (Fig 2).16

T2 MR images (single-shot fast spin-echo T2-weighted sequences in 3 orthogonal planes using a half-Fourier technique, NEX = 0.53) of 2 fetuses at 33 weeks of gestational age. The CMV-positive fetus has diffuse WMHS (white arrowheads), unilateral ventriculomegaly, and intraventricular adhesions (black asterisks), suggesting ventriculitis (A–C). The CMV-negative fetus has WMHS located in the white matter in the temporal lobes (white arrowhead) (D–F).
Interobserver Validity of ADC Measurements
To validate the consistency of measurements and reliability of results, 2 observers evaluated 10 fetuses. Interobserver variability was assessed by the interclass correlation coefficient (ICC). We considered an ICC value of ≥0.8 as excellent agreement.
Neurodevelopmental and Hearing Outcome
Children were assessed by the Vineland Adaptive Behavior Scales, 2nd edition (VABS), which is a structured parent interview assessing 4 different domains of behavior: communication, daily living skills, socialization, and motor skills. All 4 domains are included in an adaptive composite score.17,18 VABS assessment was conducted by a phone interview by 2 medical students trained and supervised by a pediatric neurologist and child development expert experienced in conducting VABS (O.B.-Y.). Validation of the phone interviews were assessed by correlation of the ICC to the VABS scores of 15 children (divided into 7 and 8 children between the students) evaluated by the pediatric neurologist (O.B.-Y.). The ICC was >0.83 for the 4 VABS domains and the composite score. Scores of children were considered abnormal if the standard score was <70.
Hearing outcome was assessed 2–3 days after delivery by Transient Evoked Otoacoustic Emissions. Neonates positive for CMV were tested routinely before 1 month of age by brain stem auditory evoked potential, then at 3, 6, and 12 months by Transient Evoked Otoacoustic Emissions and behavioral assessment.
Statistical Analysis
Categoric variables were expressed as number and percentage. Distribution of continuous variables was assessed using a histogram and Q-Q plot. Continuous variables were described using median and interquartile range or mean and SD as appropriate. Categoric variables were compared using the χ2 test, Fisher exact test, or McNemar test as appropriate. Continuous variables were compared using the Student t test or Mann-Whitney test as appropriate. A 2-tailed P < .05 was considered statistically significant. Analyses were performed with SPSS (Version 24.0, 2016; IBM, Armonk, New York).
Results
Demographic and Clinical Characteristics of the Study Population
The study subjects comprised 43 singleton pregnant women and 1 single twins pregnant woman who underwent fbMRI scans. All 44 fetuses included in this study were in their third trimester of pregnancy at the time of the fetal MR imaging, with a median gestational age of 32 weeks (interquartile range, 28.25–35 weeks). The average maternal age was 33 years (interquartile range, 25–32 years). The indications for MR imaging included the following: maternal cytomegalovirus infection (n = 31), family history of central nervous system pathology (n = 3), and abnormal findings during fetal sonography (n = 10). The abnormal sonographic findings included the following: lateral ventricular asymmetry (n = 4), mega cisterna magna (n = 2), small head circumference (n = 2), fisted hands (n = 1), and hyperechogenic bowel (n = 1). Twenty-two (50%) of the fetuses were found to be positive for CMV by amniocentesis or by saliva or urinary CMV DNA testing after birth. Thus, to examine the association between ADC values and etiology, we divided the main study group into a CMV-positive group consisting of 22 fetuses with confirmed CMV infection and a CMV-negative group consisting of 22 fetuses with WMHS from an unknown etiology.
These 2 distinct patient populations are described separately and compared by their demographic, clinical, imaging, and neurodevelopment characteristics.
The median gestational age, pregnancy history, and sex did not differ statistically between the groups. All mothers in the CMV-positive group had normal medical background, compared with 6 (27%) mothers in the CMV-negative group who had significant abnormal medical background including thrombophilia, Raynaud disease, and a history of cerebellar infarction (P = .02).
In the CMV-positive group, there were significantly less early and late anatomic scan findings (P = .02, P = .009, respectively) (Table 1).
Demographic and clinical characteristics of fetuses with white matter T2 hyperintense signala
Distribution of Hyperintense Signal and Additional MR Imaging Findings
Both groups had similar rates of WMHS in the temporal lobe (P > .999). WMHS was not depicted in the occipital lobe in both groups. However, the CMV-positive group had statistically higher rates of parietal hyperintense signal (P = .002) and a trend toward higher rates in the frontal lobe (P = .067). The CMV-positive group had more extended WMHS involving all 3 lobes (P = .004). The CMV-negative fetuses had statistically significantly higher rates (P = .046) of minor additional findings on imaging, including subarachnoid cyst (n = 2), slightly enlarged subarachnoid space (n = 1), and lateral ventricle asymmetry (n = 4) (Table 2 and Fig 2).
Radiologic MR imaging findingsa
Interobserver Validity of ADC Measurements
ADC measurements showed excellent interobserver agreement for all regions, with the ICC ranging between 0.81 and 0.97.
ADC Value Measurements
ADC values for each group were compared with the normal ADC values as published by Hoffmann et al.11 Fetuses in the CMV-positive group were found to have statistically higher ADC values in the temporal lobe bilaterally (P = .002 and P < .001) and the left parietal lobe (P = .033) and a trend in the right parietal lobe (P = .057) (Table 3).
Comparison of ADC values of the study group with the control groupa
ADC values were compared for each region between the 2 study groups. Fetuses in the CMV-positive group were found to have higher ADC values in the left frontal lobe (P = .026), the parietal lobe bilaterally (right, P = .001; left, P = .002), and the temporal lobe bilaterally (right, P = .011; left, P = .002) (Table 4).
