
Abstract
BACKGROUND AND PURPOSE: Severe respiratory distress in patients with COVID-19 has been associated with higher rate of neurologic manifestations. Our aim was to investigate whether the severity of chest imaging findings among patients with coronavirus disease 2019 (COVID-19) correlates with the risk of acute neuroimaging findings.
MATERIALS AND METHODS: This retrospective study included all patients with COVID-19 who received care at our hospital between March 3, 2020, and May 6, 2020, and underwent chest imaging within 10 days of neuroimaging. Chest radiographs were assessed using a previously validated automated neural network algorithm for COVID-19 (Pulmonary X-ray Severity score). Chest CTs were graded using a Chest CT Severity scoring system based on involvement of each lobe. Associations between chest imaging severity scores and acute neuroimaging findings were assessed using multivariable logistic regression.
RESULTS: Twenty-four of 93 patients (26%) included in the study had positive acute neuroimaging findings, including intracranial hemorrhage (n = 7), infarction (n = 7), leukoencephalopathy (n = 6), or a combination of findings (n = 4). The average length of hospitalization, prevalence of intensive care unit admission, and proportion of patients requiring intubation were significantly greater in patients with acute neuroimaging findings than in patients without them (P < .05 for all). Compared with patients without acute neuroimaging findings, patients with acute neuroimaging findings had significantly higher mean Pulmonary X-ray Severity scores (5.0 [SD, 2.9] versus 9.2 [SD, 3.4], P < .001) and mean Chest CT Severity scores (9.0 [SD, 5.1] versus 12.1 [SD, 5.0], P = .041). The pulmonary x-ray severity score was a significant predictor of acute neuroimaging findings in patients with COVID-19.
CONCLUSIONS: Patients with COVID-19 and acute neuroimaging findings had more severe findings on chest imaging on both radiographs and CT compared with patients with COVID-19 without acute neuroimaging findings. The severity of findings on chest radiography was a strong predictor of acute neuroimaging findings in patients with COVID-19.
ABBREVIATIONS:
- CCS
- Chest CT Severity
- COVID-19
- coronavirus disease 2019
- ICU
- intensive care unit
- PXS
- Pulmonary X-ray Severity
- ROC
- receiver operating characteristic
- SARS-CoV-2
- Severe Acute Respiratory Syndrome coronavirus 2
The Severe Acute Respiratory Syndrome coronavirus 2 (SARS-CoV-2), which causes coronavirus disease 2019 (COVID-19), has now infected >40 million people worldwide, with >1 million deaths reported by the end of October 2020.1 While COVID-19 is well-known for its pulmonary manifestations, it has been shown to involve other organs, including the heart, kidneys, liver, and central nervous system.2⇓⇓-5 This involvement is consistent with viral entry through the angiotensin-converting enzyme 2 receptor, which is abundantly expressed on vascular endothelial cells of the lungs but also in other organs, including the central nervous system, heart, kidneys, intestines, and muscles.6 Reported neurologic manifestations of COVID-19 infection include ischemic and hemorrhage stroke, encephalitis, and leukoencephalopathy.7⇓⇓⇓⇓-12
It has been previously reported that patients with COVID-19 and severe respiratory distress have a relatively high rate of neurologic involvement.13 Furthermore, patients with COVID-19 and neurologic symptoms have been shown to have poorer outcomes than those without them.14 Thus, it would be important to identify clinical or imaging features in patients with COVID-19 that may help predict an increased risk of neurologic injury. Severity of disease on chest imaging is a strong predictor of clinical outcome and risk of complications.15⇓-17 The objective of our study was to identify whether the severity of chest imaging findings is correlated with the risk of positive neuroimaging findings in patients admitted for COVID-19 infection.
MATERIALS AND METHODS
Study Cohort
This retrospective study was approved by Massachusetts General Hospital institutional review board of our institution with a waiver of informed consent, and patient privacy was ensured in compliance with the Health Insurance Portability and Accountability Act. Between March 3, 2020, and May 6, 2020, a total of 641 patients received medical care at our quaternary care academic medical center for COVID-19. Patients were included if they tested positive for SARS-CoV-2 infection diagnosed via real-time polymerase chain reaction, underwent CT and/or MR imaging for the evaluation of neurologic symptoms, and underwent chest radiography and/or CT within 10 days of neuroimaging for pulmonary symptoms. Patients were excluded if their neuroimaging was affected by substantial artifacts that precluded diagnostic assessment.
