
Abstract
BACKGROUND AND PURPOSE: The current reference standard of diagnosis for peripheral trigeminal neuropathies (PTN) is clinical neurosensory testing (NST). MR neurography (MRN) is useful for PTN injury diagnosis, but it has only been studied in small case series. The aim of this study was to evaluate the agreement of Sunderland grades of nerve injury on MRN and NST by using surgical findings and final diagnoses as reference standards.
MATERIALS AND METHODS: A total of 297 patient records with a chief complaint of PTN neuralgia were identified from the university database, and 70 patients with confirmed NST and MRN findings who underwent surgical nerve repair were included in the analysis. Cohen weighted kappa was used to calculate the strength of the agreement between the 3 modalities.
RESULTS: There were 19 men and 51 women, with a mean age of 39.6 years and a standard deviation of 16.9 years. Most (51/70, 73%) injuries resulted from tooth extractions and implants. MRN injury grades agreed with surgical findings in 84.09% (37/44) of cases, and NST injury grades agreed with surgical findings in 74.19% (23/31) of cases. MRN and NST both showed similar agreement with surgery for grades I to III (70% and 71.43%). However, MRN showed a higher rate of agreement with surgery (88.24%) for injury grades IV and V than did NST (75%).
CONCLUSIONS: MRN can objectively improve preoperative planning in patients with higher-grade nerve injuries.
ABBREVIATIONS:
- IAN
- inferior alveolar nerve
- LN
- lingual nerve
- MRN
- MR neurography
- NST
- neurosensory testing
- PTN
- peripheral trigeminal neuropathy
Peripheral trigeminal neuropathy (PTN) can be caused by an injury of the trigeminal nerve or its branches, specifically the inferior alveolar nerve (IAN) and lingual nerve (LN). These injuries can cause a loss of sensation to the lower face and oral cavity, an altered or absent taste sensation of the anterior two-thirds of the tongue due to damage to the chorda tympani fibers that travel with the lingual nerve, and neuropathic pain in the trigeminal nerve distribution.1⇓-3 Common etiologies of PTN include iatrogenic dentoalveolar surgeries, injection injuries, and trauma, with third molar extraction being the most common cause. With up to 10 million third molar removals occurring each year and an incidence of permanent paresthesia of the lip, tongue, or cheek ranging from 11,500 to 35,000 a year, PTN cause substantial morbidity and can result in significant reductions in quality of life.4⇓-6
The current diagnostic reference standard for PTN injuries is clinical neurosensory testing (NST), which compares a patient’s pressure and pain sensation in a nerve distribution with that of an expected normal. NST incorporates 3 domains: spatiotemporal sensory perception, monofilament contact detection, and pain tolerance and thresholds.7 The 5 scores of sensory impairment denote a normal, mild, moderate, severe, or complete loss of function.8 The results from NST, in combination with clinical history and examination findings, are used to determine proper treatment methods based on the Sunderland classification system. The Sunderland classification system defines the nerve injury in 5 grades, ranging from minor injury to complete nerve transection.9,10 Higher-grade injuries require timely and accurate interventions to maximize the possibility of the regeneration of axons. However, NST poses various limitations, including decreased test result reliability within the first 3 months following an injury, the subjectivity of patient responses, and substantial intra observer and inter observer variability.7,11 In addition, being an indirect test, NST cannot show nerve anatomy or lesions. As a result of these limitations, NST may lead to an inaccurate analysis of nerve damage severity and may delay the treatment of more severe nerve injuries that require timely surgical repair to improve a patient’s prognosis. Thus, the delays can result in otherwise preventable permanent nerve damage with substantial morbidity.
MR neurography (MRN) is an imaging technique that provides a noninvasive method by which to delineate the neuromuscular anatomy and intraneural architecture of peripheral nerves in multiple orthogonal planes.12⇓-14 Specifically, it has been validated for use in PTN and in the identification of the different Sunderland grades of injuries.7,10,12 Thus, MRN has the advantage of showing both nerve lesions for presurgical planning and the grade of severity of an injury.
