
Abstract
BACKGROUND AND PURPOSE: Classic trigeminal neuralgia is a clinical syndrome of facial pain, most often attributable to vascular compression of the proximal cisternal segment of the trigeminal nerve and treatable with microvascular decompression of the nerve. Some patients, however, meet all clinical criteria for classic trigeminal neuralgia yet do not respond to microvascular decompression. Because the reasons for surgical failure are not well understood, the aim of this study was to determine if a subset of patients with classic trigeminal neuralgia could be distinguished by measuring the angle of the trigeminal nerve in the sagittal plane as the nerve traverses the porus trigeminus.
MATERIALS AND METHODS: We retrospectively identified patients with either classic trigeminal neuralgia (n = 300) or hemifacial spasm (n = 300) who had undergone MR imaging, including 3-plane steady-state free precession imaging. Patients with hemifacial spasm served as controls. On sagittal steady-state free precession images, we measured the angle of each trigeminal nerve as it crosses through the porus trigeminus into the Meckel cave (SATNaPT). In patients with classic trigeminal neuralgia, we separated the nerves into symptomatic and asymptomatic sides. We compared these 3 groups using the Student t test.
RESULTS: Control patients had a mean SATNaPT of 170° (SD, 11°) with a normal distribution. The contralateral asymptomatic nerve in patients with classic trigeminal neuralgia had the same distribution of angles. The symptomatic nerves in patients with classic trigeminal neuralgia had a bimodal distribution; 83% of patients fell into the same distribution as the asymptomatic nerves, but the other 15% had an average angle of 143° (SD, 7°). This difference was statistically significant (P < .0001).
CONCLUSIONS: Patients with the clinical syndrome of classic trigeminal neuralgia fell into 2 categories based on the radiologic measurement of the SATNaPT. Most patients had an anatomically normal nerve that was affected by vascular compression, but 17% of these patients had aberrant anatomy that may cause or contribute to their clinical presentation. Further study is needed to determine whether this subset of patients should receive a different surgery to better address their underlying anatomic abnormality. The SATNaPT measurement should be included in every MR imaging interpretation performed on patients with classic trigeminal neuralgia.
ABBREVIATIONS:
- cTN
- classic trigeminal neuralgia
- HFS
- hemifacial spasm; MVD = microvascular decompression
- SATNaPT
- sagittal angle of the trigeminal nerve at the porus trigeminus
- SSFP
- steady-state free precession
Trigeminal neuralgia is a syndrome of pain in the distribution of the trigeminal nerve. Although trigeminal neuralgia can be caused by diseases such as multiple sclerosis or tumors, the most common form is classic trigeminal neuralgia (cTN). The International Headache Society has established objective criteria for the diagnosis of cTN, including paroxysms that last from a fraction of a second to 2 minutes; severe intensity of pain; electric, stabbing, or sharp pain; and episodes precipitated by innocuous stimuli to the face.1
In 80%–90% of patients, cTN is associated with arterial compression of the trigeminal nerve.2,3 A tortuous artery, most frequently the superior cerebellar artery, abuts (and often distorts or displaces) the trigeminal nerve near its root entry point.4 Although not well-understood, pulsations from the artery presumably irritate the adjacent nerve, causing the characteristic pain syndrome.
Voltage-gated sodium channel blockers such as carbamazepine and oxcarbazepine are considered first-line therapy for cTN.1 Unfortunately, most patients progress despite medical therapy and eventually require surgery. The surgical procedure of choice is microvascular decompression (MVD), in which the compressive artery is isolated from the trigeminal nerve and an interpositional pledget is placed between the artery and nerve to prevent further injury. MVD has a high success rate when performed on patients who meet all the criteria for cTN.2,5,6
MR imaging of the cranial nerves using high-resolution T2-weighted sequences is the technique of choice for imaging patients with cTN before surgery.4 The offending artery is identified, and the degree of compression in quantified. This process is useful not only for surgical planning, but it also conveys prognostic information.2,7
Some patients meet all the criteria for cTN yet still do not respond to surgical therapy. Although the degree of neurovascular compression and response to medication help predict which patients will respond to MVD,7,8 there may be other anatomic differences between responders and nonresponders that could predict surgical success or suggest alternative treatments. In particular, some patients have bony distortions of their skull base that result in superior displacement of the porus trigeminus (the opening between the prepontine cistern and the Meckel cave). This aberrant anatomy displaces the trigeminal nerve upward, forming an acute angle between the cisternal and cavernous portions of the nerve when viewed in the sagittal plane. We refer to this angle as the sagittal angle of the trigeminal nerve at the porus trigeminus (SATNaPT).
