
Abstract
BACKGROUND: Outcomes after endovascular embolization of vein of Galen malformations remain relatively poorly described.
PURPOSE: We performed a systematic review of the literature to determine outcomes and predictors of good outcomes following endovascular treatment of vein of Galen malformations.
DATA SOURCES: We used Ovid MEDLINE, Ovid Embase, and the Web of Science.
STUDY SELECTION: Our study consisted of all case series with ≥4 patients receiving endovascular treatment of vein of Galen malformations published through January 2017.
DATA ANALYSIS: We studied the following outcomes: complete/near-complete occlusion rates, technical complications, perioperative stroke, perioperative hemorrhage, technical mortality, all-cause mortality, poor neurologic outcomes, and good neurologic outcomes. Outcomes were stratified by age-group (neonate, infant, child). A random-effects meta-analysis was performed.
DATA SYNTHESIS: A total of 27 series with 578 patients were included; 41.9% of patients were neonates, 45.0% of patients were infants, and 13.1% of patients were children. All-cause mortality was 14.0% (95% CI, 8.0%–22.0%). Overall good neurologic outcome rates were 62.0% (95% CI, 57.0%–67.0%). Overall poor neurologic outcome rates were 21.0% (95% CI, 17.0%–26.0%). Neonates were significantly less likely to have good neurologic outcomes than infants (48.0%; 95% CI, 35.0%–62.0% versus 77.0%; 95% CI, 70.0%–84.0%; P < .01). Treatment indications following the Bicêtre neonatal evaluation score resulted in significantly higher rates of good neurologic outcome (P = .04). Patients with congestive heart failure had significantly lower rates of good neurologic outcome (OR, 0.50; 95% CI, 0.28–0.88; P = .01).
LIMITATIONS: Limitations were selection and publication biases.
CONCLUSIONS: Patients receiving endovascular embolization of vein of Galen malformations experienced good long-term clinical outcomes in >60% of cases. Appropriate patient selection is key as treatment guided by the Bicêtre neonatal evaluation score was associated with improved neurologic outcomes.
ABBREVIATIONS:
- BNES
- Bicêtre neonatal evaluation score
- CHF
- congestive heart failure
- PRISMA
- Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- VOGM
- vein of Galen arteriovenous malformation
Vein of Galen arteriovenous malformations (VOGMs) are shunts that form in utero between the choroidal arteries and the precursor of the vein of Galen, the median prosencephalic vein of Markowski.1⇓–3 Current prevalence estimates of VOGM are quite low, often cited at <1 of 25,000 deliveries.4,5 A number of studies have shown that the natural history of VOGMs is very poor, with many patients succumbing to complications related to congestive heart failure (CHF), hydrocephalus, and brain parenchymal injury.
Endovascular embolization of VOGMs has emerged as a standard of care in this patient population; however, long-term outcomes after endovascular embolization, as well as predictors of good neurologic outcomes, are still poorly understood.2⇓–4,6⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓–47 Thus, to assess the status of endovascular treatment for VOGMs, we performed a systematic review and meta-analysis with an emphasis on determining factors associated with good neurologic outcome in this patient population.
Materials and Methods
Literature Search
Our study adheres to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA; http://prisma-statement.org/) guidelines. To identify studies on outcomes of endovascular treatment of VOGMs, we performed a computerized MEDLINE search of the literature from January 1980 to January 2017. Three data bases were searched from January 1980 to April 2017: Ovid MEDLINE, Ovid Embase, and the Web of Science as described in On-line Table 1. Initial search terms included “Vein of Galen,” “malformation,” “aneurysm,” “endovascular,” “coil,” “embolization,” and “occlusion.” Identified studies from the search were then further evaluated for inclusion in the systematic review. Inclusion criteria were the following: 1) studies reporting a consecutive series of endovascular treatment of VOGMs (≥4 patients), including case series and clinical trials; and 2) studies reporting angiographic and/or clinical outcomes following treatment. Case reports were excluded from this study. Two independent reviewers selected studies for this analysis.
Data Extraction and Outcomes
Each study was analyzed by 2 independent reviewers to collect the following data: 1) patient presentation (congestive heart failure, hydrocephalus, seizure); 2) patient demographics (age, sex); 3) treatment type (transarterial versus transvenous); 4) number of treatments/stages; 5) perioperative complications (technical mortality, perioperative ischemia, and perioperative hemorrhage); 6) complete/near-complete embolization rate; 7) long-term clinical outcomes, including good clinical outcome (defined as no or minor developmental delay and no permanent disability), poor clinical outcome, and all-cause mortality; and 8) angioarchitecture of the lesion (mural versus choroidal). The primary outcome of this study was good neurologic outcome rates. Good neurologic outcome was defined as a child with normal development.
In addition to determining overall rates of the outcomes listed above, we performed subgroup analyses dividing patients by age group. The 3 age groups studied were neonates (younger than 1 month of age), infants (1 month to 2 years of age), and children (2 years of age and older). We also performed subgroup analyses to determine whether the following variables were associated with rates of good neurologic outcome: 1) use of the Bicêtre neonatal evaluation score (BNES) for patient selection, 2) the presence of CHF, 3) a prenatal diagnosis of VOGM, 4) hydrocephalus, and 5) type of VOGM (mural versus choroidal). A subgroup analysis by follow-up time (≤2 years versus >2 years) was also performed.
Risk of Bias Assessment
Risk of bias assessment of the studies was performed with a modified Newcastle-Ottawa Scale. This tool is used for assessing the quality of nonrandomized studies included in systematic reviews and/or meta-analyses. Each study is judged on 8 items categorized into 3 groups: 1) selection of the study groups, 2) comparability of the study groups, and 3) ascertainment of the outcome of interest.48 Factors that would make a study at low risk of bias would include the following: 1) well-defined selection criteria, 2) well-defined treatment regimen, 3) rates of long-term follow-up of >90% for surviving patients, and 4) age-based stratification of outcomes.