Current literature that evaluates the role of MRN for the diagnosis and management of PTN in patients has been limited to small sample sizes, and its value over NST has not been studied in sufficient detail. The aim of this study was to evaluate the agreement of Sunderland grades of nerve injury on MRN and NST by using surgical findings and the final clinical diagnosis as the reference standards in a larger, consecutive patient cohort. We hypothesized that the reported MRN injury grade agreed with surgical findings in a higher percentage of cases than did NST. As a secondary aim, we also evaluated the agreement between MRN-assigned and NST-assigned nerve injury grades.
MATERIALS AND METHODS
An Institutional Review Board approved this retrospective cross-sectional study, and informed consent was waived.
Patient Demographics and Injury Classification
A consecutive group of 297 adults of all genders with a suspected injury of PTN were queried from an institutional database over a 6-year period (July 2015 to November 2021). All patients were referred from the institutional oral and maxillofacial surgery clinic. These patients were all seen at the institution by an experienced maxillofacial surgeon and had trigeminal MRN imaging that was interpreted by an experienced radiologist. Seventy patients from the initial cohort had surgery, NST, and MRN, and these patients were included in the final sample.
Clinical and Surgical Classification
The NST was performed by the same oral and maxillofacial surgeon (J.R..Z., with 30 years of experience) and the Sunderland class grades were reported in the medical charts based on clinical findings and NST. The 70 patients who underwent surgery were also graded intraoperatively by using the Sunderland classification criteria in Table 1. The NST parameters are described in Table 2. The final diagnoses with injury grades, based on surgical and histopathology findings, were reported in the patients’ charts and served as the reference standards for both MRN and NST.
Sunderland nerve injury classification with corresponding surgical findings, MRN findings, and surgical indications
NST parameters. Present values exhibit comparable sensitivity within the normative range. Failed values are less than those of the control sites or the normative range. Elevated values are greater than those of the control sites. Absent values are greater than the maximum of the testing device
MRN Imaging and Reports
