
Abstract
BACKGROUND AND PURPOSE: Chronic subdural hematoma embolization, an apparently simple procedure, can prove to be challenging because of the advanced age of the target population. The aim of this study was to compare 2 arterial-access strategies, femoral versus patient-tailored CTA-based frontline access selection, in chronic subdural hematoma embolization procedures.
MATERIALS AND METHODS: This was a monocentric retrospective study. From the March 15, 2018, to the February 14, 2019 (period 1), frontline femoral access was used. Between February 15, 2019, and March 30, 2020 (period 2), the choice of the frontline access, femoral or radial, was based on the CTA recommended as part of the preoperative work-up during both above-mentioned periods. The primary end point was the rate of catheterization failure. The secondary end points were the rate of access site conversion and fluoroscopy duration.
RESULTS: During the study period, 124 patients (with 143 chronic subdural hematomas) underwent an embolization procedure (mean age, 74 [SD, 13] years). Forty-eight chronic subdural hematomas (43 patients) were included during period 1 and were compared with 95 chronic subdural hematomas (81 patients) during period 2. During the first period, 5/48 (10%) chronic subdural hematoma embolizations were aborted due to failed catheterization, significantly more than during period 2 (1/95, 1%; P = .009). The rates of femoral-to-radial (P = .55) and total conversion (P = .86) did not differ between the 2 periods. No significant difference was found regarding the duration of fluoroscopy (P = .62).
CONCLUSIONS: A CTA-based patient-tailored choice of frontline arterial access reduces the rate of catheterization failure in chronic subdural hematoma embolization procedures.
ABBREVIATIONS:
- CSDH
- chronic subdural hematoma
- MMA
- middle meningeal artery
The annual incidence of chronic subdural hematomas (CSDHs), 14 to 20 per 100,000 individuals, means that the condition is one of the most frequently managed by neurosurgery departments.1,2 CSDHs are thought to be sentinel health events, akin to hip fractures, with important reduction in life expectancy for patients compared with age-matched controls.3 The condition is, moreover, associated with far-from-negligible rates of morbidity and mortality, around 11% and 4%, respectively.4
Standard management of symptomatic CSDHs includes surgical evacuation, mostly through twist drill or burr-hole craniostomy with closed-system drainage.4⇓-6 Recently, middle meningeal artery (MMA) embolization has emerged as a possible treatment of CSDHs.7,8 The procedure is simple in appearance but can prove to be challenging in a subset of patients because of tortuous vasculature. Indeed, CSDH is mostly a disease of the elderly with two-thirds of cases accounted for in patients older than 65 years of age.1 In the elderly, several factors, including peripheral vascular disease and vascular anatomy, can complicate or even preclude cervical vessel navigation by a traditional transfemoral approach.9,10
The transradial approach has recently emerged as an alternative to transfemoral access in interventional neuroradiology, with the stated aim of reducing access-related complications and patient discomfort.11 It has also been envisioned that radial access may facilitate anterior circulation navigation in some patients.10,11 The aim of this study was to compare 2 arterial-access strategies, frontline femoral versus patient-tailored frontline access selection (femoral or radial), based on a preoperative CTA, in CSDH embolization procedures.
MATERIALS and METHODS
Study Design
This was a monocentric retrospective study performed in a tertiary care and teaching hospital. Starting from March 15, 2018, CSDH has been proposed as a treatment of CSDH, initially as an adjunct to surgery and more recently as a possible sole treatment in a minority of patients. The most common indication for CSDH embolization at our institution is a CSDH recurrence or a CSDH with an independent recurrence risk factor, including antiplatelet therapy, anticoagulation therapy, hepatopathy, or alcohol abuse, for instance.12 Eligible patients were excluded if they refused the embolization procedure or were denied embolization by the attending physician because they presented in a moribund state, had a contraindication to the embolization procedure like severe renal dysfunction, or had a life expectancy of <6 months. A pre-embolization aortic arch and supra-aortic trunk CTA was recommended to rule out anatomic contraindications. The choice of the MMA embolization technique was left to the discretion of the attending interventional neuroradiologist.
