
Abstract
SUMMARY: Optic nerve choristomas are rare entities in which a developmental focus of histologically normal tissue is abnormally located within or along a segment of the optic nerve. Although benign, choristomas may demonstrate slow growth, ultimately resulting in visual field deficits due to compression of the adjacent nerve in the few cases reported in the anterior fossa. Choristomas may have cystic components, though this has not been described in such lesions along the optic nerve. Here, a predominantly cystic optic nerve choristoma is described, with radiologic features mimicking those of an anterior cranial fossa neurenteric cyst. The case highlights the radiology-pathology correlates of choristomas and reviews the surgical approach and management of patients with such lesions.
The patient was a 64-year-old woman who presented from an outside institution with an intracranial cyst. The lesion had been discovered during a hospitalization for unrelated pulmonary emboli, when the patient underwent a head CT after revealing a multiyear history of headaches during her review of systems. On examination, the patient had trace temporal field vision loss in her left eye. A battery of pituitary function tests was completed, given the proximity of the cyst to the pituitary gland, all of which had normal findings. The patient was referred for assessment by neurosurgery, with additional imaging performed.
Imaging
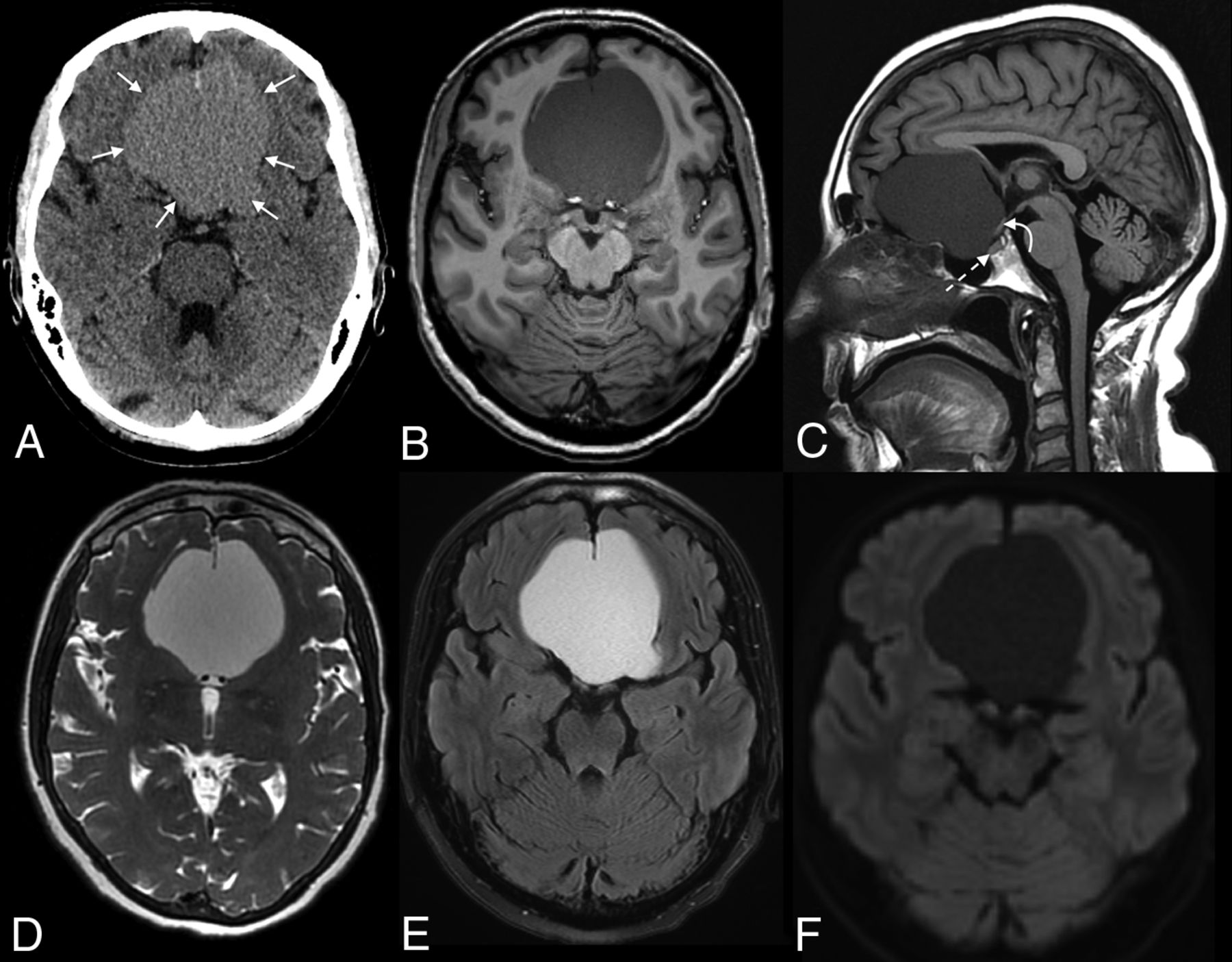
CT and subsequent MR imaging demonstrated a large extra-axial cystic mass in the anterior cranial fossa (Fig 1). Most of the lesion was centered over the planum sphenoidale, with remodeling of the adjacent bone. Posteriorly, the cyst extended into the sella, slightly compressing the anterior pituitary gland and causing substantial deviation of the optic chiasm. The anterior margins of the cyst were draped around the falx cerebri, while the bifrontal cerebral gyri, corpus callosum, and distal ICAs were all displaced by the cyst. The intracystic fluid was hyperintense on both T2 and FLAIR sequences and did not restrict diffusion. A punctate T1-hyperintense focus was noted along the left optic nerve.

