
Abstract
BACKGROUND AND PURPOSE: Dual-energy virtual NCCT has the potential to replace conventional NCCT to detect early ischemic changes in acute ischemic stroke. In this study, we evaluated whether virtual NCCT is noninferior compared with standard linearly blended NCCT, a surrogate of conventional NCCT, regarding the detection of early ischemic changes with ASPECTS.
MATERIALS AND METHODS: Adult patients who presented with suspected acute ischemic stroke and who underwent dual-energy NCCT and CTA and brain MR imaging within 48 hours were included. Standard linearly blended images were reconstructed to match a conventional NCCT. Virtual NCCT images were reconstructed from CTA. ASPECTS was evaluated on conventional NCCT, virtual NCCT, and DWI, which served as the reference standard. Agreement between CT assessments and the reference standard was evaluated with the Lin concordance correlation coefficient. Noninferiority was assessed with bootstrapped estimates of the differences in ASPECTS between conventional and virtual NCCT with 95% CIs.
RESULTS: Of the 193 included patients, 100 patients (52%) had ischemia on DWI. Compared with the reference standard, the ASPECTS concordance correlation coefficient for conventional and virtual NCCT was 0.23 (95% CI, 0.15–0.32) and 0.44 (95% CI, 0.33–0.53), respectively. The difference in the concordance correlation coefficient between virtual and conventional NCCT was 0.20 (95% CI, 0.01–0.39) and did not cross the prespecified noninferiority margin of −0.10.
CONCLUSIONS: Dual-energy virtual NCCT is noninferior compared with conventional NCCT for the detection of early ischemic changes with ASPECTS.
ABBREVIATION:
- CCC
- concordance correlation coefficient
CT of the head is the most commonly used technique in the evaluation of stroke.1 Initial NCCT is the first-line study in the evaluation of suspected stroke to exclude intracranial hemorrhage or an alternative explanation for the patient’s symptoms. While early ischemic changes can be detected with NCCT, sensitivity is limited relative to DWI, which remains the reference standard for the detection of cerebral ischemia. However, MR imaging has limited availability.2 Early ischemic changes can be evaluated with ASPECTS on CT and are prognostic for functional outcome after IV thrombolysis and endovascular thrombectomy.3-5 ASPECTS is used for thrombectomy decision-making, because the large thrombectomy trials excluded patients with a low ASPECTS.6,7
Dual-energy CT enables acquisition of CT images at 2 different tube voltages instead of one and has several applications in neurointervention and neuroradiology.8 For instance, iodine contrast can be separated from blood components in patients with large-vessel occlusion who underwent endovascular thrombectomy.9,10 Similarly, it is also possible to subtract iodine maps from the CTA images, resulting in virtual NCCT images.
It is unknown whether virtual NCCT is noninferior to conventional NCCT for the detection of early ischemic changes. If virtual NCCT is noninferior compared with conventional NCCT, then the latter may be omitted from the stroke imaging protocol, reducing the radiation exposure to the patient. We performed a noninferiority analysis comparing virtual NCCT with standard linearly blended NCCT, a surrogate of conventional NCCT, for the detection of early ischemic changes with ASPECTS in patients with acute ischemic stroke.
MATERIALS AND METHODS
Patient Selection
Adult (18 years of age or older) patients who presented with suspected acute ischemic stroke and who underwent dual-energy CT (Somatom Force; Siemens) between February 2018 and February 2019 were selected for this study. The inclusion criteria were the availability of dual-energy NCCT and CTA scans and brain MR imaging within 48 hours after CT. Imaging was routinely performed as part of our standard-of-care stroke protocol. This study was approved by the Stanford University Institutional Review Board and complied with the Health Insurance Portability and Accountability Act. The need for informed consent was waived.
Image Acquisition and Preparation
NCCT and CTA were acquired helically using tube voltages of 80 and 140 kV (peak) with a tin filter and tube currents of 640 and 320 mAs, respectively. The images were acquired in dual-energy mode. The conventional NCCT was a standard linearly blended reconstruction to match a conventional 120-kVp NCCT. The virtual NCCT was reconstructed from CTA. The dual-energy data sets were routinely postprocessed using available dedicated software (syngo; Siemens) that was provided by the vendor to reconstruct virtual NCCT images. Section thicknesses of conventional and virtual NCCT were 3 mm.
DWI parameters were the following: TR = 6000 ms, TE = 78.2 ms, b-values = 0 and 1000, flip angle = 90°, and section thickness = 5 mm.