Seventy patients underwent MRN imaging by using a standardized institutional protocol (Table 3). Sixty-two patients had MRN on 3T scanners, and 8 patients had MRN on 1.5T scanners. The same imaging sequences and similar parameters were used on both types of scanners (Ingenia, Achieva, Philips; Avanto, Siemens). Most scans were noncontrast scans (90%, 63/70). 1.5T was used in the setting of dental hardware in a small minority of cases. The protocol was longer on the 1.5T scanners than on the 3T scanners by 15 minutes, overall. Otherwise, the image quality was similar, except for less-than-optimal fat suppression on 3D MR imaging and a less ideal demonstration of the lingual nerve on 1.5T. We prefer 3T scanners for most cases because of the time efficiency and better fat suppression on 3D imaging. Contrast scans do not make any difference in nerve evaluation, as the injured nerves do not enhance in our experience. It was a referring doctor’s preference to obtain a few scans with contrast imaging. The MRN reports were generated by an experienced radiologist (A.C., 15 years of postfellowship experience and 14 years of MRN-reading experience) as the standard of care, and injury grades were placed in the reports prospectively, based on imaging and a review of patient history (duration after injury, distribution of pain to cheek or tongue, paresthesia, taste changes, etc), independent of the NST score.
Institutional protocol for MRN imaging
Data Analysis
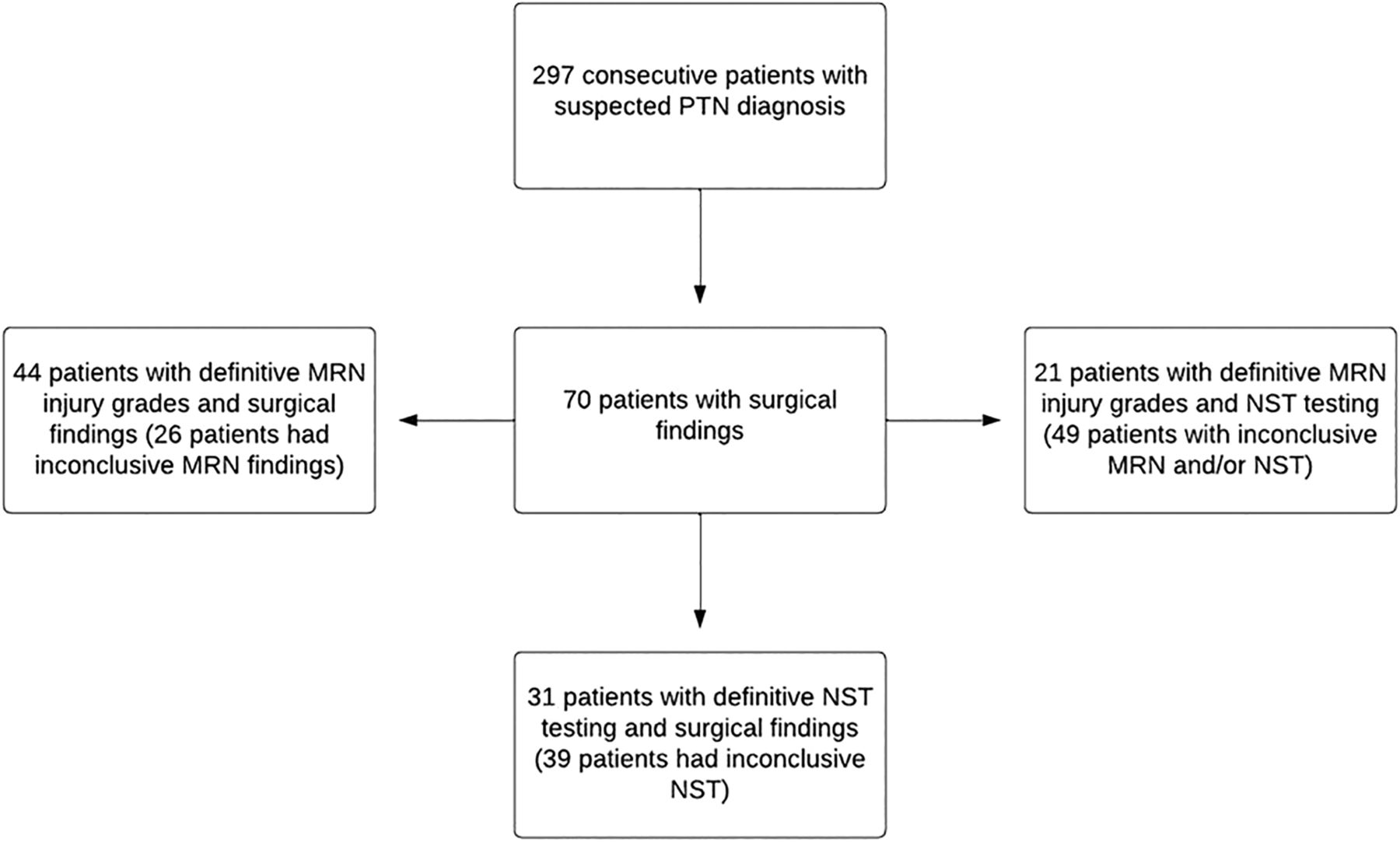
The medical charts were reviewed by 3 medical students. All charts were data mined to identify the Sunderland injury class on NST and MRN, previous surgeries, surgical findings, whether surgery was performed after the MRN, and surgical pathology results. The Sunderland classification system of nerve injury is described in detail in Table 1. Of the cohort, 70 patients had surgery. In the surgical cohort, not all patients had definitive MRN and NST injury grades in their charts. For example, inconclusive results included patients whose injury grades could not be definitively classified into a single grade. Thus, when doing the statistical analysis, inconclusive results were not included (Fig 1).

The 3 groups from the main cohort of 70 surgical patients were included in the statistical analysis. Because patients had inconclusive results in different modalities, the 3 groups had different sizes. For example, the 44 patients in the MRN versus surgical findings cohort were derived from the original 70 patients because 26 patients in the 70-patient surgical cohort had inconclusive MRN findings.
