
SUMMARY:
We describe 2 cases of a spinal cord lesion with imaging features closely resembling those described in supratentorial multinodular and vacuolating neuronal tumor (MVNT) or infratentorial multinodular and vacuolating posterior fossa lesions of unknown significance. Multiple well-delineated nonenhancing T2-hyperintense intramedullary cystic ovoid nodules were visualized within the white matter of the spinal cord, including some immediately abutting the gray matter. No alterations in signal intensity or morphology were detected in a follow-up. Moreover, no relevant clinical symptoms attributable to the lesions were present. We describe these lesions as presumed MVNT, and we therefore use the term MVNT-like spinal cord lesions.
ABBREVIATIONS:
- MVNT
- multinodular and vacuolating neuronal tumor
- MV-PLUS
- multinodular and vacuolating posterior fossa lesions of unknown significance
- UC
- ulcerative colitis
A multinodular and vacuolating neuronal tumor (MVNT) is a fairly new and distinctive entity in the 5th edition of the World Health Organization classification of central nervous system tumors.1 It was first described in 2013 by Huse et al2, who showed a case series of benign seizure-associated intra-axial lesions. Imaging features on MR imaging include clusters of multiple well-delineated T2-hyperintense millimetric ovoid nodules subcortically in the white matter (ie, a “bubbly appearance”), which can also be found juxtacortically. The gray matter is generally not affected. Classically, there is no contrast enhancement, no diffusion restriction, and no signal loss on FLAIR sequences. Cerebral MVNT is described as a “leave me alone” lesion. The microscopic appearance of a MVNT consists of immature neuroepithelial cells organized in nodules with a prominent vacuolating matrix3 that is almost pathognomonic.
CASE SERIES
Case 1
A 45-year-old woman presented with right-sided cervicobrachialgia for several weeks. Except for discrete paresthesias in the right thumb and index finger, no neurologic symptoms were present. There was no relevant medical history.
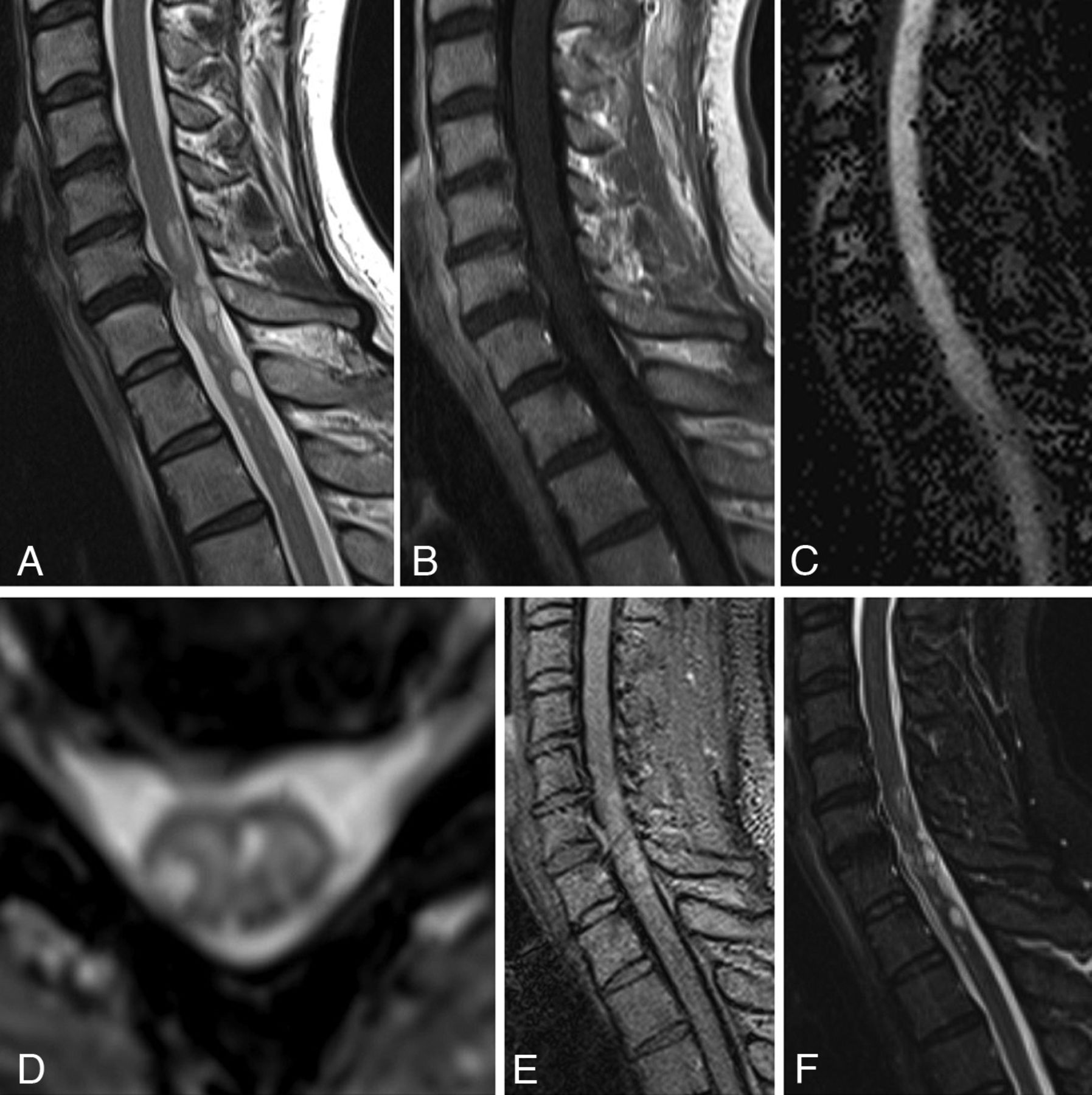