The purpose to this study was to establish normal measurements for the SATNaPT in asymptomatic individuals and to determine whether the SATNaPT differs between asymptomatic individuals and patients with cTN.
MATERIALS AND METHODS
The institutional review board of University of Pittsburgh approved this study as performed on retrospective data and thus waived informed consent.
Patient Selection
From the surgical registry at the University of Pittsburgh, we identified 300 consecutive patients with cTN who had undergone MR imaging before surgery. We then identified 300 consecutive patients with hemifacial spasm (HFS) who had undergone MR imaging. All patients in the registry were screened for facial nerve and trigeminal nerve symptoms; patients with both were excluded from this study. Because the patients with HFS had no symptoms attributable to their trigeminal nerves, they served as controls for measurement of the trigeminal nerves. We recorded age, sex, and symptom laterality for all patients. All patients were imaged between 2013 and 2018 at a single academic hospital. Patients were excluded (and not counted toward the total of 300 patients) if they had been previously treated with MVD or if motion artifacts prevented measurement.
Imaging Protocol
Our MR imaging protocol for patients with presumed vascular compression of the cranial nerves consists of sagittal T1 and axial FLAIR images through the entire brain. Balanced steady-state free precession (SSFP) images with dual excitation, which are often referred to by vendor acronyms such as FIESTA or CISS, are performed in the axial, coronal, and sagittal planes through the cranial nerves. We do not rely on reformatted images because we have found them to be less reliable than multiplanar imaging, allowing us to use a single protocol for evaluating compression of the trigeminal, facial, and glossopharyngeal nerves. The SSFP sequences use optimized TR and TE (usually about 5.5 and 2 ms), a flip angle of 65°, FOV of 18 cm, matrix of 384 × 256, 1.0-mm section thickness, 0.5-mm section interval, and NEX of 2.
Measurements
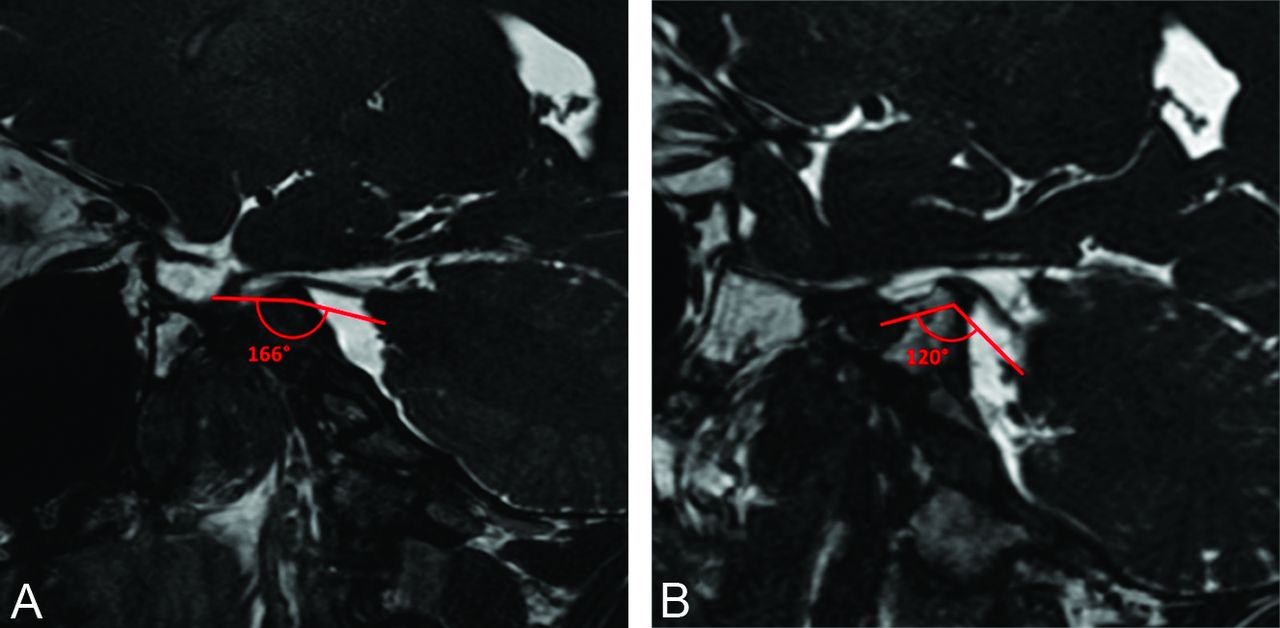
The images were evaluated by a single dedicated head and neck radiologist with 20 years of experience in practice. On a single sagittal SSFP image, the angle between the trunk of the trigeminal nerve (in the prepontine cistern) and the uppermost branch of the trigeminal nerve (within the Meckel cave) was measured (Fig 1). This constitutes the SATNaPT. Each trigeminal nerve angle was measured separately on each patient using the angle measurement tool in the PACS. The observer was blinded to the patients’ symptoms and the scans were presented in random order.

