
Abstract
BACKGROUND AND PURPOSE: Published data regarding embolic protection device efficacy is mixed, and its use during carotid artery stent placement remains variable. We, therefore, examined the frequency of embolic protection device use and its association with outcomes after carotid artery stent placement using a national quality improvement data base.
MATERIALS AND METHODS: Patients undergoing carotid artery stent placement with or without embolic protection devices were identified in the American College of Surgeons National Surgical Quality Improvement Program data base. The primary outcome was the incidence of major adverse cardiovascular events (defined as death, stroke, or myocardial infarction/arrhythmia) within 30 days. Propensity scoring was used to create 2 matching cohorts of patients using demographic and baseline variables.
RESULTS: Between 2011 and 2018, among 1200 adult patients undergoing carotid artery stent placement, 23.8% did not have embolic protection devices. There was no trend toward increased embolic protection device use with time. Patients without embolic protection device use received preoperative antiplatelets less frequently (90.6% versus 94.6%, P = .02), underwent more emergent carotid artery stent placement (7.2% versus 3.6%, P = .01), and had a higher incidence of major adverse cardiovascular events (OR = 1.81; 95% CI, 1.11–2.94) and stroke (OR = 3.31; 95% CI, 1.71–6.39). After compensating for baseline imbalances using propensity-matched cohorts (n = 261 for both), carotid artery stent placement without an embolic protection device remained associated with increased major adverse cardiovascular events (9.2% versus 4.2%; OR = 2.30; 95% CI, 1.10–4.80) and stroke (6.5% versus 1.5%; OR = 4.48; 95% CI, 1.49–13.49).
CONCLUSIONS: Lack of embolic protection device use during carotid artery stent placement is associated with a 4-fold increase in the likelihood of perioperative stroke. Nevertheless, nearly one-quarter of patients in the American College of Surgeons National Surgical Quality Improvement Program underwent unprotected carotid artery stent placement. Efforts targeting improved embolic protection device use during carotid artery stent placement are warranted.
ABBREVIATIONS:
- ACS-NSQIP
- American College of Surgeons National Surgical Quality Improvement Program
- CAS
- carotid artery stent placement
- EPD
- embolic protection device
- MACE
- major adverse cardiovascular events
Carotid artery stent placement (CAS) has developed rapidly during the past 30 years to become a viable option for carotid revascularization, especially in patients at high-risk for carotid endarterectomy.1 One of the major remaining concerns about CAS is the risk of embolic stroke caused by mobilization and migration of plaque fragments during stent placement.2 Embolic protection devices (EPDs) have been developed to reduce the risk of distal embolization.3 In 2011, guidelines from the American Stroke Association suggested that the use of EPDs during CAS can be beneficial to reduce the risk of stroke when the risk of vascular injury is low.4 Nevertheless, randomized trials, systematic reviews, and meta-analyses offer conflicting evidence regarding the frequency and efficacy of EPD use, with some showing diminished rates of postoperative stroke and death when an EPD was used,5⇓⇓-8 whereas others have not supported the benefit of an EPD during CAS.9⇓⇓-12 We, therefore, examined the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) data base to determine the frequency of EPD use during CAS and compared preoperative and postoperative characteristics, complications, and outcomes of patients undergoing CAS with and without an EPD.
MATERIALS AND METHODS
Our retrospective observational study did not require institutional review board approval or patient consent because the ACS-NSQIP is a publicly available, de-identified data base.