From March 15, 2018, to February 14, 2019 (period 1), a femoral access was systematically used as a frontline strategy for CSDH embolization, in line with wider institutional habits. On the basis of this initial experience, from February 15, 2019, to March 30, 2020 (period 2), the choice of the arterial frontline access, femoral or radial, was patient-tailored and based on the available CTA. The choice of frontline access was left to the discretion of the attending interventional neuroradiologist. Radial frontline access was, nevertheless, strongly recommended for right carotid catheterization in case of a type III aortic arch with proximal common carotid artery tortuosity and for left carotid navigation in case of a bovine arch configuration.10,11 For radial access (up to 6F sheaths), micropuncture under sonographic guidance was preferred, without prior testing of collateral circulation. Intra-arterial injection of verapamil (3 mg) through the sheath was performed. Given the context of intracranial hemorrhage, radial access in this specific setting was usually performed without anticoagulation. Postprocedure, patent hemostasis for 2 hours was recommended. No left radial or distal radial access was used in this series.
Demographic and clinical data were retrieved by retrospective review of patient medical records. Imaging data were analyzed on the local PACS.
End Points
The primary end point was the rate of catheterization failure leading to procedure abortion. The secondary end points were rate of access site conversion and fluoroscopy duration. Because some procedures were performed in a biplane angiosuite while others were performed in a monoplane angiosuite, only the fluoroscopy duration of the anterior-posterior plane was considered for biplane procedures.
Statistical Analysis
Data are expressed as a percentage for binary variables and as mean [SD] for continuous variables. Probability values are provided uncorrected. Probability values < .05 were considered significant. A χ2 test was used to compare frequencies, and comparison of means was performed using a Student t test. Statistical analyses were performed using MedCalc, Version 19.2 (MedCalc Software).
Ethical Statement
The institutional review board approved this study (Comité d’Ethique pour la Recherche en Imagerie Médicale CRM-2003–063) and the need for signed patient consent was waived.
Data-Sharing Statement
Raw data are available on reasonable request from the corresponding author.
RESULTS
Population Characteristics
One hundred thirty-eight patients were referred for MMA embolization during the study period (Fig 1). Six patients were deemed unfit to undergo embolization, and another 6 patients refused to undergo the procedure. Two patients were excluded on the basis of the result of the CTA because of extensive supra-aortic trunk atheroma precluding safe endovascular navigation. A total of 124 patients underwent embolization procedures of 143 target MMAs (105 unilateral and 19 bilateral CSDHs). The mean age of the study population was 74 [SD, 13] years, and most of the patients (94; 76%) were men. There was no difference in terms of demographics, clinical and radiologic presentation of the CSDHs, management strategy, and choice of anesthesia technique between patients managed during periods 1 and 2 (Table 1).

Flow chart. E° indicates embolization.
Patient characteristicsa
Embolization Procedures
During period 1, all 48 CSDH embolizations were performed via a frontline femoral access. In 1 instance (2%), a femoral-to-radial conversion was deemed necessary during the procedure (Fig 2, illustrative example C). During period 2, a frontline femoral access was chosen for 57/95 (60%) CSDH embolizations. Of these, a femoral-to-radial conversion was deemed necessary during the procedure in 1/57 (2%) instances (Fig 2, illustrative example D). Conversely, a frontline radial access was chosen for 38/95 (40%) cases with 3/38 (8%) radial-to-femoral per-procedure conversions. Figure 2 shows a series of anatomic configurations having led to difficult endovascular navigation or catheterization failure.