Statistical Analysis
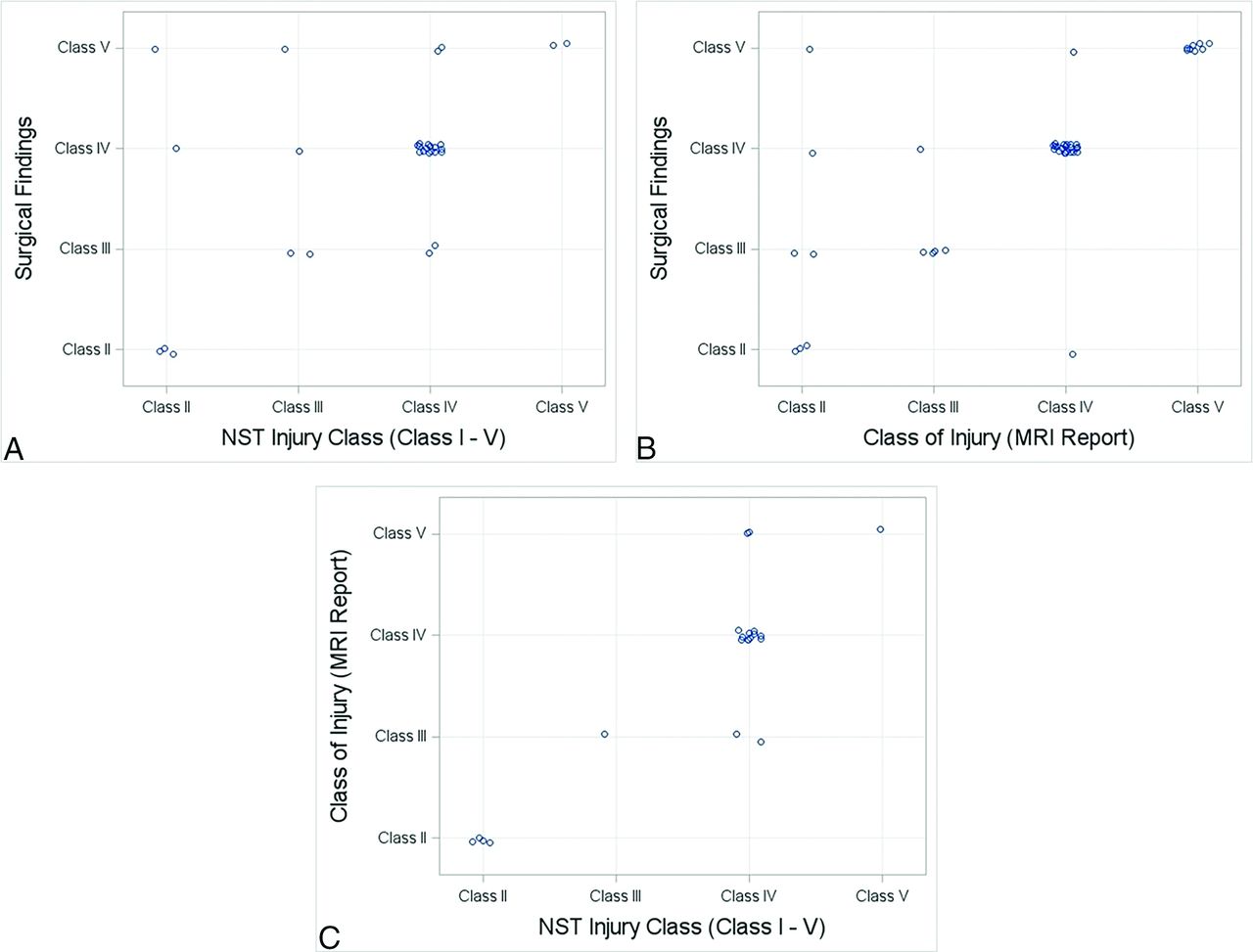
Descriptive statistics were used for the demographic data and nerve injury classifications on NST and MRN. The agreement of NST and MR imaging was obtained, using surgical and histopathology findings as reference standards. Cohen weighted kappa was also calculated. The distribution of injury classes by NST, MRN, and surgical findings can be found in Figure 2. The agreement coefficient interpretations used were as follows: Excellent Agreement: 0.75–1.00, Good Agreement: 0.60–0.75, Fair Agreement: 0.40–0.60, Poor Agreement: < 0.40.15

Jitter plots showing injury class distributions for (A) NST versus surgery, (B) MRN versus surgery, and (C) NST versus MRN.
RESULTS
Patients
Seventy patients underwent surgical repair. The study cohort consisted of 19 (27%) men and 51 (73%) women with a mean age of 39.6 years and a standard deviation of 16.9 years. Most (51/70, 73%) injuries resulted from tooth extractions and implants, with other injuries including motor vehicle crashes, sinus surgery, and mandibular bone grafting. Table 4 contains the breakdown of injury grades for NST, MRN, and surgical findings among the 70 patients. Of the 70 patients, 44 had LN injuries, 15 had IAN injuries, 5 had both IAN and LN injuries, and 6 had maxillary nerve injuries. The mean time from MRN to surgery was 87 days, with a standard deviation of 141 days.