Data Base
Patients who underwent CAS were identified using the vascular-targeted ACS-NSQIP Participant Use Data Files from 2011 (when targeted data bases were introduced) to 2018 (the latest data base available at time of analysis, spanning 98 hospitals). The ACS-NSQIP is a multi-institutional collaboration that collects information, including preoperative risk factors, intraoperative variables, and 30-day morbidity and mortality. The CAS-targeted module provides additional information including symptom status, anatomic and physiologic high-risk factors, preoperative antiplatelet medications, and the degree of carotid artery stenosis. Previous studies have shown the reliability of this data base.13,14 Patients with complete ipsilateral carotid occlusion and patients who underwent thrombectomy at the same admission were excluded. Included patients were divided into 2 groups (CAS with EPD and CAS without EPD). General risk factors such as age, sex, race, body mass index, smoking, diabetes mellitus, preoperative dialysis, hypertension, history of chronic obstructive pulmonary disease and congestive heart failure, preoperative functional status, and emergency procedure status were obtained from the main ACS-NSQIP dataset. Anatomic high-risk factors were defined by the ACS-NSQIP to include recurrent stenosis, radical neck dissection, contralateral occlusion, prior neck radiation, contralateral laryngeal nerve injury/palsy, and a high anatomic lesion (C2 or higher). Physiologic high-risk factors were defined by the ACS-NSQIP as New York Heart Association congestive heart failure class III/IV, left ventricular ejection fraction <30%, unstable angina, and recent (within 30 days) myocardial infarction. Ipsilateral carotid stenosis was divided into 3 groups based on the baseline Doppler sonography or angiography: mild (estimate of <50%), moderate (estimate of 50%–79%), and severe (estimate of 80%–99%) stenosis. A list of all variable definitions captured by the ACS-NSQIP can be found in the data user guides.15,16
Outcomes
The primary outcome was the occurrence of major adverse cardiovascular events (MACE), defined as the composite of death, stroke, and myocardial infarction/arrhythmia. Secondary outcomes included individual components of MACE as well as TIA, length of stay > 2 days, nonroutine discharge, and unplanned readmission within 30 days postoperatively. Discharge disposition to any hospital or facility other than home was designated as nonroutine discharge. All outcomes used prespecified variables in ACS-NSQIP.
Missing Data and Propensity Matching
The percentage of missing values across all variables varied between 0% and 4.9%. In total, 184 of 1200 records (15%) were incomplete. We used multiple imputation with fully-conditional specification using all covariates and outcome variables to create and analyze 20 multiple imputed datasets. This method is widely considered to improve accuracy and statistical power relative to other missing-data techniques.17 To address potential confounding nonrandom differences between patients who underwent CAS with EPD versus those who underwent CAS without EPD, we used propensity scoring techniques to create 2 cohorts of patients from the entire study population who were matched on their propensity for undergoing CAS with EPD versus without EPD. In this analysis, a logistic regression model was created for each of the 20 imputed datasets to estimate the likelihood of undergoing CAS without EPD (rather than CAS with EPD) using all demographic and baseline variables as potential predictors. The logit coefficients from this model were then used to create a propensity score for undergoing CAS without EPD for each patient from the entire study population that ranged from 0 to 1 and represented the likelihood of undergoing CAS without EPD rather than CAS with EPD. We then averaged the 20 propensity scores for each case across the completed datasets18 and performed nearest-neighbor matching (with a caliper distance of 0.05) with these averaged scores to create 2 evenly matched cohorts of CAS with EPD and CAS without EPD by a caliper-matching algorithm, with patients being used only once in the matching.
Statistical Analysis
Baseline patient- and procedure-related characteristics of patients undergoing CAS with and without EPD were compared across both the entire study population and the propensity score–matched groups using χ2 and Fisher exact (when appropriate) tests in the imputed dataset. For comparison, we also performed the analysis on the subset of available cases before imputation. The trend of EPD use was assessed during the entire time period by annual percentage change estimates using the Joinpoint Regression Program (Version 4.6.0.0; Statistical Methodology and Application Branch, Surveillance Research Program, National Cancer Institute, Bethesda, Maryland).19 Logistic regression was performed on pre- and postmatched imputed datasets to assess the effect of EPD on postprocedural outcomes. Propensity score matching was performed using R statistical and computing software, Version 4.0.2 (http://www.r-project.org) and the MatchIt20 package for R (https://cran.r-project.org/web/packages/MatchIt/MatchIt.pdf). Multiple imputation and statistical analyses were performed using SPSS Statistics for Windows, Version 26 (IBM), and statistical significance was defined as P < .05.