Alongside a disk extrusion and degenerative uncovertebral changes on the right, MR imaging showed a large multilocular intradural intramedullary lesion, consisting of multiple well-defined homogeneous T2-hyperintense and T1-hypointense cystic-like changes, at the cervicothoracic junction (C5–T2) (Fig 1). These cystic-like changes were located in the white matter of the spinal cord, including some immediately abutting the gray matter. There was no contrast enhancement and no diffusion restriction. No perilesional signal changes were detected. Follow-up MR imaging after 12 months showed no volume and/or signal intensity changes of the lesion. To exclude intracranial pathology, an MR imaging examination of the brain was performed, and it showed no abnormalities. All lab values, including infectious serology, were normal.

Case 1; 45-year-old woman A, Sagittal TSE T2-weighted image shows a multilocular intradural intramedullary lesion. There are multiple cystic-like changes within the spinal cord at different levels of the cervicothoracic junction. Note that there is neither syringomyelia nor T2-hypointense changes within the medulla. A cervical disk extrusion at C6–C7 can also be seen. B, Sagittal TSE T1-weighted image after the intravenous administration of gadolinium. No contrast enhancement can be seen. C, Sagittal echo-planar diffusion-weighted image shows no diffusion restriction within the lesion. D, Para-axial gradient recalled-echo T2-weighted image depicts the cystic-like intra-axial lesion. Note the sharp delineation of the lesions without perilesional edema. These lesions are located within the white matter of the spinal cord, without affecting the gray matter. E, Sagittal FLAIR T2-weighted image shows the T2-hyperintense lesion. Unlike perivascular spaces (also called Virchow-Robin spaces), there is no signal loss on FLAIR. F, Sagittal short tau inversion recovery T2-weighted image from a 12-month follow-up. No alterations in signal intensity or morphology were detected. Stable lesion.
Case 2
A 37-year-old woman with a history of BRCA1 carrier status and ulcerative colitis (UC) presented with approximately 9 months of chronic headache. She reported that the headaches began following an intrauterine fetal demise in the setting of a UC flare, complicated by retained products of conception, requiring dilatation and curettage. She reported a dull, nonlocalizable headache that was a 2/10 in severity but denied other neurologic symptoms.