Preoperative CT and MR images of the lesion. Axial CT (A), axial (B) and sagittal (C) MPRAGE, and axial T2 Cube (GE Healthcare) (D), T2-FLAIR (E), and DWI (F) demonstrate an extra-axial cystic lesion in the anterior cranial fossa (between arrows, A). The cyst drapes around the anterior falx and causes substantial mass effect on the adjacent bifrontal gyri. The optic chiasm (curved arrow, C) and pituitary gland (dashed arrow, C) are deviated posteriorly. The intracystic fluid signal is slightly hyperintense to CSF on T2 Cube, does not suppress on FLAIR, and does not restrict on DWI.
The appearance of the lesion was thought to have attributes of a slow-growing, benign intracranial cyst. The intralesional fluid content was uncharacteristic of the most commonly encountered cysts: the fluid did not mimic CSF like an arachnoid cyst, did not restrict diffusion as would be expected with an epidermoid cyst, and did not have intralesional fat suggestive of a dermoid cyst. The most likely entity was thought to be a neurenteric cyst; though rarely intracranial, neurenteric cysts in the anterior cranial fossa share many of the imaging characteristics seen in this case.1,2 A Rathke cleft cyst and craniopharyngioma were considered much less likely because the cyst did not appear to originate from the sella.
The patient ultimately underwent surgical treatment of the cyst 6 months after presentation.
Operative Report and Subsequent Image Review
The operation was completed via a small left frontal craniotomy with a subfrontal approach. An endonasal approach was not selected because the preoperative consensus was that this was a neurenteric cyst, and the surgeon did not believe the whole capsule could be removed from the middle fossa component. The cyst was immediately identified and contained a yellowish fluid when opened. Starting on the left side, the cyst lining was carefully dissected from the olfactory nerve and the frontal lobe. However, an unexpected small granular lesion was observed along the medial surface of the left optic nerve (Fig 2). This was partially resected and sent to pathology. Examination of the surgical field found no other such lesions. The surgeons then proceeded to remove all additional remaining cyst linings before the conclusion of the procedure.

Intraoperative view of a left frontal craniotomy with a subfrontal approach for resection of an anterior cranial fossa cyst. A granular lesion adhering to the medial surface of the left optic nerve is shown, with adjacent structures labeled. L. indicates left.
Postoperatively, images were re-reviewed to assess a correlate with the intraoperative findings. A punctate focus of T1-hyperintensity along the medial margin of the left optic nerve was observed, which demonstrated questionable, superimposed, associated enhancement corresponding to the small granular lesion identified intraoperatively (Fig 3).

Re-review of preoperative coronal MPRAGE (A) and postcontrast (B) images demonstrates a T1-hyperintense focus along the left optic nerve (arrows), correlating with the surgical findings. Intrinsic T1 signal was presumably related to the intralesional fat tissue noted on subsequent histologic analysis. Although faint enhancement was seen in the adjacent tissue, it was not certain whether a component of this solid focus demonstrated definite enhancement (B).
Diagnosis
The diagnosis was benign epithelial cyst associated with an optic nerve choristoma.