Clinical Data
Basic demographic information, including age and sex, as well as indications for neuroimaging were obtained from the electronic medical record for each patient. Clinical data, including length of hospital stay, admission to intensive care unit, intubation status, and death, were obtained for each patient.
Imaging Technique
All neuroimaging CT examinations were obtained on 64–section multidetector row CT scanners, either a Revolution CT (GE Healthcare) or a Somatom Force CT (Siemens) scanner. For non-contrast-enhanced head CTs, the studies were axially acquired (120 kV/auto-milliampere-seconds) at 5- and 1.25-mm-thick slices, from the level of the skull base to the vertex. For MR brain imaging, sequences performed included axial DWI, axial T2 FLAIR, axial T2WI, axial SWI, and sagittal T1WI. Intravenous contrast was used in a subset of studies.
All patients included in the study underwent portable chest radiography within 10 days before neuroimaging. The chest radiograph with the highest severity (highest Pulmonary X-ray Severity [PXS] score) within 10 days before neuroimaging was used for analysis (a mean of 3.3 [SD, 3.3] days for patients with acute neuroimaging findings versus a mean of 1.8 [SD, 3.7] days for patients without acute neuroimaging findings, P = .18).
Chest CT was performed in a subset of patients during admission and within 10 days before neuroimaging (a mean of 2.2 [SD, 2.9] days for patients with acute neuroimaging findings versus a mean of 1.5 [SD, 2.6] days for patients without acute neuroimaging findings, P = .40). The images were obtained with the patient in the supine position using one of the following CT scanners: Discovery CT750 HD (GE Healthcare), Revolution Frontier (GE Healthcare), Somatom Definition Flash (Siemens), Somatom Definition AS (Siemens), Somatom Force (Siemens), and Aquilion ONE (Toshiba). The scanning parameters were the following: tube voltage = 140 kV(peak) (plus 80 kVp for dual energy), matrix = 512 × 512, section thickness = 1.25 mm, FOV = 440 × 440 mm.
Image Evaluation
All neuroimaging examinations included in this study were reviewed by 2 fellowship-trained neuroradiologists, and the presence of intracranial hemorrhage, acute or subacute infarction, and/or leukoencephalopathy was recorded.
Portable chest radiographs for each patient were assessed using a previously validated convolutional Siamese neural network–based approach for automated assessment of COVID-19 lung disease severity, called the PXS score.16,18 Briefly, this machine learning model takes pixel-level image data from frontal chest radiographs as input and outputs a quantitative score for parenchymal lung disease severity. This score has previously been shown to correlate with manual radiologic assessments of COVID-19 radiographic severity as well as clinical outcome. A PXS score of ≤2.5 indicates no or minimal disease; > 2.5 and ≤5.0, mild disease; >5.0 and ≤9.0, moderate disease; and >9.0, severe disease.16,18
Chest CT severity was assessed by 3 fellowship-trained thoracic radiologists on the basis of a previously published grading system, the Chest CT Severity (CCS) score.19 Briefly, the 5 lung lobes were assessed individually for the degree of involvement by ground-glass opacities and consolidation. A score of 0 indicates no involvement; 1, minimal involvement (1%–25%); 2, mild involvement (26%–50%); 3, moderate involvement (51%–75%); and 4, severe involvement (76%–100%). The summation of the individual lobe scores yields the total CCS score.
Statistical Analysis
Statistical analysis was performed using GraphPad Prism software (GraphPad Software) and R Studio (http://rstudio.org/download/desktop). Continuous data were presented as means [SD] and were analyzed by a 2-tailed t test; categoric data were presented as frequency (%) and analyzed with a χ2 test. Associations between the lung disease severity scores (PXS and CCS) and neuroimaging findings were examined using multivariable logistic regression. Models were risk-adjusted for age, sex, the need for intubation, and intensive care unit (ICU) admission. The R Studio package pROC (https://www.rdocumentation.org/packages/pROC/versions/1.16.2) was used to generate receiver operating characteristic (ROC) curves and to calculate the area under the ROC curve.20 We computed 95% confidence intervals with 2000 stratified bootstrap replicates. Statistical significance was set at P < .05.