Interobserver Study
CT data were saved and presented in a random order to 2 experienced neuroradiologists (M.W. and J.W.D.) in the form of videos with fixed window settings (window width = 50 HU and window level = 40 HU). The reviewers evaluated the presence of early ischemic changes (yes or no) and rated ASPECTS, which is a prognostic score and allows quantification of the extensiveness of anterior circulation ischemic stroke.3 ASPECTS ranges from 0 to 10, with 0 indicating involvement of all the ASPECTS areas and 10 indicating involvement of none of the ASPECTS areas. One point is subtracted for every involved area. The areas include the caudate, internal capsule, lentiform nucleus, insular ribbon, anterior MCA cortex (M1), MCA cortex lateral to the insular ribbon (M2), posterior MCA cortex (M3), anterior cortex immediately rostral to M1 (M4), lateral cortex immediately rostral to M3 (M5), and posterior cortex immediately rostral to M3 (M6). Two separate scoring rounds were organized per reviewer, and the presentations contained a mix of virtual and conventional NCCT images. In case of disagreement, a third reviewer (G.Z.) was consulted to reach adjudicated assessments.
The DWIs were anonymized and presented to 1 neurointerventional radiologist with 7 years of experience (J.J.H.) who was blinded to the clinical and other imaging data. The reviewer was able to adjust the window settings and evaluated the presence of ischemia with ASPECTS, which can also be rated on DWI.11
We assessed interobserver agreement of early ischemic changes and ASPECTS, as well as the agreement between adjudicated CT assessments and MR imaging assessments.
Statistical Analysis
We reported frequencies and percentages for categoric characteristics and medians with first (Q1) and third (Q3) quartiles for continuous characteristics. These included symptom laterality (left/right/both/unknown), image assessability (yes/no), as well as MR imaging–assessed early ischemic change (presence/absence)—overall and for each of the 10 brain regions (M1–M6, caudate, lentiform nucleus, internal capsule, and insular cortex). Proportions of the involved brain regions were visualized as barplots.
The agreement between the 2 reviewers was quantified by calculating the Cohen κ, with disagreements weighted according to their squared distance from perfect agreement.12 The level of agreement was interpreted on the basis of the following intervals for κ: poor, <0.20; fair, 0.21–0.40; moderate, 0.41–0.60; good, 0.61–0.80; and very good, 0.81–1.00. Confidence intervals for κ statistics were based on 5000 bootstrap resamples.
Measures of sensitivity and specificity were calculated for virtual and conventional NCCT. We used a global test to compare the sensitivity and specificity.13
For feasibility, we concluded that the maximum study size was 200 patients. Our a priori power calculation determined that this would provide 77% power to show noninferiority, given a noninferiority margin of −0.10. Concordance between adjudicated CT assessments and the MR imaging criterion standard was quantified using the Lin concordance correlation coefficient (CCC),14,15 which is also a measure of accuracy against the criterion standard. Bootstrapped estimates were obtained of the differences between virtual and conventional NCCT with 2-sided 95% CIs. Noninferiority of virtual NCCT to conventional NCCT was prespecified as the lower boundary greater than −0.10 for the 95% CI of their difference in the CCC. In case the 95% CI of the difference in the CCC was greater than 0, superiority could be inferred.
All analyses were performed in the R statistical computing framework, Version 4.0 (http://www.r-project.org/), and the CCC was estimated using the epiR R package.
RESULTS
Imaging assessment was not possible in 3 of the 196 included patients. As a result, 193 patients remained for the final analysis (Table 1). In 100 patients (52%), ischemia was detected with MR imaging in different ASPECTS regions.