Pathology
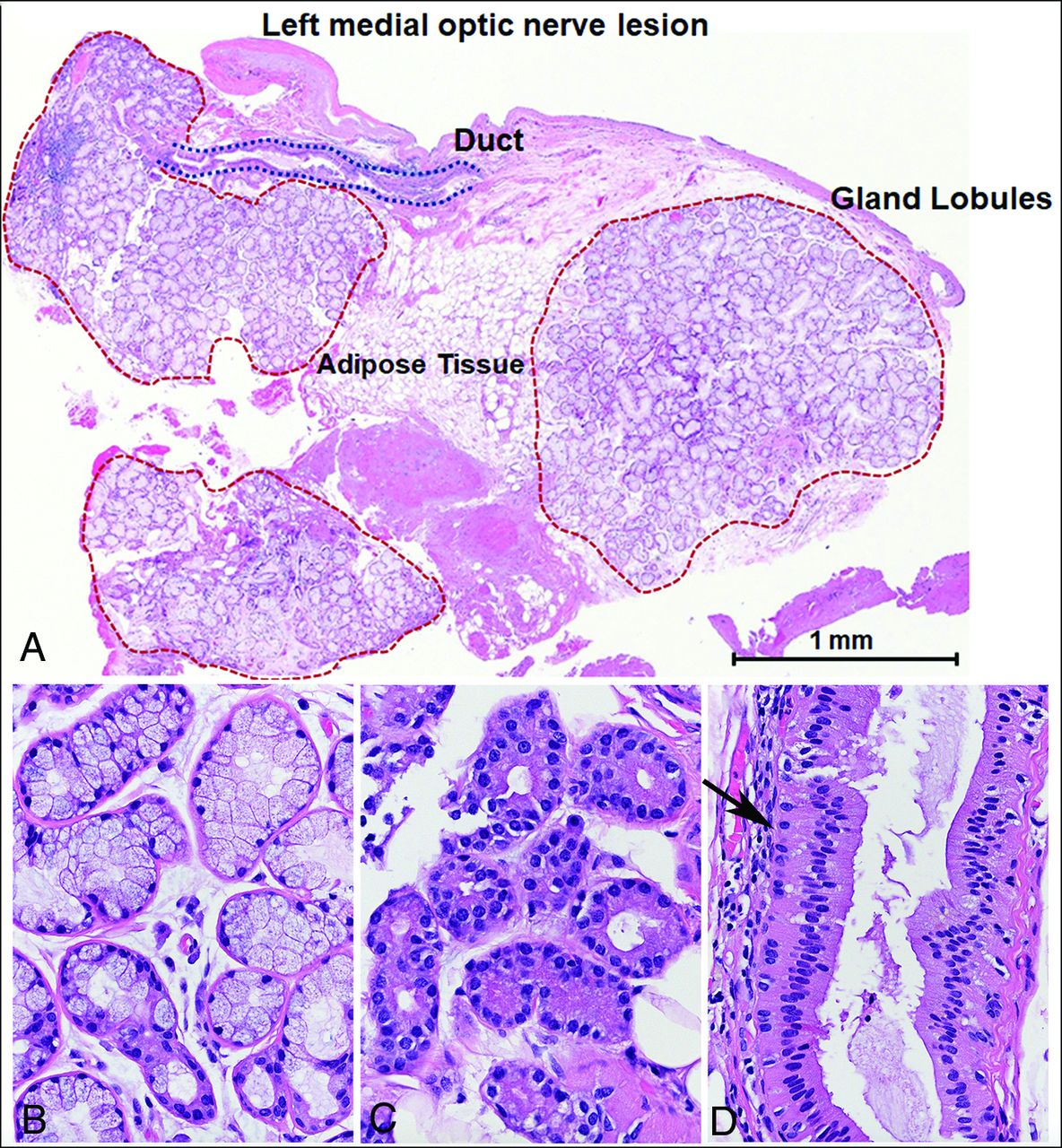
The specimen resected along the left medial optic nerve showed small glandular lobules composed predominantly of mucin-producing cells and, to a lesser extent, of serous cells associated with small ductal structures, consistent with salivary gland tissue (Fig 4). This was intermixed with adipose tissue, compatible with an optic nerve salivary gland choristoma. The cyst specimens showed a folded benign epithelial cyst wall with a double layer of cells, including a basal layer, p63-positive, as well as a superficial flattened layer, diffusely positive for anti-cytokeratin (CAM5.2) (Fig 5). There was no evidence of mucin-producing cells and no evidence of cilia, confirmed by the negative BRAF V600E stains.3 The cyst lining resembled, to some extent, a cystically dilated duct. It was not the lining of an enterogenous (neuroenteric) cyst, which is typically composed of a single layer of columnar cells, often ciliated and mucin-producing cells with goblet cells. The cyst lining epithelium lay over a fibrous stroma containing reactive arachnoid cells, highlighted by the progesterone receptor stain, as well as rare microcalcifications. The histopathologic findings were not those of a cystic craniopharyngioma. BRAF V600E and beta-catenin immunostaining, markers characteristic of papillary and adamantinomatous variants of craniopharyngioma, were performed and were negative.

Optic nerve choristoma composed of adipose tissue, glandular lobules, and ducts (A), with predominant mucinous (B) and scant serous (C) glands consistent with salivary gland tissue. The duct (D) shows a typical basal cell layer (black arrow) and columnar lining.