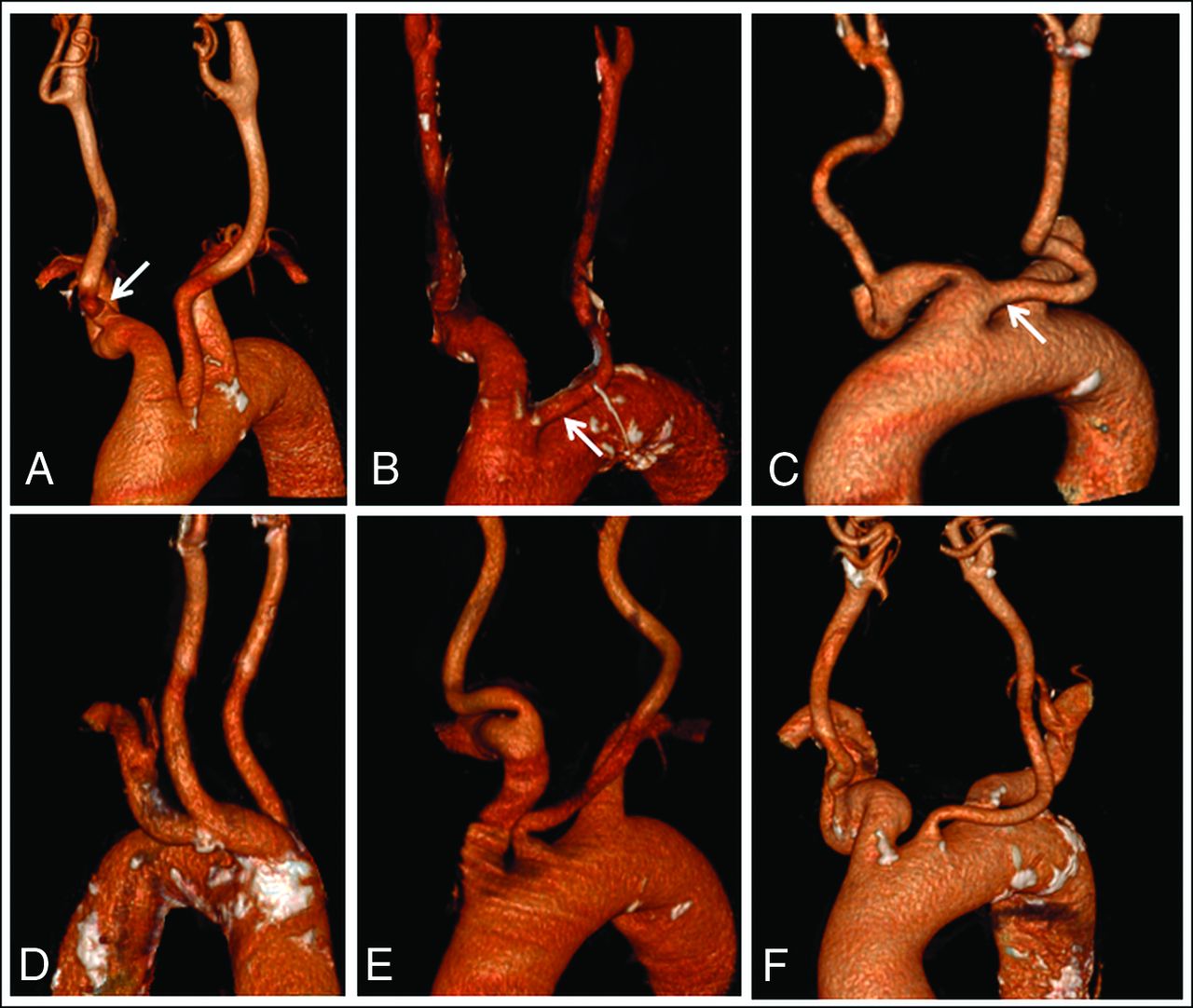
Illustrative examples of challenging and failed catheterization cases. Manually-segmented surface-rendering 3D reconstructions of CTAs of aortic arches of patients included during periods 1 (A–C) and 2 (D–F). A, Anterior view of a case of failed right carotid catheterization by femoral access due to a proximal kinking of the right common carotid artery (right arrow) in a type III aortic arch. B, Anterior view in a case of failed left carotid catheterization by femoral access due to a bovine arch configuration (right arrow), which, in retrospect, would have been an ideal candidate for radial access. C, Anterior view in a case of failed left carotid catheterization by femoral access converted secondarily to transradial catheterization in relation to a bovine arch (right arrow). D, Posterior view of a case of failed right carotid catheterization by a frontline femoral access most probably due to the angulation between the brachiocephalic trunk and the aortic arch, with subsequent successful radial access conversion. E, Anterior view of a bilateral CSDH in which a frontline radial access was chosen. Following right CSDH embolization by the transradial approach, failure to navigate the left carotid artery led to radial-to-femoral access conversion and left-sided successful embolization. F, Anterior view in a case of failed catheterization of the left carotid artery from a frontline femoral access after which the procedure was aborted.