RESULTS
A total of 93 patients met the inclusion criteria for the study. Twenty-four (26%) patients had acute neuroimaging findings, whereas 69 (74%) patients did not. The proportion of patients who underwent MR imaging or CT was not significantly different between patients without acute neuroimaging findings (58 underwent head CT and 11 underwent brain MR imaging) and patients with acute neuroimaging findings (18 underwent head CT and 6 underwent brain MR imaging; P = .36). The mean age of patients without acute neuroimaging findings was 66 [SD, 16] years of age, 33% of whom were women. The mean age for patients with acute neuroimaging findings was 63 [SD, 16] years, 33% of whom were women as well. The most common indication for neuroimaging was altered mental status and concern for stroke for patients with and without neuroimaging findings (Table 1).
Summary of patient characteristics, clinical data, and indication for neuroimaging
The average length of hospital stay was significantly longer in patients with acute neuroimaging findings (31 [SD, 12] days versus 23 [SD, 15] days, P = .021; Table 1). In addition, the prevalence of ICU admission and intubation was significantly higher for patients with acute neuroimaging findings than for patients without acute neuroimaging findings (92% versus 67%, P = .04%, and 88% versus 52%, P = .005, respectively; Table 1). The mortality rate, however, was not significantly different between patients without acute neuroimaging findings (17%) and patients with acute neuroimaging findings (21%, P = .945).
Of the 24 patients with acute neuroimaging findings, 7 patients were found to have intracranial hemorrhage (Fig 1), 7 patients were found to have acute infarction (Fig 2), 6 patients were found to have leukoencephalopathy (Fig 3), 3 patients had intracranial hemorrhage and infarction, and 1 patient had intracranial hemorrhage, infarction, and leukoencephalopathy (Table 2). Sixty-nine patients did not have acute neuroimaging findings (Fig 4). There was no significant difference (P = .225) between the distribution of Radiological Society of North America categories of chest CT findings between patients without acute neuroimaging findings (n = 66) and those with acute neuroimaging findings (n = 14), with the “typical” category being the most prevalent in both groups (Table 2).21

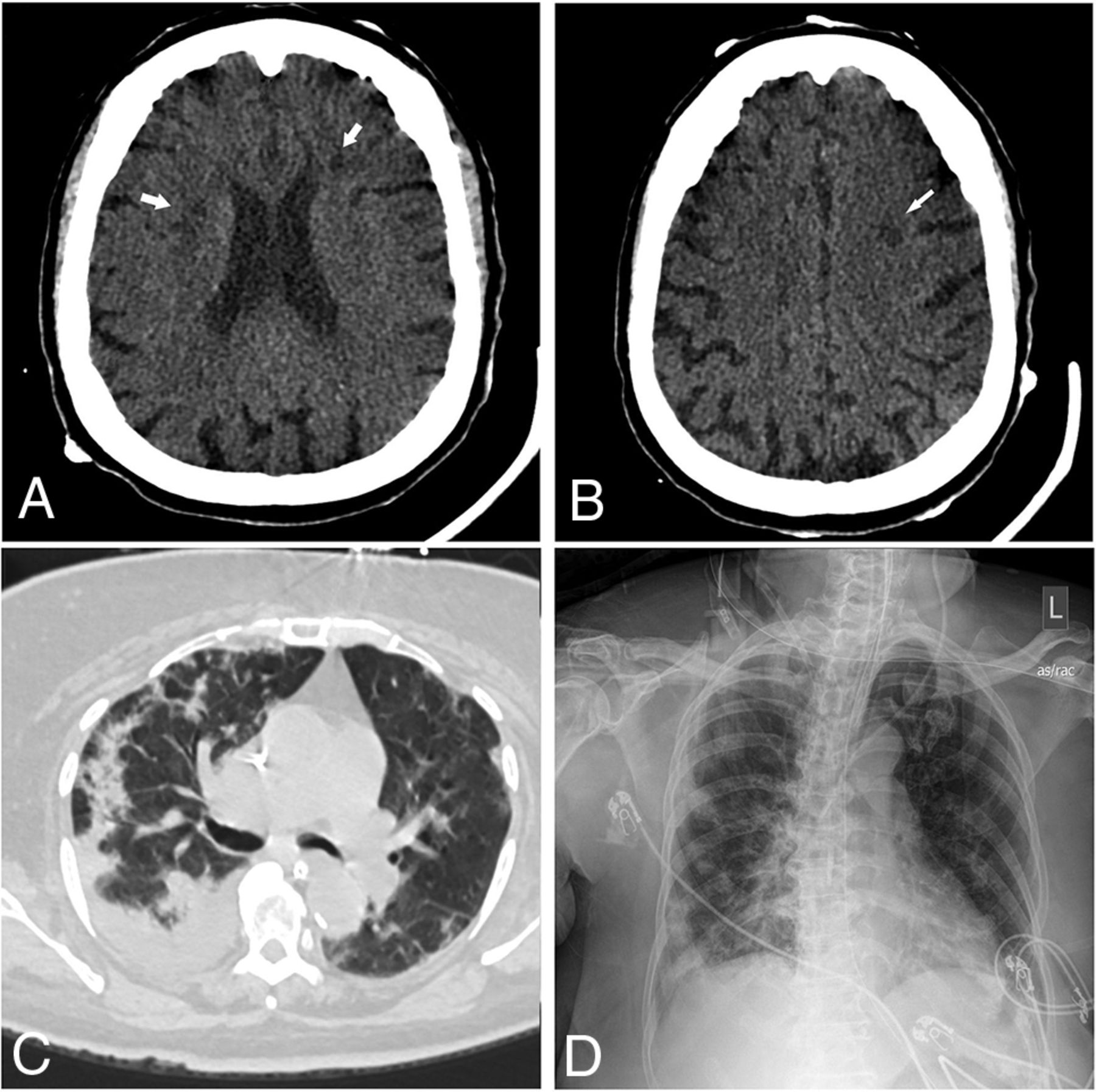
A 42-year-old man presented with hypoxemic respiratory failure. Non-contrast-enhanced axial (A) and coronal (B) CT head images demonstrate a new, large, right cerebellar intraparenchymal mixed-attenuation hematoma suggestive of hyperacute or active hemorrhage. C, Chest CT of the patient demonstrates bilateral consolidation and ground-glass opacities involving all lobes, with a CCS score of 18. D, Portable chest radiograph demonstrates bilateral patchy air space opacities with a PXS score of 10.3.

An 85-year-old man presented with increasing shortness of breath. Non-contrast-enhanced axial CT of the head demonstrates multiple new foci of hypoattenuation within the bilateral frontal corona radiata (arrows on A) and left centrum semiovale (arrow on B), in keeping with acute infarcts. C, Chest CT of the patient shows diffuse bilateral, right greater-than-left, predominantly consolidation and ground-glass opacities as well as bilateral pleural effusions. The CCS score was calculated as 13. D, Portable chest radiograph demonstrates bilateral patchy opacities with a PXS score of 10.6.

A 64-year-old man presented with fever and shortness of breath. Axial FLAIR (A) and diffusion-weighted (B) images demonstrate extensive symmetric confluent T2/FLAIR signal abnormality and restricted diffusion involving the corona radiata bilaterally. C, Chest CT shows bilateral peripheral ground-glass opacities and a small amount of consolidation involving all lobes, with a CCS score of 15. D, Portable chest radiograph demonstrates bilateral lower-zone-predominant peripheral opacities with a PXS score of 8.8.