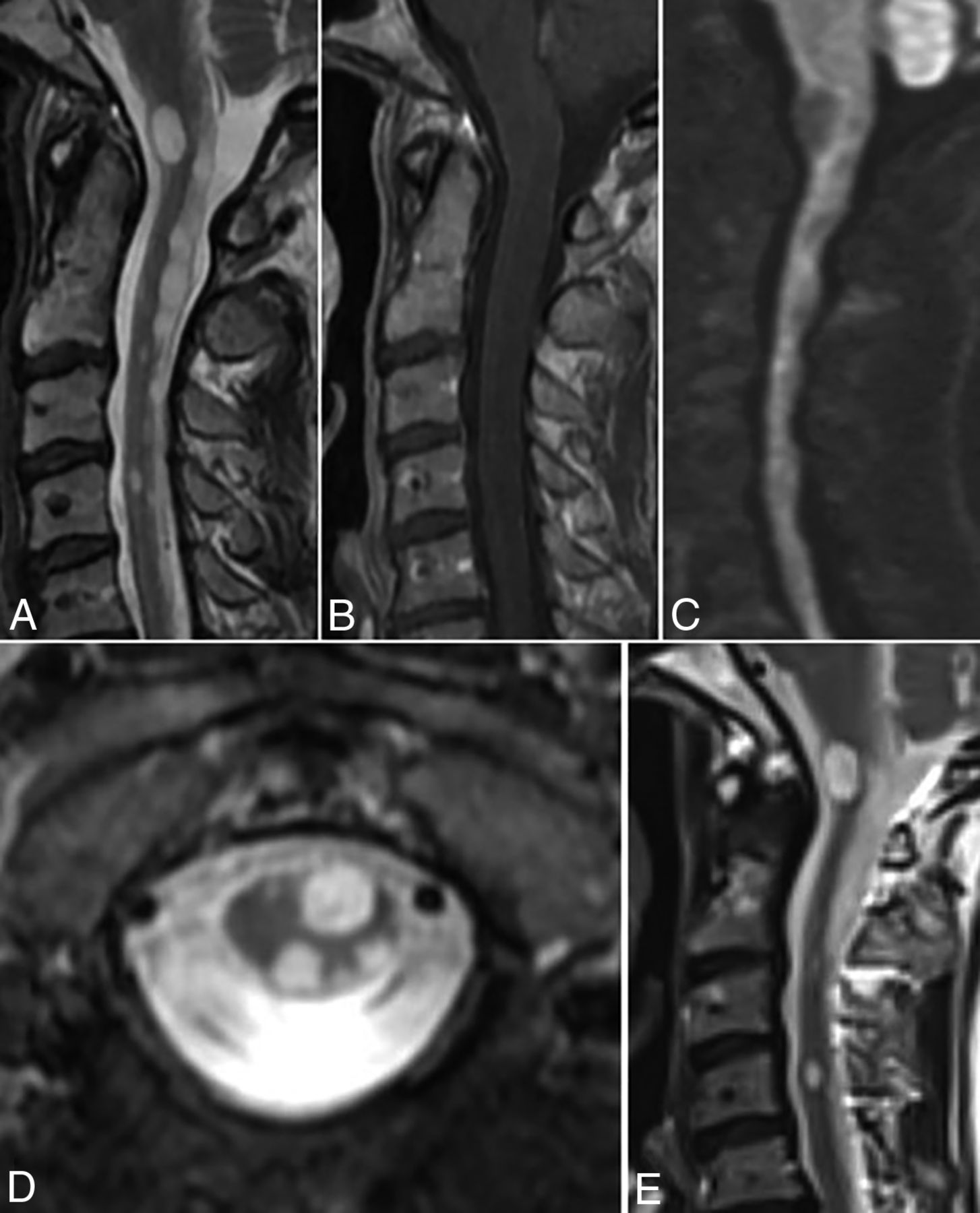
For a work-up of her headaches, she was referred for MR imaging of the head, which revealed numerous well-demarcated, nonenhancing T2-hyperintense cystic-like lesions in the medulla and visualized upper cervical spinal cord. Subsequent dedicated spine MR imaging revealed the extent of these intramedullary lesions within the cervical spinal cord, down to the C4 level (Fig 2). Follow-up imaging over the next 4 years remained stable, without the development of clinical symptoms. The laboratory values and infectious work-up were unrevealing. CSF sampling revealed mildly elevated protein but was otherwise normal.