Distribution of injury grades for NST, MRN, and surgical findings among the 70 patients. Inconclusive results mean that the injury grade was unable to be narrowed down to just 1 class. For example, a grade of II/III being reported in the patient chart is recorded as inconclusive
NST, MRN, and Surgical Correlations
The study found that NST showed fair agreement with surgical findings, whereas MRN exhibited good to excellent agreement with surgical findings. Overall, NST and MRN had excellent agreement with each other.
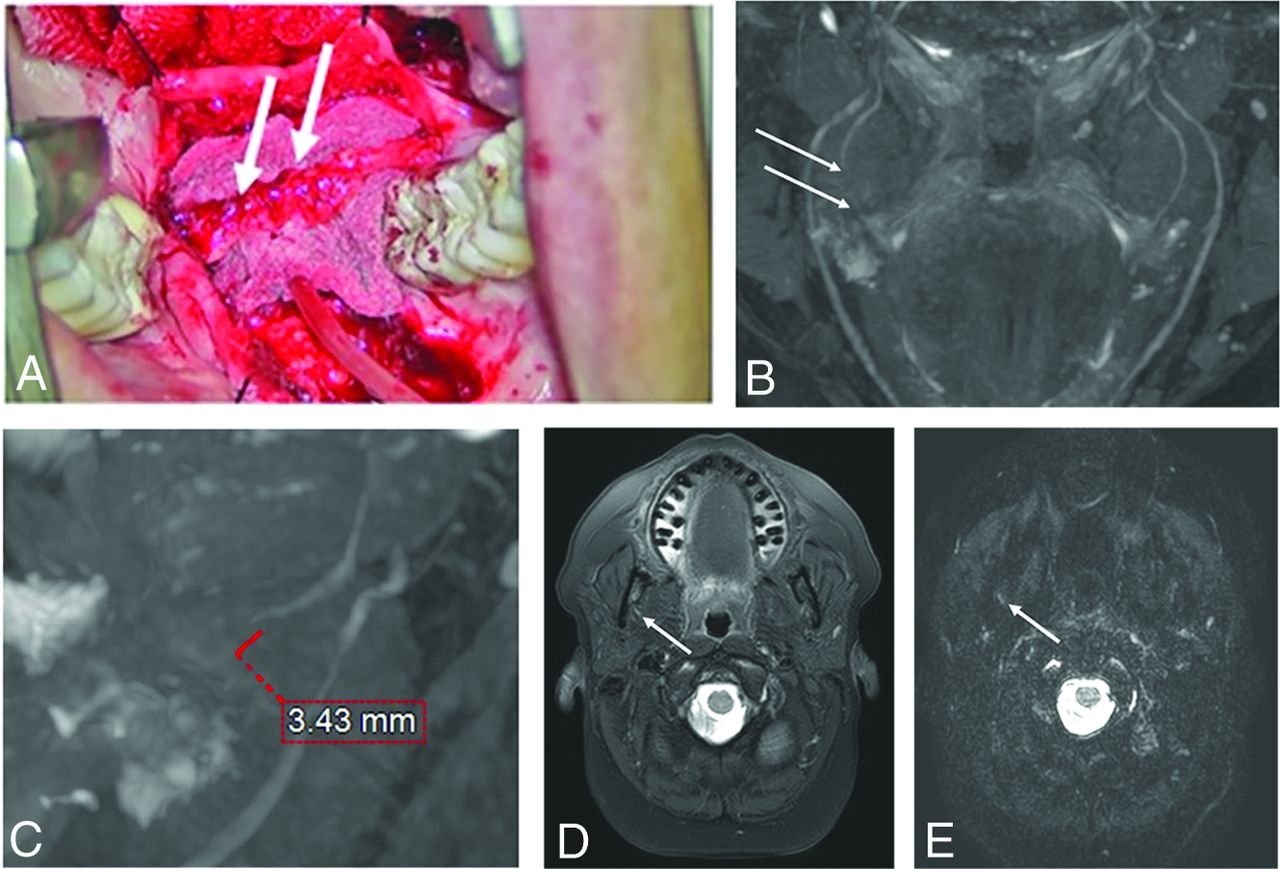
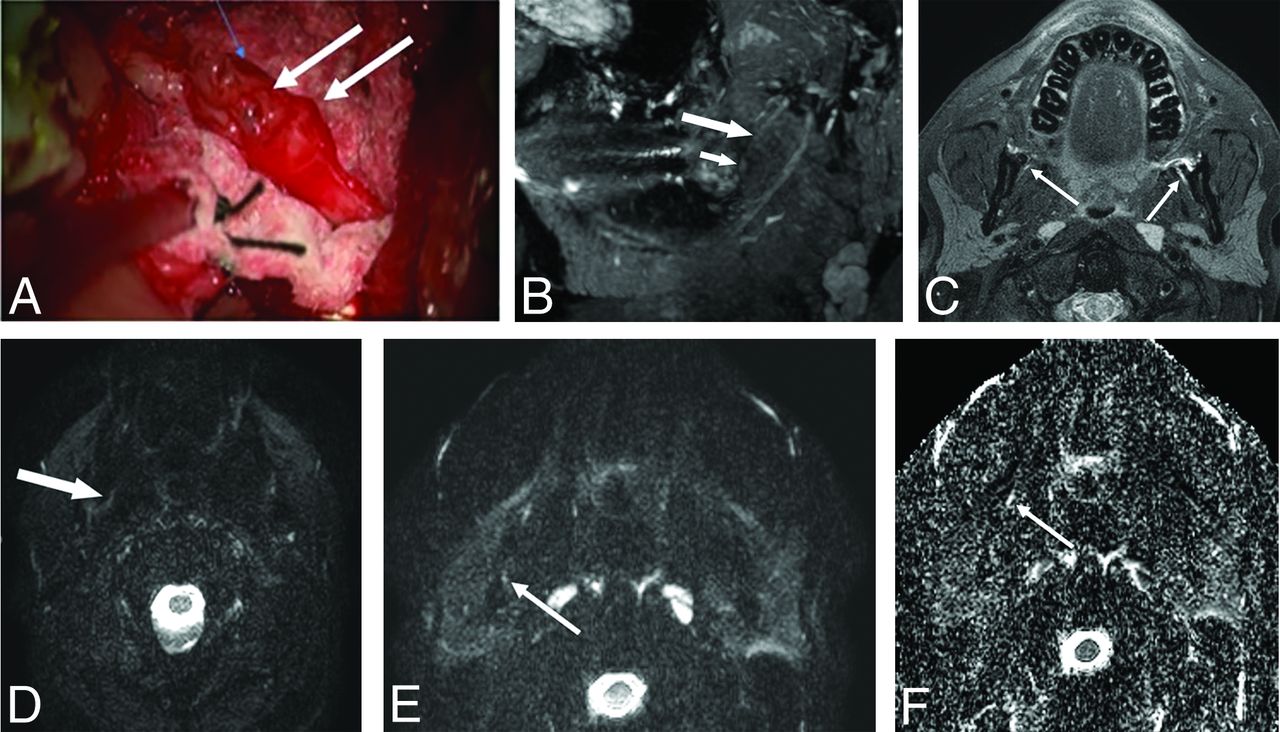
The study found that the MRN Sunderland injury grades agreed with surgical findings 84% (37/44 cases) of the time, whereas NST injury grades agreed with surgical findings 74% (23/31 cases) of the time. The weighted kappa values with 95% CI for the comparisons of each pair of techniques can be seen in Table 5. Figure 3 shows a case in which the NST did not agree with surgical findings but the MRN did. Figure 4 shows a case in which the NST was inconclusive, but the MRN agreed with surgical findings. Figure 5 shows a case in which all 3 modalities agreed. The MRN and NST injury grades agreed 81% of the time (17/21 cases).

A 46-year-old woman with an injury to the right lingual nerve from molar teeth extraction. The NST yielded an injury grade of IV, but MRN yielded an injury grade of V, consistent with the surgical findings of a class V injury with amputation neuroma and a fibrous connection to the distal end. A, Intraoperative picture with amputation neuroma and foreign material highlighted by arrows. B, Coronal 3D PSIF MRN image of the lower face with arrows pointing to a gap in the right lingual nerve. C, Sagittal 3D PSIF MRN image reconstruction showing the neural gap in more detail, measuring 3.43 mm. D, Axial T2 SPAIR and (E) axial DTI showing the abnormal right lingual nerve (arrows). The nerve gap is best seen on 3D MRN images. PSIF indicates reversed fast imaging in steady state free precession; SPAIR, spectral attenuated inversion recovery.