Sample measurements of the SATNaPT. Sagittal SSFP MR images show a normal angle of 166° (A) and a decreased angle of 120° (B). The angle measurements are shown below the nerves to avoid obscuring the anatomy.
Statistical Analysis
We analyzed 3 groups of nerves: asymptomatic nerves in control patients, asymptomatic (contralateral) nerves in patients with cTN, and symptomatic nerves in patients with cTN. Normal distribution of data was confirmed, and normal (bell-shaped) curves were fitted to the histogram of angles in each population. For populations with a bimodal distribution, the least-squares method was used to optimize a sum of 2 normal curves. In anticipation of similar normal distributions between left and right ears as well as between control patients and uninvolved ears in patients with trigeminal neuralgia, equivalence testing was used to demonstrate similarities among these groups.9 The Student t test was used to demonstrate pair-wise differences between those with affected trigeminal nerves and the other groups.
RESULTS
We accrued 306 patients with HFS as controls; 6 were excluded because of excessive motion artifacts on their scans. Of the remaining 300 controls, 88 (29%) were men and 212 (71%) were women, with an average age of 56 years (range, 20−88 years). We accrued 331 patients with cTN; 13 were excluded for motion artifacts and 18 were excluded because they had prior MVD surgery. Of the remaining 300 patients, 116 (39%) were men and 184 (61%) were women, with an average age of 63 years (range, 23–87 years). Although some patients had bilateral symptoms, 1 side was always dominant and that side was considered symptomatic for our analyses.
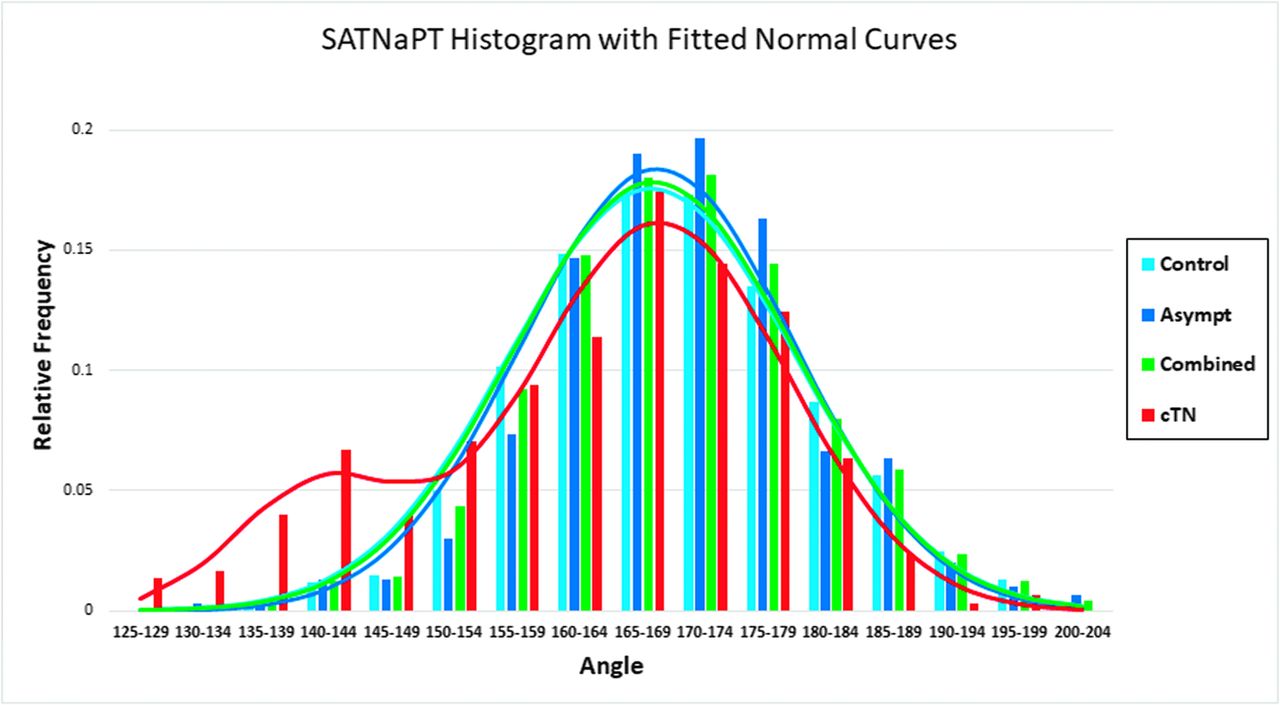
In the healthy population, the SATNaPT has an average value of 170°. It follows a normal distribution with an SD of 11° (Fig 2). Equivalence testing showed no differences based on sex, age (dichotomized to the median), or side (left/right), using Δ = 10°. The asymptomatic (contralateral) nerves of patients with cTN also have an average SATNaPT of 170° (SD, 11°). There was no statistical difference between the SATNaPT for controls and the asymptomatic nerves of patients with cTN (P = .48).

