
Article Figures & Data
Figures
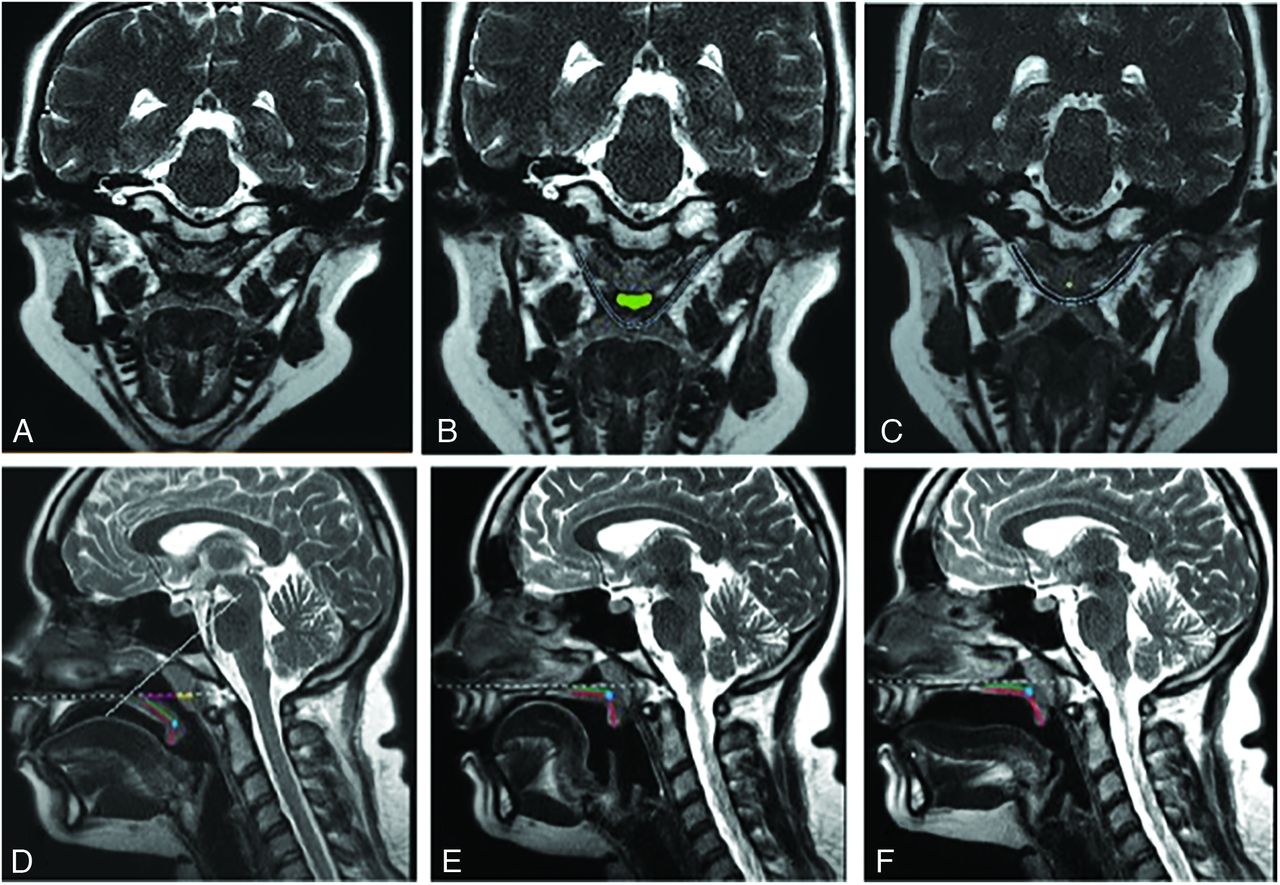
- FIGURE.
A, Coronal oblique T2 image along the plane of the LVP (blue outline, B and C) at the level of the velopharyngeal port during rest. The normal appearance of the LVP is T2-hypointense and intact along its length. B, Coronal oblique T2 with the velopharyngeal port appropriately open (green outline). C, Coronal oblique T2 during phonation with the velopharyngeal port appropriately closed. D, Sagittal midline T2 image through the head at rest showing the 50–60° coronal oblique plane (solid white line), effective length (green line), the total velar length (red line), and the palatal plane (dotted line). E and F, Sagittal midline T2 image during both i and s phonation, respectively. Note the appropriate elevation of the velum with closure of the velopharyngeal port as well as the tongue position.

Tables
Variable Description Pharyngeal depth Linear distance (mm) from PNS to PPW or adenoid pad as seen on the midsagittal image Velar length Curvilinear distance (mm) from the posterior nasal spine to the tip of the uvula as seen on the midsagittal image VP ratio Calculation obtained from the dividing velar length by pharyngeal depth Effective velar length Linear distance (mm) from the posterior border of the hard palate to the point of levator muscle insertion into the velum as seen on the midsagittal image EVP ratio Calculation obtained from dividing effective velar length by the pharyngeal depth Adenoid depth Linear distance (mm) along the palatal plane from the adenoid pad to the posterior end of the adenoid Note:—PNS indicates posterior nasal spine; PPW, posterior pharyngeal wall; VP, velopharyngeal; EVP, effective VP.
↵a Adapted with permission from Perry JL, Kotlarek KJ, Sutton BP, et al. Variations in velopharyngeal structure in adults with repaired cleft palate. Cleft Palate Craniofac J 2018;55:1409-18.
- Table 2:
The mean (SD) of pertinent variables for quantitively examining VPI and results of analysis of variancea,b,31
Variable Infants (4–23 mo.) Children (4–9 yr) Adolescents (10–19 yr) Adults (20+ yr) Pharyngeal depth 11.43 (4.46) 17.80 (4.79) 21.45 (4.62) 20.92 (4.14) Velar length 20.27 (3.32) 27.63 (4.17) 30.98 (5.10) 34.85 (4.79) VP ratio 2.08 (0.94) 1.70 (0.69) 1.51 (0.42) 1.73 (0.42) Effective velar length 8.58 (1.46) 12.07 (2.43) 13.12 (3.32) 13.72 (3.46) EVP ratio 0.89 (0.43) 0.74 (0.30) 0.63 (0.19) 0.67 (0.19) Adenoid depth 11.36 (4.38) 9.66 (5.49) 9.96 (5.49) 5.18 (3.88) Note:— EVP indicates effective velopharyngeal; VP, velopharyngeal.
↵a Measurements are listed in millimeters with the exception of VP ratio measures.
↵b Adapted from Haenssler et al.31 Table 3 which is copyrighted material and included here with the permission of the American Speech-Language-Hearing Association (ASHA).





{kind=link}