Comparison of ADC values between fetuses with CMV-positive infection and fetuses with isolated white matter hyperintense signala
Delivery Data, Hearing, and Neurodevelopmental Assessment
Neurodevelopmental assessment (VABS) and delivery data were analyzed for 20 children in the CMV-positive group and 18 children in the CMV-negative group (Table 5). Six patients (2 from the CMV-positive group and 4 from the CMV-negative group) refused to participate in the neurodevelopmental assessment. Delivery data and age at developmental assessment were not statistically different between the groups. Comparison of the VABS score for the 4 domains and the adaptive composite score showed only a trend for motor skills (P = .07). Four children in the CMV-positive group and 1 child in the CMV-negative group had at least 1 VABS score <70; however, this was not statistically significant. Only 1 child had a hearing deficit; this child was CMV-positive with a low VABS score.
Delivery data, hearing, and VABS assessmenta
Discussion
WMHS is a puzzling finding in fetal MR imaging, and its significance is not completely understood. The aims of our study were initially to explore the etiologies associated with this finding, then to examine whether the different etiologies are characterized by different ADC values, and, last, to investigate the association of WMHS with neurodevelopmental outcome.
Diverse etiologies were found to be associated with WMHS in this study. The major one (half of the study group), in accordance with fetal MR imaging literature, is congenital CMV infection.13,19,20 The precise etiologies of the second half of the group are not completely clear. Ten fetuses had further imaging findings; thus, the WMHS might be a different aspect of the overall brain pathology.
Comparison between the 2 groups demonstrated a difference in the distribution of the WMHS. Both groups had the same prevalence of WMHS in the temporal lobes, but the CMV-positive group had a higher rate in the parietal lobes and a trend in the frontal lobes. In general, the CMV-positive group had more diffuse WMHS.
The median ADC values were higher in the CMV-positive group than in the CMV-negative group in the temporal, parietal, and left frontal lobes. The ADC values of the CMV-negative group did not differ from those of the control group. Thus, although the incidences of WMHS were similar in the temporal lobes, the median ADC values were different. Because ADC is a quantitative measure and not a subjective interpretation, it is possible that some WMHS of the CMV-negative group is actually overinterpretation.
As for the CMV-positive group, the specific involvement of the temporal lobes was previously described in fbMRI. WMHS is part of a spectrum of findings localized to this area, including cysts, dilation of the temporal horns, and reduced temporal lobe volume.4,11,21,22 The reason for the specific vulnerability of the temporal lobe is unclear. Most interesting, in addition to the presence of WMHS in the temporal lobe, most of the fbMRIs in our study depicted a similar signal in the parietal lobe. This finding was previously described in children with congenital CMV.23⇓–25 Thus, the combination of temporal and parietal hyperintense T2 signal is potentially a sign of CMV infection involving the brain. Further involvement of WMHS including the frontal lobes may serve as an additional sign of congenital CMV infection.
The combination of WMHS and high ADC values in the CMV-positive group suggests a possible etiology for this finding. Hyperintense signal was associated at postmortem examination with astrogliosis and extracellular brain edema in the subacute stage of hypoxic-ischemic injury.2 Although hypoxic-ischemic injury pathogenesis is different from CMV infection, the simplest explanation of the T2 finding is an increase in extracellular fluid content in the white matter. Kotovich et al26 found low ADC values in fetuses with congenital CMV infection without T2 hyperintense signal. In a previous study of the same group, Yaniv et al4 described postmortem histology consisting of edema and cellular infiltration of plasma cells, lymphocytes, and microglia. The difference in T2 hyperintense signal and ADC values between the 2 latter studies and ours might reflect a different ratio between the edema and cellular component in the brain tissue. When the microgliosis and edema component are more prominent, the ADC values are larger than those of controls; whereas when the component of cellular degeneration and immune cell infiltration is more prominent, the ADC values are lower than those of controls.2,14,27⇓–29
The association between WMHS and abnormal neurodevelopmental outcome was not found in this study. In the CMV-positive group, 4 children (20%) had abnormal neurodevelopmental findings or hearing loss. Based on neurodevelopmental data from previous studies, the expected range of these abnormal findings in children with asymptomatic congenital CMV (normal prenatal imaging findings) is 10%–15%.30,31 Thus, it is difficult to assess whether the WMHS and the increased ADC values predict worse prognosis.
Combining the results from our study and others2,11⇓⇓–14,26 investigating the association of ADC and brain pathologies suggests the following practical advice for clinicians: The combination of WMHS and normal ADC suggests that the source of WMHS is most likely without clinical significance. As for cases of abnormal ADC either below or above the expected value for gestational age, they raise the suspicion of brain pathology such as CMV infection, ventriculomegaly, or ischemia. However, the association of abnormal ADC with neurodevelopmental outcome is unclear.
Our study is limited by the size of the study group. A larger number of patients could be used to correlate the distribution of T2 hyperintense signal or ADC values with neurodevelopment. On the other hand, the small number of children in each group strengthens the significance of the difference in T2 hyperintense signal and ADC values between the CMV-positive and -negative groups.
Conclusions
ADC measurements supported the validity of T2 hyperintense signal in fbMRI only in fetuses with CMV infection. The association of this finding with neurodevelopmental outcome requires further investigation.
Footnotes
E. Katorza and G. Strauss contributed equally to this work.
References
- Received February 26, 2018.
- Accepted after revision July 19, 2018.
- © 2018 by American Journal of Neuroradiology




{kind=link}
{kind=link}