The CSDH embolization procedure was aborted in 15/143 (10%) cases, in 6 instances because of agitation, in 6 cases because of failed catheterization, and in 3 cases because of a so-called “dangerous anastomosis,” including 2 cases in which the MMA originated from the ophthalmic artery. Notably, once the guiding catheter was successfully placed, microcatheter navigation in the external carotid artery and MMA was always achieved. A total of 128/143 (90%) MMAs were embolized. Embolization was performed with calibrated tris-acryl microspheres (300–500 µm in diameter) in 111/128 (87%) instances, with associated proximal MMA coiling in 33/111 (30%) cases; using an n-BCA liquid embolic agent in 6/128 (5%) cases; by proximal MMA coiling alone in 10/128 (8%) cases; and by a gelatin-based embolic agent in the remaining patient (1%). We registered 7 minor complications in 124 patients (6%): 1 partial seizure during the procedure, 1 reversible headache, 2 transient diplopias, 2 asymptomatic iatrogenic meningomeningeal fistulas treated by MMA coiling during the procedure, and 1 asymptomatic external carotid artery occlusion. The only major complication (1%) was a femoral artery occlusion at the access site, treated surgically. The patient died 6 weeks after the CSDH embolization procedure.
Outcome
During period one, 5/48 (10%) CSDH embolization procedures were aborted due to failed catheterization. In all cases of failed catheterization, only a femoral access was attempted (Fig 2, illustrative cases A and B). In comparison, during period 2, only 1/95 (1%) procedures was interrupted after a failed attempt to catheterize a left carotid artery by a femoral access (Fig 2, illustrative case F), significantly less than during period 1 (P = .009). During periods 1 and 2, all 5 femoral-to-radial and radial-to-femoral conversions led to successful CSDH embolizations (Fig 2, illustrative cases C, D, and E). In none of the 6 failed catheterizations was an access site conversion attempted. The mean age of patients with failed catheterization was 81 [SD, 9] years and tended to be higher than that in the general study population, but the difference did not reach statistical significance (P = .21).
The rates of femoral-to-radial (P = .55) and total conversion (P = .86) did not differ significantly between the 2 periods. No significant difference was found regarding the duration of fluoroscopy between the 2 periods (P = .62) (Table 2).
Comparison of outcomesa
DISCUSSION
Main Results
This nonrandomized study shows that a CTA-based patient-tailored choice of frontline arterial femoral or radial access reduces the rate of catheterization failure in CSDH embolization procedures. Moreover, femoral-to-radial and radial-to-femoral per-procedure conversion should be considered when faced with challenging endovascular navigation because versatility appears to improve procedure outcomes.
MMA Embolization in the Treatment of CSDH
MMA embolization has been proposed as a potential treatment for CSDH.7,8 Enhanced understanding of CSDH physiopathology underlies the rationale for CSDH embolization.13 Morphologically, microvasculature alterations of the outer membrane of the CSDH include increased vessel density, capillary diameter, and the occurrence of large intercellular gaps between the endothelial cells.14,15 MMA embolization aims to occlude the so-called sinusoid neovessels of the CSDH outer membrane and subsequently reduce repeated microhemorrhage. Both curative embolization as a sole treatment7,16⇓-18 or combined management with embolization as an adjunct to surgical treatment have been proposed.7,19,20 A variety of embolic agents have been described in this context, mostly calibrated particles but also coils, n-BCA, or ethylene-vinyl alcohol copolymer liquid embolic agents.7,17,21⇓-23 Ban et al,7 in a relatively large study, compared 72 consecutive patients treated by CSDH embolization, either curative (27 patients) or as an adjunct to surgery (45 patients), with a historical control group of 469 patients managed conventionally either by an operation alone or conservatively. The treatment failure rate in the embolization group was found to be significantly reduced (1%) compared with historical controls (27.5%).
Challenging Catheterization and Radial Access
As stated above, CSDH is mostly a disease of the elderly.1 Indeed, the mean age of the study population described herein is >5 years higher than in patients included in real-life mechanical thrombectomy registries.24,25 Advanced age is associated with peripheral vascular disease, aortic arch elongation, and increased carotid artery tortuosity, all of which can increase technical difficulty or even preclude endovascular navigation by femoral access.9,10,26,27 The 2 largest CSDH embolization series to date have reported populations with an average age younger than 70 years,7,8 closer to the ages of patients undergoing mechanical thrombectomy than those reported herein. This may explain why technical difficulties related to CSDH embolization have not been highlighted before.