Case 2; 37-year-old woman A, Sagittal TSE T2-weighted image shows multilocular intradural intramedullary lesions. Similar to case 1, there was neither syringomyelia nor any T2-hypointense changes within the medulla. B, Sagittal T1-weighted image after the intravenous administration of gadolinium. No contrast enhancement can be seen. C, Sagittal echo-planar diffusion-weighted image shows no diffusion restriction within the lesions. D, Para-axial T2-weighted image depicts the cystic-like intra-axial lesions. Note the sharp delineation of the lesions. These lesions are located within the white matter of the spinal cord, without affecting the gray matter. E, Sagittal T2-weighted image from a 4-year follow-up MR-examination. No volume changes and/or signal intensity changes could be detected, allowing for differences in the field of view.
DISCUSSION
In our cases, we see lesions that include a cluster of multiple well-delineated T2-hyperintense millimetric ovoid nodules in the spinal cord white matter, some immediately next to the gray matter. All imaging characteristics are exactly as described in MVNT. Moreover, the lesions did not present any clinical symptoms and did not change on follow-up. Therefore, we describe these lesions as MVNT-like spinal cord lesions.
We present 2 cases of cervical multilocular intradural intramedullary lesions. The differential diagnosis includes neoplastic, inflammatory, vascular, or infectious lesions. Neoplasms, such as glioma, ependymoma, hemangioblastoma, metastasis, and diffuse leptomeningeal glioneuronal tumors have a different morphology and generally show contrast enhancement. Because of its similar T1-signal and T2-signal characteristics, spinal cord subependymoma should also be considered. Spinal subependymomas tend to present as diffuse T2-hyperintense lesions with cord enlargement and possibly some enhancement. As they arise from subependymal glial cells, these lesions are typically centrally located in the spinal cord, rather than being peripheral. The lesions are larger than the typical “cysts” seen in MVNT, and they have a lower signal intensity compared with CSF. In MVNT and in our cases, cystic portions are isointense on T1-weighted and T2-weighted images. Various neurologic symptoms have been described in patients with spinal cord subependymoma, but they can also be asymptomatic. Infectious diseases, such as cryptococcosis and echinococcosis may also be considered; however, all lab values were negative. Further, there were no clinical signs of infection and the lesions did not show any enhancement. Inflammatory disorders of the cervical spinal cord with T2-hyperintense lesions mainly consist of multiple sclerosis, neuromyelitis optica, and acute disseminated encephalomyelitis. Neither lesion showed any change on follow-up examinations, and there were no clinical symptoms or laboratory findings attributable to either of the lesions. Vascular pathology (eg, vasculitis) may mimic this imaging presentation. However, lesions associated with vasculitis usually show contrast enhancement and may be irregularly delineated. Perivascular spaces, also called Virchow-Robin spaces, are also included in the differential diagnosis of a cerebral MVNT, but dilated perivascular spaces in the spinal cord have only been reported on microscopy and not on MR imaging.
In the literature, MVNT was originally exclusively described within the cerebrum. Early case series reported that MVNT occurs supratentorially in all lobes,3 and a recent publication has shown that these benign lesions do not change over long-term follow-ups.4 Lesions, although originally associated with seizures, are often asymptomatic, incidental findings.5,6 Recent publications have also demonstrated cystic multinodular lesions infratentorially in the posterior fossa, with imaging characteristics compatible with MVNT.7⇓-9 These were reported within the cerebellar hemispheres and vermis. None were histologically proved. The term multinodular and vacuolating posterior fossa lesions of unknown significance (MV-PLUS) was proposed.7
No case reports were found describing MVNT in the spinal cord. However, the imaging features of these lesions in our patients and the stable findings on follow-up MR imaging were MVNT-like lesions. It is reasonable to hypothesize that MVNTs can also occur within the spinal cord, as they may also occur in the posterior fossa. Short-term follow-up is a limitation of this case report. There was a follow-up period of 12 months in case 1 and a 4-year follow-up in case 2. Also, because of the asymptomatic characteristics of the lesions in combination with their locations in the spinal cord, no histopathologic confirmation was obtained. However, other publications regarding MV-PLUS also have no histopathological confirmation.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received October 18, 2023.
- Accepted after revision December 5, 2023.
- © 2024 by American Journal of Neuroradiology





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.