RESULTS
Demographics and Clinical Characteristics
Overall, 1200 adult patients undergoing CAS in the vascular-targeted ACS-NSQIP dataset between 2011 to 2018 met the criteria for analysis, of whom 277 (23.8%) underwent CAS without an EPD. The frequency of EPD use did not show any significant trend (annual percentage change, −0.74; 95% CI, −3.61–2.23; P = .56) during the study period (Fig 1). Demographics and characteristics of the study cohorts (before and after propensity score matching) are shown in the Online Supplemental Data. Use of multiple imputation to account for missing variables (0%–4.9% across the dataset) did not significantly affect the results (Online Supplemental Data); hence, subsequent analyses used the imputed dataset. There were no significant differences between 2 groups in age, sex, race, body mass index, preoperative comorbidities, functional dependency, American Society of Anesthesiologists classification, symptom status, or anatomic or physiologic high-risk factors before matching. However, stenosis categories were differently distributed across the 2 groups (P = .02), and preoperative antiplatelet medication was administered more often in patients who had CAS with EPD (94.6% versus 90.6%, P = .02). Subgroup analysis showed that the proportion of patients who did not receive preoperative antiplatelets was higher in emergency cases compared with nonemergency cases (43.4% versus 4.6%, P < .001). Finally, CAS without an EPD was more likely to have been performed emergently compared with CAS with an EPD (7.2% versus 3.6%, P = .01). These baseline differences were no longer seen after propensity score matching (Online Supplemental Data).

Annual proportion of EPD use during CAS (ACS-NSQIP CAS-targeted module, 2011–2018). Asterisk indicates mean percentage use of an EPD during the entire study period.
Clinical Outcomes before and after Matching
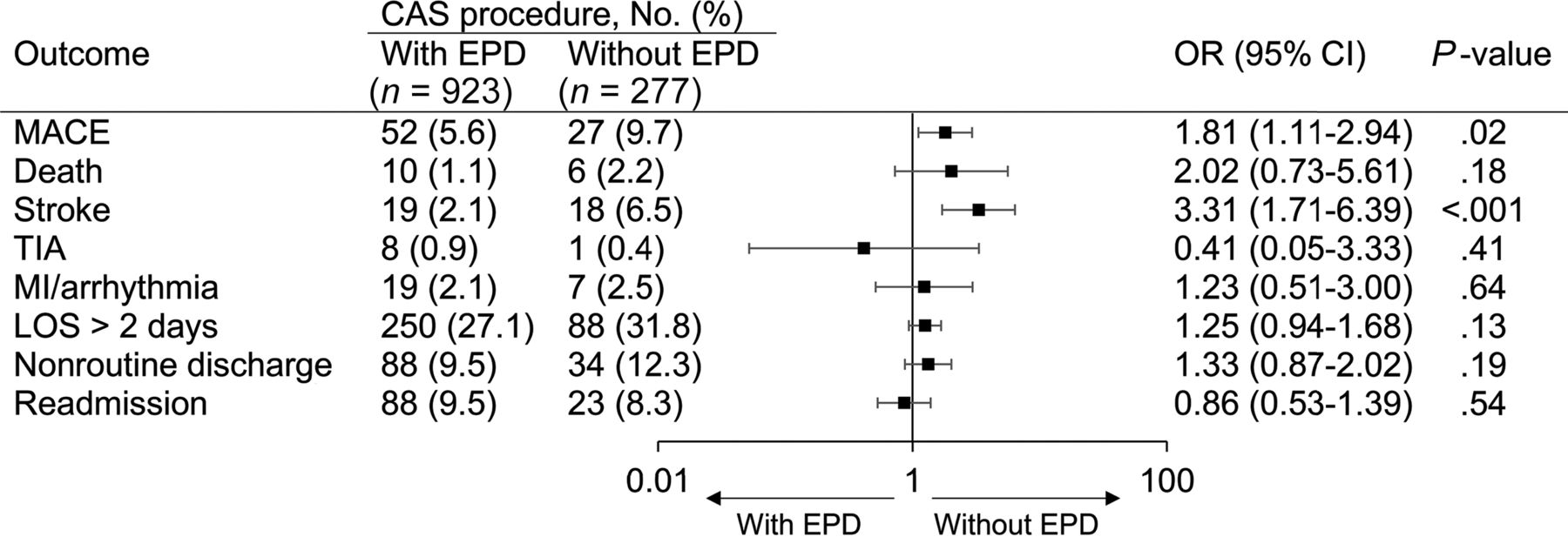
The 30-day postoperative outcomes of the entire cohort (before matching) are shown in Fig 2. The incidence of MACE was higher in CAS without EPD than in the group with EPD (OR = 1.81; 95% CI, 1.11–2.94; P = .02), and was unrelated to the degree of stenosis being treated (P = .68 and P = .16 for CAS with and without EPD, respectively). Analysis of secondary outcomes revealed CAS without an EPD had a higher incidence of stroke compared with CAS with an EPD (OR = 3.31; 95% CI, 1.71–6.39; P < .001). Other secondary outcomes did not show any differences between the 2 groups.