A 33-year-old man with bilateral injuries to the lingual nerves caused by a third molar extraction. The NST was inconclusive, but MRN revealed a Sunderland grade IV injury, consistent with surgical findings. A, Intraoperative picture of the left lingual nerve showing a neuroma in continuity. B, 3D PSIF sagittal reconstructed 3D MRN image showing the focal nerve swelling (small arrow) in the abnormal nerve (large arrow) as a neuroma in continuity. C, Corresponding axial T2 SPAIR image showing abnormally hyperintense and enlarged lingual nerves bilaterally (arrows). D and E, Axial DTI and (F) axial ADC images showing the abnormally hyperintense right lingual nerve (arrows) with nonvisualization of the left lingual nerve on DTI and ADC images. PSIF indicates reversed fast imaging in steady state free precession; SPAIR, spectral attenuated inversion recovery.

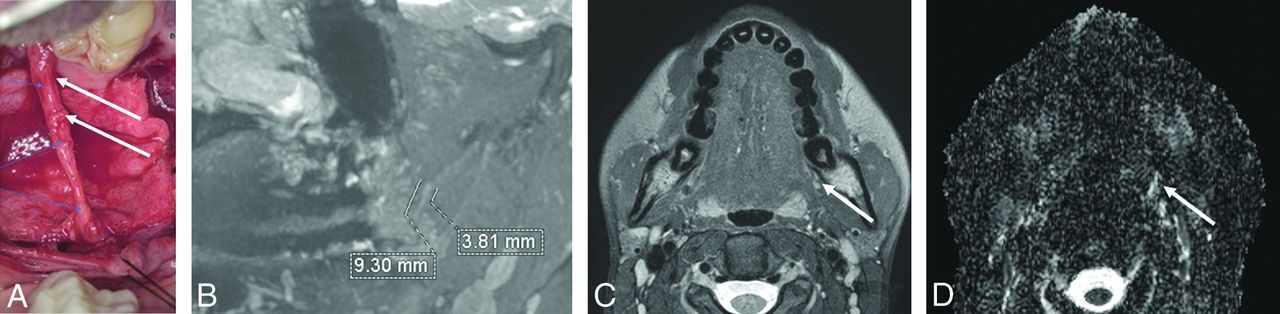
A 23-year-old woman with an injury to the right lingual nerve caused by a third molar extraction. Both MRN and NST revealed a Sunderland grade IV injury, consistent with surgical findings. A, Intraoperative picture showing neuroma in continuity. B, 3D PSIF sagittal reconstructed MRN image of the lower face showing a neuroma in continuity of 3.81 mm with a 9.3 mm overall abnormal hyperintense nerve. C, Focal nerve swelling can be appreciated in an axial T2-weighted SPAIR image and (D) the corresponding DTI, as outlined by the arrows. PSIF indicates reversed fast imaging in steady state free precession; SPAIR, spectral attenuated inversion recovery.
Weighted Cohens kappa with 95% CIs for the NST grade versus MRN, surgical findings versus MRN, and surgical findings versus NST
Sunderland injury grades of I through III have better prognoses and may not be treated surgically unless either persistent pain exists or extensive surrounding scarring causes nerve entrapment. Sunderland injury grades of IV and V show worse prognoses unless treated timely with surgery.9 Thus, the study also analyzed the rates of agreement for NST and MRN in these 2 overarching injury categories. MRN and NST had similar rates of agreement with surgical findings for Sunderland injury classes I to III (70% for MRN, 71.43% for NST). However, MRN showed a moderately higher rate of agreement with surgical findings (88.24%) for Sunderland injury grades IV and V, compared with NST findings (75%). Detailed statistics can be found in Table 6. Table 1 contains a more detailed explanation of the Sunderland injury classifications as well as their respective surgical indications and radiologic findings.