Baseline characteristics
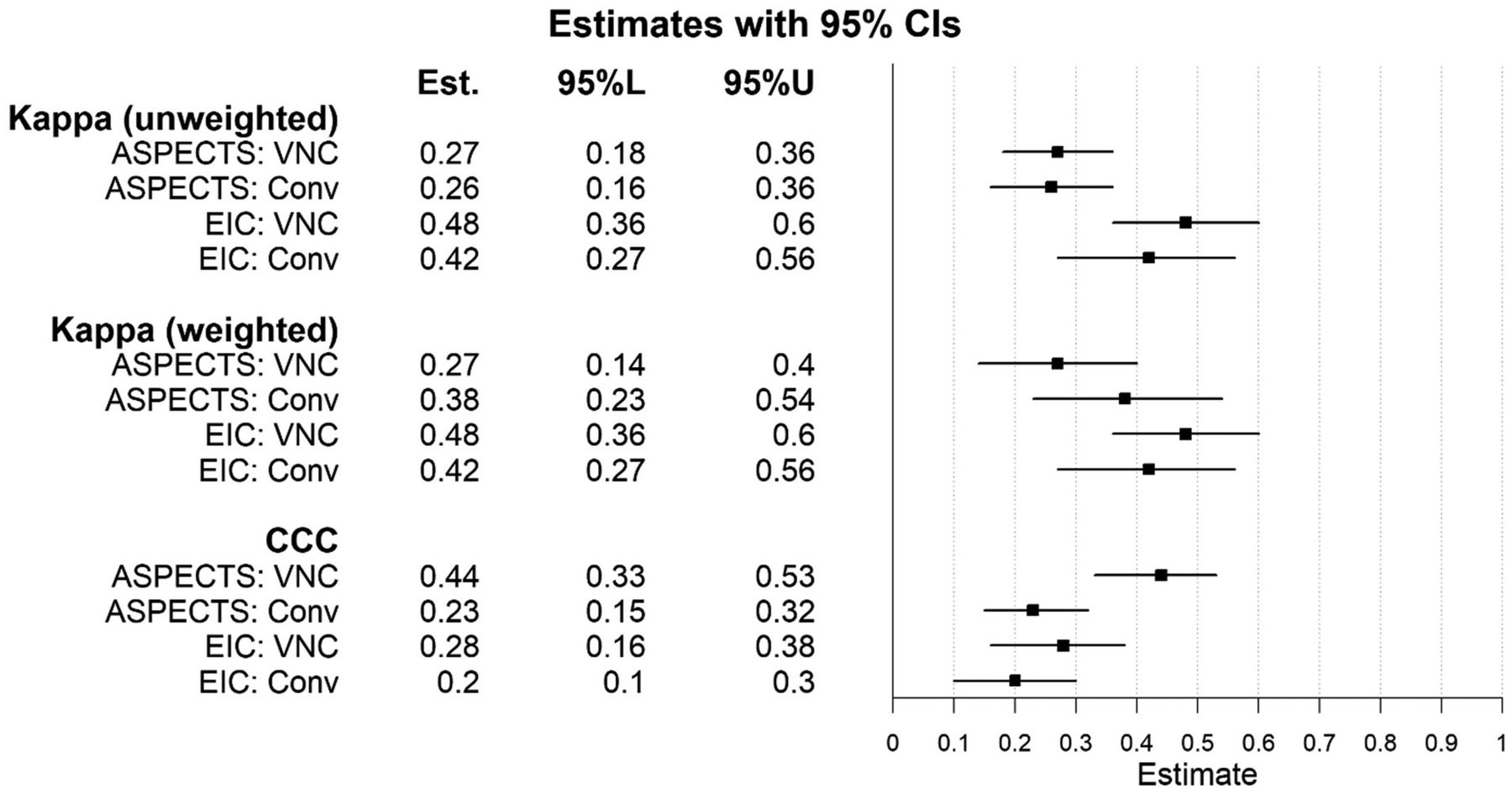
Some differences were observed between the observations of reviewers 1 and 2 (Fig 1). Interobserver agreement regarding the presence of early ischemic changes was moderate for conventional (weighted κ = 0.42; 95% CI, 0.27–0.56) and virtual NCCT (weighted κ = 0.48; 95% CI, 0.36–0.6) (Fig 2). Interobserver agreement regarding ASPECTS was fair for conventional NCCT (weighted κ = 0.38; 95% CI, 0.23–0.54) and virtual NCCT (weighted κ = 0.27; 95% CI, 0.14–0.4).

The proportion of CT scans showing early ischemic changes by reviewer and technique. VNC indicates virtual noncontrast; EIC, early ischemic changes; Cau, caudate nucleus; LNuc, lentiform nucleus; ICap, internal capsule; ICor, insular cortex.

Estimates of interobserver agreement between CT and the reference standard and accuracy with 95% confidence intervals. VNC indicates virtual noncontrast; EIC, early ischemic changes; Conv, conventional; 95%L, lower bound of the 95% confidence interval; 95%U, upper bound of the 95% confidence interval.
The sensitivity of virtual and conventional NCCT for the detection of early ischemic changes was 0.37 (95% CI, 0.28–0.47) and 0.27 (95% CI, 0.19–0.37), respectively (P = .078). Specificity was 0.91 (95% CI, 0.83–0.96) and 0.94 (95% CI, 0.86–0.98), respectively (Table 2). The global test finding was not significant (P = .111).