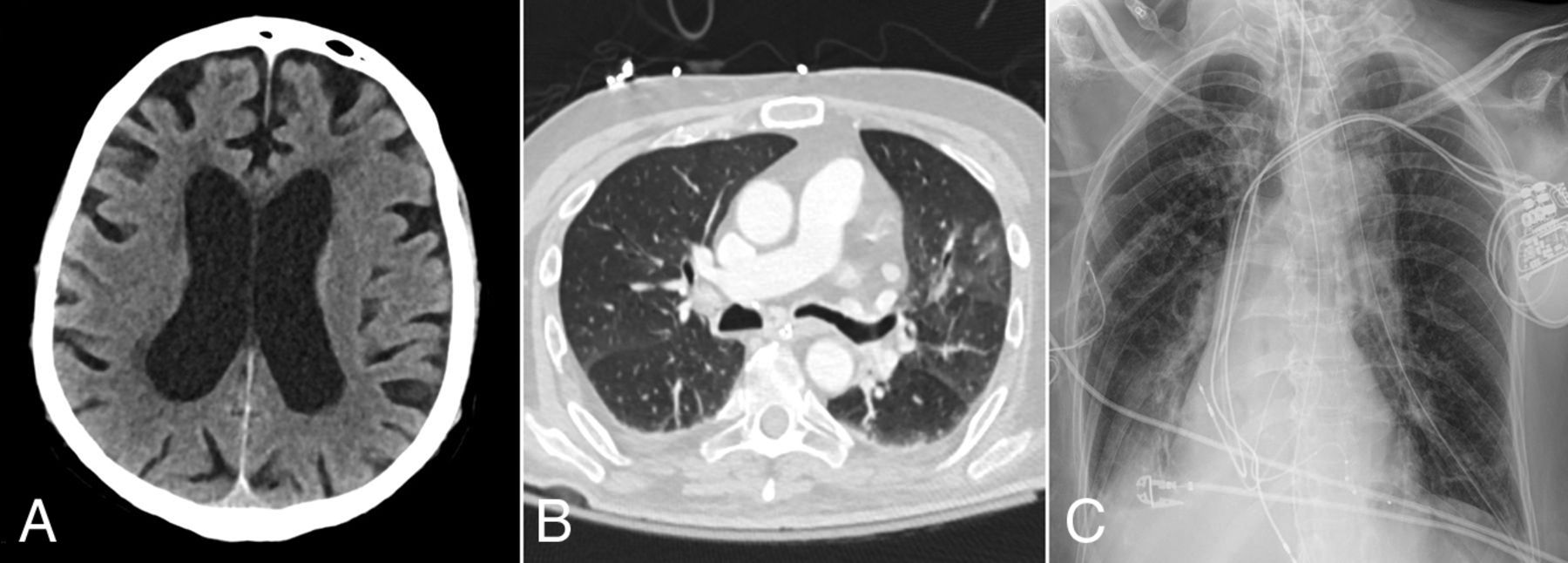
A 67-year-old woman presented with hypoxemic respiratory failure. Axial non-contrast-enhanced head CT image (A) shows no acute findings. B, Chest CT image of the patient demonstrates bilateral peripherally distributed ground-glass opacities involving 4 of the 5 lobes with a CCS score of 8. D, Portable chest radiograph demonstrates bibasilar patchy opacities with a PXS score of 4.4.
Distribution of neuroimaging findings and RSNA categories
The mean PXS score was significantly greater in patients with acute neuroimaging findings (n = 23, 9.2 [SD, 3.4]) than in patients without acute neuroimaging findings (n = 64, 5.0 [SD, 2.9], P < .001; Fig 5A). The PXS score was a significant predictor of positive acute neuroimaging findings in patients with COVID-19 after adjusting for age, sex, ICU admission, and intubation status (odds ratio = 1.45, P < .001; Fig 6). The mean CCS score was also significantly greater in patients with acute neuroimaging findings (n = 14, 12.1 [SD, 5.0]) than in patients without acute neuroimaging findings (n = 64, 9.0 [SD, 5.1], P = .041; Fig 5B). However, after we adjusted for age, sex, ICU admission, and intubation status, the CCS score was not a significant predictor of positive acute neuroimaging findings in patients with COVID-19 (odds ratio = 1.08, P = .308; Fig 6).

A, Comparison of portable chest radiograph severity (PXS) score between patients with and without acute neuroimaging findings. B, Comparison of the CCS score between patients with and without acute neuroimaging findings.

Odds ratio of the PXS score and the CCS score in association with the risk of acute neuroimaging findings. A multivariate logistic regression model was used after adjusting for age, sex, the need for intubation, and ICU admission status.