The collapsed cyst wall shows largely a flattened lining (A and B) bistratified positive for CAM5.2 (C). p63-positivity is limited to the basal cells of the bistratified epithelium lining the cyst wall as typically seen in duct structures (D). BRAF V600E, a marker of papillary craniopharyngioma, is negative (E); the stain is also typically positive in normal cilia, which were not present in the cyst lining. The cyst lining shows normal cytoplasmic beta-catenin expression (F) and also of epithelial membrane antigen (EMA) (G), while progesterone receptor (PR) stain is present in a subset of the arachnoidal cells observed in the fibrous stroma associated with the cyst wall (J).
DISCUSSION
Choristomas are composed of normal, mature tissue that is located in an abnormal anatomic location. They have been described throughout the body, from the head and neck to the extremities.4,5 Choristomas do not have a sex predilection and can present at any age.6 Optic nerve choristomas, though exceedingly rare, have been previously reported.7⇓⇓-10 More frequently, optic nerve choristomas contain smooth-muscle and adipose tissue and, only rarely, salivary gland tissue.11 The lesions often demonstrate slow progressive growth, sometimes eventually causing compressive atrophy of the optic nerve.11 Nevertheless, choristomas are uniformly benign and considered to be developmental rather than neoplastic.
Radiologic descriptions of optic nerve choristomas remain predictably scarce. Adipose-rich choristomas exhibit intralesional fat density on CT and demonstrate fat signal on MR imaging with drop-out of signal on fat-suppression sequences.12 Lesions composed of predominantly smooth-muscle or glandular tissue, conversely, often lack such characteristic imaging findings. Both intralesional enhancement and enhancement of the adjacent optic nerve have been reported.11,13 The adjacent optic nerve may be enlarged due to mass effect related to the tumor or small due to compressive atrophy.6 An enhancing tumor involving the optic nerve (or sheath) should raise suspicion for either an optic nerve glioma or meningioma, though a dominant cyst arising from an optic nerve glioma in an adult would be atypical.14 In addition, a teratoma could be considered; such lesions are composed of all 3 germ cell layers and can appear as cystic lesions with components of intralesional fat. However, a newly diagnosed teratoma would be rare in an adult because the incidence decreases with age.15 Most teratomas also have some degree of calcification, which was lacking in this case.16
Intracranial cysts, conversely, are not uncommon. As mentioned above, the lesion in the current case shared many features of a supratentorial neurenteric cyst: Intracystic fluid was hyperintense to CSF on FLAIR sequences (unlike arachnoid cysts, which mimic CSF) and lacked intralesional restricted diffusion (unlike epidermoid cysts).2,17 Thus, this case is an example of the need to closely examine the margins of all cystic foci for fat signal or pathologic enhancement.
To the best of our knowledge, this is the first reported instance of an optic nerve choristoma leading to the formation of a such a large epithelial cyst, most likely representing a very large dilated duct. Nevertheless, cystic choristomas are known entities.18-20 Glandular tissue is found within such lesions, as was noted on histologic analysis of the current case.18 It is possible that these cysts develop from persistent excretion of fluid from intralesional glandular tissue. In the patient presented here, slow excretion of fluid would conceivably account for its insidious clinical onset and bony remodeling.
Surgical resection of choristomas is typically curative, though reports of recurrence following incomplete resection have been reported.21 In this case, surgical resection of the cyst wall would likely have little effect on future recurrence of the cyst because no secretory histologic components were noted in the actual cyst wall. The patient reported here is expected to make a full recovery, with resolution of her symptoms and no new neurologic deficits expected. Follow-up MRIs will be completed in 6 and 12 months to exclude recurrence of the solid tumor or re-accumulation of cystic fluid.
Case Summary
Choristomas are benign lesions, in which histologically normal tissue is located in an abnormal anatomic location
Imaging features of choristomas vary on the basis of the histologic composition of each lesion. Adipose-rich lesions demonstrate expected features of fat tissue on CT and MR imaging; characteristics of other lesions are less specific
Because many pathologic lesions may have cystic components, identification of any intracranial cyst should prompt close scrutiny of the margins of the lesion for T1-hyperintense or enhancing foci
The differential diagnosis of a large cystic lesion in the anterior cranial fossa is ample and includes neurenteric cysts, arachnoid cysts, Rathke cleft cysts, teratomas, cystic pituitary adenomas, craniopharyngiomas, and epidermoid and dermoid cysts. Cystic choristoma is a very rare possibility.
Footnotes
Disclosures: John Port—UNRELATED: Consultancy: BioClinica, Comments: I am an imaging consultant to Bioclinica; consulting fees are paid to Mayo Clinic.* *Money paid to the institution.
References
- Received July 29, 2020.
- Accepted after revision August 27, 2020.
- © 2021 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.