Adjudicated-versus–criterion standard assessments
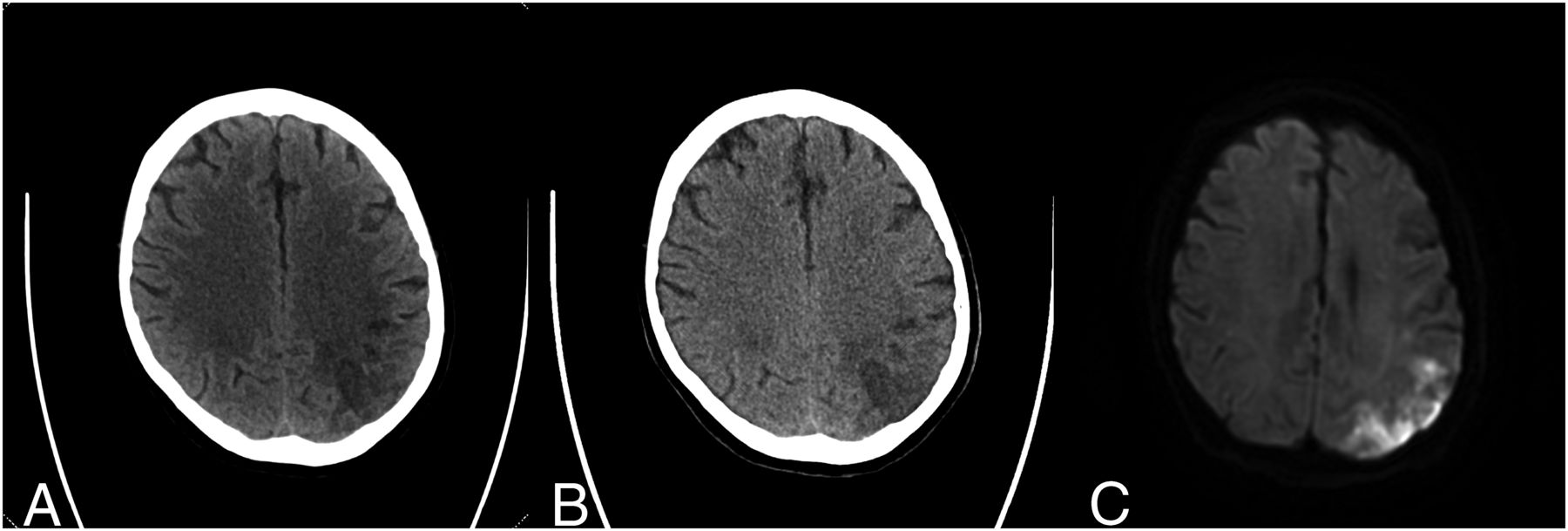
The forest plots (Fig 2) for the CCC showed overlapping intervals for early ischemic changes and nonoverlapping 95% CIs for ASPECTS. The difference in the CCC between virtual and conventional NCCT was 0.201 (95% CI, 0.014–0.389) regarding ASPECTS and 0.077 (95% CI, −0.041–0.191) regarding early ischemic changes. Neither 95% CI for the difference in the CCC crossed the prespecified noninferiority margin of −0.10, thereby establishing noninferiority of virtual NCCT compared with conventional NCCT with respect to both ASPECTS and early ischemic changes. Furthermore, virtual NCCT was demonstrated to be superior to conventional NCCT with respect to ASPECTS. Sample acquisitions of conventional NCCT, virtual NCCT, and DWI MR imaging are shown in Fig 3.

A sample case of a 66-year-old male patient who presented with right-sided weakness and numbness (NIHSS 7). His medical history included diabetes mellitus, hypertension, hyperlipidemia, prior smoking, and prior ischemic stroke, for which the patient used dual-antiplatelet therapy. The time between last seen well and CT was 14 hours. The time between CT and DWI was 12 hours. Conventional NCCT (A) and virtual NCCT (B) show early ischemic changes in the left parietal lobe (ASPECTS region M6). In the same region, DWI (C) shows hyperintensity, indicating diffusion restriction compatible with ischemia.
DISCUSSION
This study shows that detection of early ischemic changes with dual-energy virtual NCCT in patients with suspected stroke is noninferior compared with standard linearly blended NCCT. Furthermore, virtual NCCT was demonstrated to be superior to conventional NCCT with respect to ASPECTS.
To the best of our knowledge, no studies have evaluated early ischemic changes on virtual NCCT images reconstructed from CTA. Studies in fields other than neuroradiology have shown contradictory results, and the reliability of the virtual NCCT maps seems to be influenced by the clinical indication.16,17 Excluding intracranial hemorrhage is an important application of NCCT in the acute stroke setting and can also be done with dual-energy virtual NCCT images.18-20 Dual-energy CT can also be used to distinguish intracranial hemorrhage and extravasation of iodine contrast after endovascular treatment of stroke.21-23 In addition, 1 study showed high sensitivity and specificity for detecting the hyperdense artery sign on dual-energy virtual NCCT.24 Previous studies showed that the detection of the ischemic core with dual-energy virtual NCCT images derived from NCCT was superior compared with conventional NCCT.22,25,26 It is difficult to compare these studies with our study because the reconstructions were acquired from different CT images (NCCT versus CTA). However, all studies indicated that dual-energy virtual NCCT has the potential to replace conventional NCCT with respect to the detection of early ischemic changes.