Histogram of SATNaPT in different patient populations. The horizontal axis angle is measured in 5° intervals. The vertical axis is the percentage of patients. A best-fit normal curve is also shown for each histogram. Note that all curves are similar except the cTN curve, which has a bimodal distribution in which 17% of the nerves form a separate population with decreased SATNaPT. Asympt indicates the contralateral asymptomatic nerve in patients with cTN; Control, patient scanned for other reasons; Combined, all asymptomatic nerves (control plus Asympt).
The symptomatic nerves in patients with cTN followed a bimodal distribution (Fig 2); 83% of patients had the larger peak, which had an average SATNaPT of 170° (SD, 10°) (similar to that in controls). The remaining 17% of patients had an average SATNaPT of 143° (SD, 7°). The symptomatic nerves differed significantly from the nerves in control patients and also the contralateral asymptomatic nerves in patients with cTN (P < .0001).
DISCUSSION
We have identified 2 distinct groups of patients who present with cTN. These 2 groups are distinguishable by the anatomy of the trigeminal nerve as it passes through the porus trigeminus. Most patients have normal trigeminal nerve anatomy, and their symptoms are attributable to vascular compression in the traditional model popularized by Jannetta.10
However, about one-fifth of patients have aberrant anatomy with a decreased SATNaPT. It is unclear how this underlying anatomy, which is rare in the asymptomatic population, contributes to the symptoms of cTN. One possibility is that the trigeminal nerve becomes stretched as it extends over an elevated porus trigeminus; this stretching may inherently injure the nerve or may make it more susceptible to vascular compression. It is unclear whether patients with a decreased SATNaPT are less likely to respond to MVD; this is an area for further research that may provide insight into the role that the SATNaPT plays in the pathogenesis of cTN.
This study is limited by its single-institution design, in which all measurements were made by a single experienced radiologist. We did not attempt to assess interobserver variability. Another potential criticism of this work is that severe displacement of the cisternal segment of the trigeminal nerve by a compressing artery could result in a decreased SATNaPT, in which case the effect on the SATNaPT would be a consequence of vascular compression rather than a cause of disease. Subjective evaluation of the patients in our series does not support this theory because the degree of nerve displacement was mild or absent in most patients with a decreased SATNaPT.
It is difficult to define a precise threshold for an “abnormal” SATNaPT because there is overlap between the patients with a normal SATNaPT and those with a decreased SATNaPT. Outcome analysis is needed to define an optimal cutoff point for prediction of surgical success. However, a value below 150° should prompt concern.
It is possible that patients with a decreased SATNaPT would benefit from additional or different surgery at the time of MVD. Further study is needed on the rates of coexistence between radiologic vascular compression and decreased SATNaPT and on outcomes for these groups of patients.
CONCLUSIONS
Patients with the clinical syndrome of cTN fall into 2 categories based on the radiologic measurement of the SATNaPT. Most patients have an anatomically normal nerve that is affected by vascular compression, but 17% of these patients have aberrant anatomy that may cause or contribute to their clinical presentation. Further study is needed to determine whether this subset of patients should undergo different surgery to better address their underlying anatomic abnormality. Radiologists should be aware of this potentially important anatomic variant and should know how to measure the SATNaPT.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received November 25, 2021.
- Accepted after revision July 19, 2022.
- © 2022 by American Journal of Neuroradiology





{kind=link}
{kind=link}