The area under the ROC curve using the PXS score to classify acute neuroimaging findings was 0.83 (95% CI, 0.72–0.93; Fig 7A). The optimal threshold PXS score was 7.55, which corresponded to a sensitivity of 83%, specificity of 81%, positive likelihood ratio of 4.7, and negative likelihood ratio of 0.2. By means of this threshold, meaning scores of ≥7.6 were labeled as positive for acute neuroimaging findings and scores of ≤7.5 were labeled as negative for acute neuroimaging findings, 77% of cases in our study would be correctly classified.

ROC curves of the PXS and CCS scores to classify acute neuroimaging findings in patients with COVID-19. A, The area under the ROC curve using the PXS score to classify acute neuroimaging findings was 0.83 (95% CI, 0.72–0.93). The optimal threshold PXS score was 7.55, which corresponded to a sensitivity of 83%, specificity of 81%, positive likelihood ratio of 4.7, and negative likelihood ratio of 0.2. B, The area under the ROC curve using the CCS score to classify acute neuroimaging findings was 0.67 (95% CI, 0.50–0.84). The optimal threshold CCS score was 12.5, which corresponded to a sensitivity of 64%, specificity of 73%, positive likelihood ratio of 2.4, and negative likelihood ratio of 0.5.
The area under the curve using the CCS score to classify acute neuroimaging findings was 0.67 (95% CI, 0.50–0.84; Fig 7B). The optimal threshold CCS score was 12.5. This threshold corresponded to a sensitivity of 64%, specificity of 73%, positive likelihood ratio of 2.4, and negative likelihood ratio of 0.5. By means of this threshold, meaning scores of ≥13 were labeled as positive for acute neuroimaging findings and scores of ≤12 were labeled as negative for acute neuroimaging findings, 61% of cases in our study would be correctly classified.
DISCUSSION
A variety of neuroimaging findings have been reported in patients with COVID-19, including infarction, intracranial hemorrhage, leukoencephalopathy, and hemorrhagic encephalitis.8⇓⇓-11,14,22 The presence of acute-to-subacute neuroimaging findings in patients with COVID-19 is associated with a higher risk of ICU admission, intubation, and mortality.14 However, the risk factors for developing neurologic deficits in patients with COVID-19 are unclear. The results of this retrospective study showed that the severity of disease on chest radiographs and chest CT images was significantly greater among patients with COVID-19 with acute neuroimaging findings than in patients without acute neuroimaging findings, suggesting that more severe pulmonary manifestations are associated with a higher likelihood of neurologic injury.
Similar to prior reports, the presence of acute neuroimaging findings in our study was associated with an increased length of hospital stay, increased risk of requiring ICU admission, and risk of intubation.14,23 Acute ischemic and hemorrhagic strokes, the most common neuroimaging manifestation, have been reported to be a strong prognostic maker for poor clinical outcome in patients with COVID-19.14 While ischemic and hemorrhagic strokes were also the most common neuroimaging findings in our study population, mortality was not significantly different between patients with acute neuroimaging findings and those without them. The small number of patients with acute neuroimaging findings may be underpowered to detect a statistically significant difference.
Respiratory symptoms are the most common manifestations of COVID-19, and extensive research has been performed on chest imaging features of the disease, including using chest radiograph and chest CT severity as a prognostic tool for clinical outcome.16,19,24⇓⇓⇓⇓-29 A study by Mao et al13 has also demonstrated high rates of neurologic symptoms in patients with COVID-19 and severe respiratory disease. This outcome may be due to shared mechanisms, including cytokine-related abnormal inflammatory response, coagulopathy, and micro- and macroangiopathy, which contribute to both chest and neuroimaging findings in patients with COVID-19.28⇓⇓⇓⇓⇓-34 Both chest and neuroimaging manifestations, however, are unlikely due to a single etiology but rather a combination of interconnected pathophysiologic processes. The greater severity of chest imaging findings may therefore indicate more severe system-wide pathology, in which case-heightened suspicion for acute neurologic injury is warranted. Consistent with this theory, PXS scores of patients with COVID-19 were found to be significantly associated with an increased risk of acute neuroimaging findings in our study. While a higher CCS score was associated with an increased risk of acute neuroimaging findings in the current study, this did not reach statistical significance. This may be related to the small number of patients who underwent chest CT relative to the number of patients who underwent chest radiographic assessment. Future investigation with a larger patient cohort is needed.