The observed interobserver variability with regard to the detection of early ischemic changes and ASPECTS was moderate and fair, respectively, and similar for virtual NCCT and conventional NCCT in this study. ASPECTS is known to have relatively poor intraobserver and interobserver agreement, as was the case in this study.27 Recently, this finding was supported by a study that demonstrated a relatively poor interobserver agreement in a large group of 100 readers.28 The agreement, based on the CCC, between the dual-energy virtual NCCT assessments and MR imaging assessments regarding the presence of early ischemic changes was slightly better than the agreement between conventional NCCT assessments and MR imaging assessments. With regard to ASPECTS, the CCC showed fair agreement between both CT modalities and MR imaging, which is in line with findings in a previous study.29
The applications of dual-energy CT are becoming increasingly apparent. If dual-energy virtual NCCT of the brain can replace conventional NCCT, this would result in less radiation exposure for the patient. Whether dual-energy virtual NCCT saves time in the acute stroke work-up needs to be elucidated because dual-energy reconstructions also take time. Automated dual-energy reconstructions do not add extra time to the imaging protocol, unless manual processing is required. The disadvantages of replacing conventional NCCT with virtual NCCT include the necessity of acquiring CTA, turning on the dual-energy mode, and the requirements of added storage and bandwidth. Besides replacing conventional NCCT, future applications of virtual NCCT may include improvement of the conventional NCCT in case of severe movement artifacts and reduction of the radiation dose in a nonacute setting.
Most dual-energy CT scanners, using a dual source with a dual detector or a monosource with rapid kilovolt (peak) switching, require that the dual-energy setting be switched on beforehand to acquire dual-energy data.30 Other detector-based spectral CT scanners have a single source and a single dual-layered detector that is always switched on. In the acute stroke imaging work-up, NCCT needs to be acquired first to exclude intracranial hemorrhage. Because the dual-energy virtual NCCT images need to be reconstructed from the CTA, which is often only performed if an NCCT has ruled out an intracranial hemorrhage, it is difficult to omit the conventional NCCT in clinical practice. On the other hand, even in patients who have intracranial hemorrhage, CTA is often performed to look for cerebral aneurysms, cerebral arteriovenous malformations, or other vascular malformations as the cause of the bleed. Taken together, the role of dual-energy virtual NCCT seems dependent on the indication and on whether CTA is performed regardless of the findings on NCCT.
Several strengths can be noted in this study. To prevent observation bias, the observers who assessed the CT were blinded to clinical information and MR images; vice versa, the observer who assessed the MR images was blinded to the CT images. Another strength was the power calculation, which helped to achieve a reliable noninferiority analysis.
A limitation of this study was the potential risk of selection bias because patients were selected who underwent dual-energy CT and diffusion-weighted MR imaging. However, besides the imaging criteria, we used wide inclusion criteria (adult patients with a suspicion of acute ischemic stroke). Nevertheless, the results of this study need to be validated, preferably in a large prospective study. Due to missing data, extensive patient characteristics were not reported in this study. Although we did not use conventional single-source NCCT in this study, standard linearly blended images closely resemble conventional NCCT.31 Another limitation is the time interval between the acquired CT scan and the DWI. Although the time window was within 48 hours, this theoretically could have resulted in larger or additional infarcts on MR imaging compared with CT. This possibility may also partially explain the fair agreement between CT and MR imaging in this study. In addition, MR imaging is more sensitive for detecting ischemia; therefore, ASPECTS may differ between CT and MR imaging assessments, which are acquired simultaneously because small infarcts may be visible on MR imaging but not on CT. In this study, the dual-energy CT scanner and the software of 1 vendor were used, limiting the ability to generalize these findings. Future studies should include a broader range of CT vendors and software to increase generalizability.
CONCLUSIONS
Dual-energy virtual NCCT is noninferior compared with NCCT for the detection of early ischemic changes with ASPECTS.
Footnotes
This research has been made possible by the Dutch Heart Foundation, the Netherlands Organisation for Scientific Research, and the Domain Applied and Engineering Sciences, as part of their joint strategic research program: “Earlier Recognition of Cardiovascular Diseases” (grant No. 14732).
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received January 21, 2022.
- Accepted after revision June 17, 2022.
- © 2022 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.