Radial access was described >3 decades ago.28 It has since become the access route of choice in percutaneous cardiac interventions, mainly due to demonstrated superiority in terms of patient satisfaction, cost effectiveness, and, more important, reduced local complication rates and even cardiac mortality.29,30 Transfemoral access exposes patients to a risk of retroperitoneal hematoma with potentially catastrophic consequences, especially in the setting of antiplatelet or anti-coagulant medication. Alternatively, hand ischemia is a potentially devastating complication of radial access, but in practice, radial artery occlusion remains essentially clinically silent.31 In the Minimizing Adverse Haemorrhagic Events by Transradial Access Site and Systemic Implementation of AngioX (MATRIX) trial, >4000 patients were randomized to transradial access and none presented with symptomatic hand ischemia.31,32
Interventional neuroradiology has lagged behind in adopting radial access, and several factors have been proposed to explain this hesitancy: Interventional neuroradiology training is dominated by femoral access, and there is a perceived difficulty in navigating the cerebrovasculature from the radial artery.11 Despite these potential impediments, several centers have successfully implemented radial-access strategies for diagnostic cerebral angiographies and neurointerventional therapeutic procedures.11,33⇓–35 Although definite evidence of the potential benefit of radial access in neurointerventional procedures is still lacking, several studies have pointed out reduced patient discomfort, reduced complication rates, and even enhanced technical feasibility in a subset of patients.10,11,33,34 The critical importance of both safety and technical feasibility in the specific context of CSDH embolization is underlined by the results of this study.
Both radial and femoral access strategies have specific complications and drawbacks, further highlighting the potential benefit of a tailored-access strategy. For instance, considering alternative access sites to transfemoral access has been recommended in patients with known prior surgery, stent placement, or occlusion of the femoral or iliac arteries or descending aorta.31 Alternatively, tortuosity and acute angulation of the left common carotid artery and internal carotid artery have been associated with radial approach failure.36
Study Limitations
The retrospective, monocentric, and nonrandomized design of this study are all potential sources of bias. In particular, it cannot be excluded that later-stage reduced rates of failure to catheterize are related to more aggressive endovascular navigation. Indeed, CSDH embolization is an emerging procedure for which the perceived utility may have increased across time during the study, therefore reducing the acceptability of procedural failure. However, the stability of fluoroscopy durations between the study periods contradicts this notion. Fluoroscopy duration as an outcome is, in itself, also subject to bias given that it does not distinguish the duration of endovascular navigation as opposed to embolization time. Also, criteria leading to the choice of a frontline radial or femoral access were largely based on operator preferences and eluded this study. Moreover, it could be that increased recourse to the radial route in itself, rather than the patient-tailored strategy of frontline access, reduced catheterization failure. Indeed, an increased choice of radial access as a frontline option and the propensity to switch from femoral to radial access in case of challenging anatomies may be thought of as mutually reinforcing. As stated earlier, in none of the 6 failed catheterizations was an access site conversion attempted, stressing the fact that improved catheterization rates may be a marker of increased versatility. This may be especially true in the general context of the modification of access strategies in interventional neuroradiology underway.
Also, the learning curve effect cannot be excluded to explain reduced later-stage catheterization failure. Experience gained during period 1 could have led to better operator performance during period 2. This is unlikely, however, for femoral access, given that challenging anatomies have become common with the advent of mechanical thrombectomy, and catheterization failure is now exceptional in this context, albeit with dedicated catheters with enhanced navigability. Also, given the potentially debilitating consequences of stroke, physicians may be less reluctant to perform more aggressive endovascular maneuvers to reach the target vessel in this setting. Finally, as illustrated in this study population, agitation is also a frequent cause of procedural abortion with the patient under local anesthesia or even conscious sedation. General anesthesia should be considered in a subset of patients to increase procedural success rates.
CONCLUSIONS
A CTA-based patient-tailored choice of frontline arterial access reduces the rate of catheterization failure in CSDH embolization procedures.
Footnotes
Disclosures: Eimad Shotar—UNRELATED: Grants/Grants Pending: Principal Investigator of the EMPROTECT randomized trial.* Nader Sourour—UNRELATED: Consultancy: Medtronic, Balt. Frédéric Clarençon—UNRELATED: Board Membership: ArteDrone; Payment for Development of Educational Presentations: Balt, Penumbra, Guerbet. *Money paid to the institution.
References
- Received July 5, 2020.
- Accepted after revision October 12, 2020.
- © 2021 by American Journal of Neuroradiology





{kind=link}
{kind=link}