Three patients in the current study who had minimal-to-mild chest radiographic findings were found to have either infarction or intracranial hemorrhage. Similarly, 3 patients with mild disease on chest CT were found to have infarction, hemorrhage, and leukoencephalopathy on neuroimaging. The cause of neurologic injury in these patients may be better explained by direct neurotropism of the SARS-CoV-2 virus, which may occur through retrograde transmission through peripheral nerve terminals including the olfactory nerves, rather than widespread cytokine storm.35,36 Other proposed mechanisms of neurologic injury without severe chest imaging manifestations include silent hypoxia, metabolic disturbances, neuroinflammation, angiopathy, embolic phenomenon, or an autoimmune-mediated process.37⇓⇓-40 While neurologic injury can occur in patients with mild pulmonary disease and with less evident chest imaging findings, the relative proportion of these patients is much smaller than those with more severe pulmonary findings.
Limitations of the current study include its retrospective nature and relatively small sample size from a single institution. The small number of patients also precluded further analysis of the risk of developing different types of neurologic injury, such as infarction, hemorrhage, or leukoencephalopathy. Furthermore, additional patient information including laboratory values and comorbidities was incomplete and therefore was not included in the study. Finally, most of these patients did not have additional imaging of other body parts, including the abdomen and pelvis, limiting correlation of findings in other organ systems.
CONCLUSIONS
Patients with COVID-19 and acute neuroimaging findings had greater disease severity on both chest radiography and CT than patients without acute neuroimaging findings. In our adjusted regression models, chest radiograph severity was a strong predictor of acute neuroimaging findings in patients with COVID-19, while the small number of patients may have underpowered the study to detect a significant correlation with chest CT. Therefore, a high severity of disease on chest imaging should raise suspicion for neurologic injury in patients with COVID-19. Early use of neuroimaging in these patients should be considered.
Footnotes
B.P. Little and K. Buch are equal co-senior authors.
This study was supported by sundry funds to J. Kalpathy-Cramer. This research was carried out, in whole or in part, at the Athinoula A. Martinos Center for Biomedical Imaging at the Massachusetts General Hospital, using resources provided by the Center for Functional Neuroimaging Technologies, P41EB015896, a P41 Biotechnology Resource Grant supported by the National Institute of Biomedical Imaging and Bioengineering, National Institutes of Health. GPU computing resources were provided by the MGH and BWH Center for Clinical Data Science.
Disclosures: Matthew D. Li—UNRELATED: Grants/Grants Pending: Radiological Society of North America, Comments: M.D.L. reports funding from a Radiological Society of North America Research and Education Presidents Circle Research Resident Grant, outside of the submitted work.* Efren J. Flores—UNRELATED: Grants/Grants Pending: National Cancer Institute Research Diversity Supplement, American College of Radiology Innovation Fund. William A. Mehan, Jr—UNRELATED: Consultancy: Kura Oncology, Comments: independent reviewer of imaging for a head and neck cancer trial; Employment: Massachusetts General Hospital; Expert Testimony: expert opinion for medicolegal cases involving neuroimaging. Susie Y. Huang—UNRELATED: Grants/Grants Pending: Siemens, Comments: research grant for clinical translation of fast brain MRI sequences*; Payment for Lectures Including Service on Speakers Bureaus: Siemens, Comments: payment for speaking on Connectome 2.0 at OHBM 2020. Jayashree Kalpathy-Cramer—UNRELATED: Grants/Grants Pending: GE Healthcare, Genentech Foundation*; Travel/Accommodations/Meeting Expenses Unrelated to Activities Listed: IBM. Brent P. Little—UNRELATED: Royalties: Elsevier, Comments: textbook royalties, chest radiology textbook, author/associate editor. *Money paid to the institution.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received November 8, 2020.
- Accepted after revision December 11, 2020.
- © 2021 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.