OR of outcomes in all patients undergoing CAS with or without EPD (ACS-NSQIP CAS-targeted module, 2011–2018). LOS indicates length of stay.
To account for potential confounders and baseline imbalances when comparing CAS with and without EPD, we performed propensity score matching between the 2 groups, yielding 261 patients in each matched cohort. After propensity score matching, no significant differences remained in baseline demographics and characteristics between the 2 cohorts (including stenosis categories, proportion of CAS performed emergently, and antiplatelet use), confirming that the cohorts were well-matched (Online Supplemental Data). Outcomes after matching are shown in Fig 3. The incidence of MACE remained higher in CAS without EPD compared with CAS with EPD (OR = 2.30; 95% CI, 1.10–4.80; P = .03) as did stroke (OR = 4.48; 95% CI, 1.49–13.49; P = .008). Other secondary outcomes were not significantly different between the matched cohorts.

OR of outcomes in propensity-matched cohorts of patients undergoing CAS with or without EPD (ACS-NSQIP CAS-targeted module, 2011–2018). LOS indicates length of stay.
DISCUSSION
Our analysis of carotid stent placement records from the most recent 8 years of the ACS-NSQIP data base (2011–2018) found that approximately one-quarter of CAS was performed without an EPD each year and that this practice is associated with significantly higher odds of MACE and stroke, even after adjusting for baseline imbalances between cohorts using propensity-matched analyses. These conclusions are strengthened by the relative size of the prospective ACS-NSQIP targeted registry being studied (rivaling the prespecified combined analysis of the Endarterectomy versus Angioplasty in Patients with Symptomatic Severe Carotid Stenosis [EVA-3S], Stent-Protected Angioplasty versus Carotid Endarterectomy [SPACE], and International Carotid Stenting Study [ICSS] trials by the Carotid Stenosis Trialists Collaboration)12 and are in keeping with data from the Vascular Quality Initiative regarding variations in EPD use during CAS,21 despite its efficacy.22 These findings imply that a substantial portion of CAS remains unprotected (despite the consequences), a practice pattern that runs counter to the 2011 multisociety consensus guidelines, noting the benefit of EPD during CAS,4 and to the directions from the US Centers for Medicare and Medicaid Services,23 which list intraprocedural use of an EPD as a necessary condition for reimbursement of CAS.
The reasons for lack of EPD use in approximately one-quarter of CAS cases in the ACS-NSQIP targeted registry are unclear and do not appear to be explained by any differences in anatomic high-risk factors in patients undergoing CAS with or without EPD. One potential reason may be that while EPD use during CAS has been favored in a number of meta-analyses6,7 and national data base reviews,8 definitive evidence has not emerged from more recent randomized trials to support its use. For example, of the 5 major recent carotid revascularization trials comparing carotid endarterectomy with CAS, only 2 (Carotid Revascularization Endarterectomy versus Stenting Trial [CREST]24 and Asymptomatic Carotid Trial [Randomized Trial of Stent versus Surgery for Asymptomatic Carotid Stenosis - ACT I]25) mandated EPD use with CAS. Of the remaining 3, the SPACE trial found no difference in 30-day ipsilateral stroke or death in patients undergoing CAS with and without an EPD (8.3% versus 6.2%; P = .40),26 and the ICSS trial found a trend toward more MACE after CAS with an EPD (8.5% versus 4.6%; P = .056).27 Only the EVA-3S trial found EPD use to be associated with fewer strokes or death (7.9% versus 20.6%; relative risk, 0.38; 95% CI, 0.17–0.85), though this trial was criticized for higher complication rates and operator inexperience.28 Finally, a prespecified pooled analysis of individual patient data from 3 trials (SPACE, EVA-3S, ICSS) found stroke and death after CAS to be related to stent cell design and unrelated to EPD, even after adjusting for age, qualifying event, history of prior stroke, baseline disability, and operator experience.11 Use of DWI as a surrogate measure of EPD efficacy has also not yielded evidence in favor of its use, with the ICSS trial finding more ischemic brain lesions on MR imaging after CAS with-versus-without an EPD (68% versus 35%; P = .003)29 and Barbato et al11 similarly finding more DWI lesions in patients having undergone CAS randomized to EPD versus to no EPD.