Agreement percentages for all modalities
DISCUSSION
Peripheral nerve injury is one of the most common causes of chronic neuropathic pain, contributing to significant disease burden.16 The most common cause of PTN results from molar tooth extractions, resulting in facial and jaw pain or paresthesia.17 In PTN, early diagnosis and timely management are essential for improved patient outcomes and prognosis, with outcomes deteriorating due to older age, delayed treatment, and a larger nerve gap.18
The current standard for diagnosing PTN by using NST is limited, as the subjectivity of the results delays the treatment of higher-class injuries, resulting in potentially irreversible nerve damage. MRN provides an alternative method for the diagnosis and staging of patients with PTN because of its ability to delineate anatomy and the exact location of injury for preoperative planning.8
Similar to previous studies, this study establishes that MRN can accurately diagnose patients with PTN, with localization of the nerve lesion. Though previous literature has demonstrated the viability of MRN in the diagnosis of patients with PTN, sample sizes were small, and surgical findings were not systematically examined. This study expands on current literature by examining the correlations between injury grading based on NST and MRN, using surgical and histopathology findings as reference standards. This study found that though NST and MRN had similar rates of agreement with surgical findings in lower-grade injuries, MRN had higher rates of agreement with surgical findings than did NST in higher-grade injuries. MRN also yielded smaller confidence intervals than did NST. Because NST is subjective, responses can be similar in different grades of nerve injury due to various factors, such as delayed or exaggerated sensory responses, psychological issues, and secondary gain. However, MRN displays a more objective anatomy of the nerve and injury. Thus, MRN can be a useful tool for the staging of patients with PTN, especially patients with higher-grade injuries for whom timely intervention is crucial in lowering the risk of irreversible nerve damage. It should also be noted that the NST was performed by the same surgeon, who had extensive experience with NST. While it takes years of experience and clinical skills to establish such acumen, MRN is more widely available and is not dependent on subjective patient information about pain and pressure sensitivity. Though a strength of the study was having MRN interpretations done by an experienced reader who prospectively assigned the injury grades, this may limit generalizability. However, MRN is increasingly becoming widely available, as higher Tesla strengths are being incorporated into clinical practices and 3D MR imaging protocols have been standardized.
This study has some limitations. The patients in the cohort had symptomatic PTN that warranted referral to the university maxillofacial clinic, resulting in a cohort that had higher degrees of nerve injuries, overall. However, there were 24/70 class II and III injuries available, as well. Additionally, not all patients underwent surgery, and the same surgeon who documented the NST results performed the final surgeries. Furthermore, some patients had inconclusive results on MRN and NST such that a definitive injury class could not be determined between class II or III. This decreased the size of the cohort that could be examined. It was also a learning experience for the MRN reader, as the imaging knowledge from other, larger peripheral nerves was being transferred to the smaller jaw nerves. It is expected that future correlations might even be improved with consistent and improved imaging on the newer scanners. We also did not reevaluate the MRN scans, as doing so would have led to results that differed from the prospectively determined MRN grades of injury and would have compromised the first approximation that we wanted to derive about the MRN-NST-surgery correlation data that was intended with this institutional audit of the utility of MRN. The full utility of MRN would be best demonstrated in future prospective studies with the possible randomization of patient groups. Furthermore, there was possible bias in the evaluation of the NST grades, as only 1 surgeon evaluated the NST gradings. Likewise, because only 1 radiologist read the MRN and generated the final reports, there could be bias and errors on the assignment of the Sunderland grading scale on the MRN. However, the radiologist is experienced with reading MRN (14 years), and the possibility of misclassifying injuries on MRN is slim.
Because the MR imaging and NST grades agreed well, the noninferiority of results may encourage surgeons to use MRN more in their practices. Future related studies could examine the utilization of MRN in the evaluation of PTN in the preoperative and postoperative periods as well as whether the utilization of MRN led to better patient outcomes in patients who underwent surgery.
CONCLUSIONS
This study demonstrates that MRN-derived peripheral trigeminal nerve injury grades correlate with intraoperative findings in patients with higher-grade nerve injuries better than do NST-derived grades. This finding supports MRN as an important tool for the diagnosis and clinical management of patients with PTN. With a timely diagnosis of higher-grade injuries, it can result in potentially lower times to intervention and can thereby impact patient outcomes.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received June 30, 2023.
- Accepted after revision December 2, 2023.
- © 2024 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.