How EPD may counterintuitively increase stroke risk during CAS or lead to more ischemic changes on MR imaging has not been fully explained. Thrombus may form on the distal filter surface, on the tip of the EPD wire, or from microtrauma to the vascular wall and plaque during EPD placement, and microemboli may pass through the micropores of the EPD or through gaps that exist between the EPD and the vascular wall.30 Other challenges related to use of an EPD during CAS may be the additional technical difficulty of EPD navigation and placement, especially in severely stenotic and/or highly tortuous anatomy. To overcome some of these issues, a variety of EPDs have been developed to improve the safety of CAS, including proximal protection devices represented by proximal balloon occlusion and flow-reversal devices.31 Nevertheless, even CAS using proximal protection with flow reversal has been associated with DWI lesions, though fewer than those seen with traditional distal EPDs.32
Given the above discussion, our finding that CAS without EPD is associated with a significantly higher risk of stroke and MACE (in both primary and matched-cohort analyses), while intuitive, may still come as a surprise. For example, a prior analysis of ACS-NSQIP did not find any significant differences in the number of major adverse events between CAS with and without an EPD.33 However, the time span of this prior study (4 years) was much shorter than that in our dataset, and it is likely that our use of the largest targeted ACS-NSQIP dataset available to date may have accounted for our positive results. Most important, none of the prior studies randomized patients to EPD use, raising concern for potential confounding differences between cohorts with and without EPD that might mask significant differences despite multivariable regression analysis. For example, patients without an EPD in the ACS-NSQIP were more likely to have CAS performed emergently and less likely to have had preoperative antiplatelets. We, therefore, further adjusted for potential confounding differences between cohorts with EPD and without EPD by use of propensity score matching, which further confirmed the increased risk of stroke and MACE seen after CAS without EPD on our primary multivariable analysis.
There are limitations to our study, most important, that multivariable analysis, with or without propensity score matching, cannot eliminate biases inherent in retrospective data base analysis or replace a prospective randomized trial of CAS with or without EPD. However, it appears increasingly unlikely that such a trial will ever be undertaken, and prospective registries such as ACS-NSQIP, while not as comprehensive as desired, may be the next best alternative to randomized trial data. Nevertheless, the ACS-NSQIP does not provide granular periprocedural data that would permit analysis of factors such as the etiology of stenosis or the use of pre-/postangioplasty during CAS. Similarly, the ACS-NSQIP data base may not be representative of national practice, but it does identify periprocedural stroke more accurately than national administrative datasets.14 Last, the ACS-NSQIP study population is largely from CAS using a distal rather than proximal EPD, and transcarotid artery revascularization was not part of this dataset. Use of transcarotid artery revascularization has been associated with exceptionally low rates of stroke and death after CAS in the Vascular Quality Initiative,34 and increased use of proximal protection and/or flow-reversal techniques may further increase the performance gap between CAS with and without an EPD in the future.
CONCLUSIONS
Analysis of the vascular-targeted ACS-NSQIP data base reveals that nearly one-quarter of CAS is performed without an EPD. This has not significantly changed between 2011 and 2018 and is associated with a more than a 2-fold increase in the likelihood of MACE, and a 4-fold increase in the likelihood of periprocedural stroke. Quality improvement efforts targeting increased use of an EPD during CAS may, therefore, yield substantial benefit toward patient outcomes.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received December 15, 2020.
- Accepted after revision January 26, 2021.
- © 2021 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}