Statistical Analysis
We estimated, from each study, the cumulative incidence (event rate) and 95% confidence interval for each outcome. Event rates were pooled across studies with a random-effects meta-analysis.49 Heterogeneity across studies was evaluated with the I2 statistic.50 Analysis of outcomes for children older than 2 years of age could not be performed due to the lack of sufficient studies. Analysis was conducted with STATA Statistical Software, Release 14 (StataCorp, College Station, Texas).
Results
Literature Search, Study Characteristics, and Risk of Bias
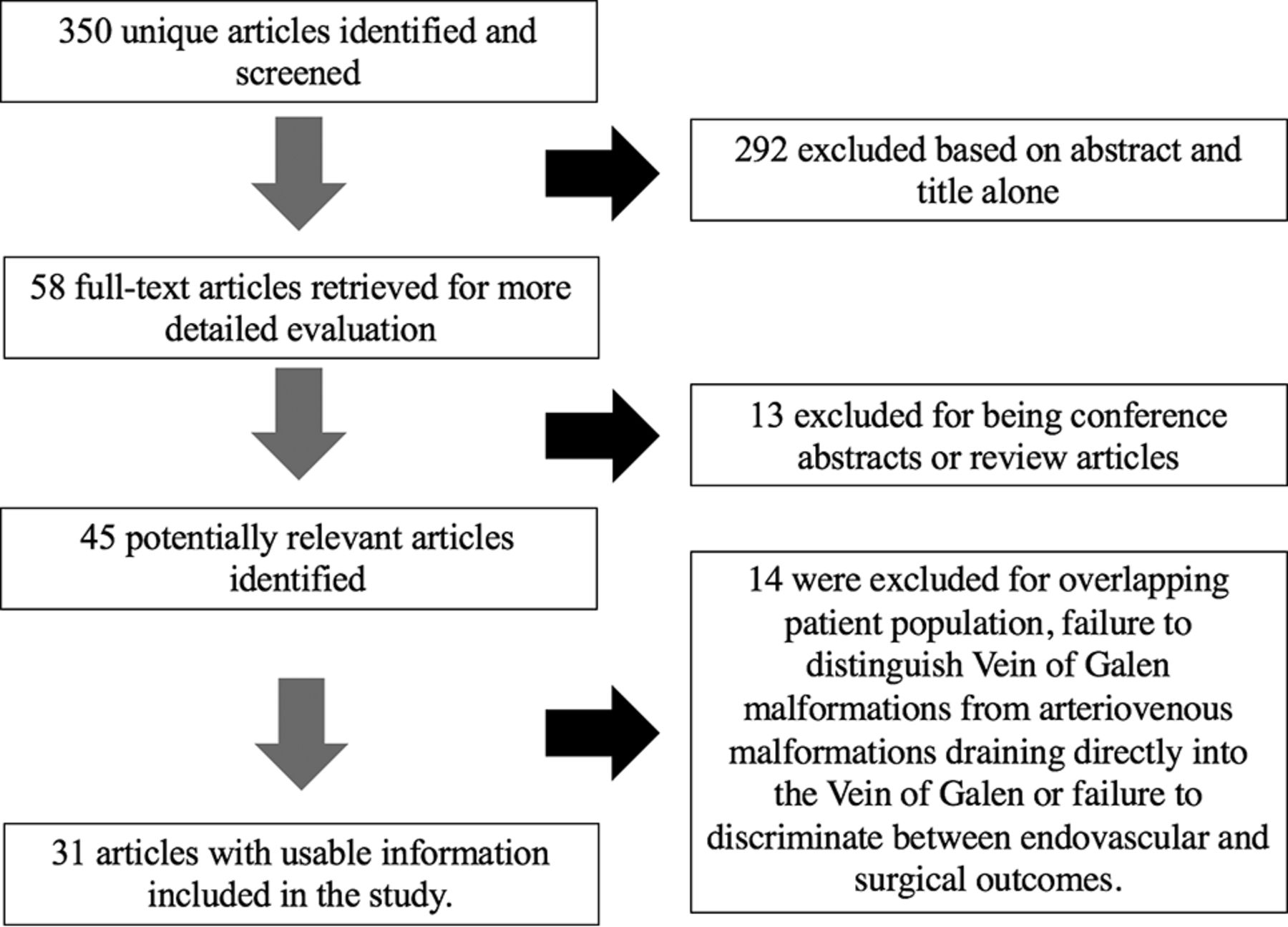
The initial literature searched yielded 350 unique articles. On review of the abstracts and titles, 292 articles were immediately excluded. Fifty-eight articles were retrieved for full-text evaluation. Of these, 13 were excluded because they were review articles or conference abstracts with insufficent information. Forty-five articles were then evaluated. Of these, 14 were excluded for overlapping patient populations, failure to distinguish vein of Galen malformations from arteriovenous malformations draining directly into the vein of Galen, or failure to discriminate between endovascular and surgical outcomes. In total, 31 articles reflective of the experiences of 27 centers were included. There were 4 articles that had overlapping patient populations, but these were included because they provided additional data not available in other articles from the institution. In total, 578 unique patients were included. These findings are summarized in Fig 1.

PRISMA flow diagram.
Six institution experiences were found to have a low risk of bias, 7 institution experiences had a moderate risk of bias, and 14 studies had a high risk of bias. Eight institution experiences used the BNES in determining patient eligibility for treatment. The number of patients ranged from 4 to 216. Mean follow-up ranged from 0.5 to 6.8 years with a median of 2 years. These data are summarized in On-line Table 2.
Baseline Characteristics and Patient Presentation
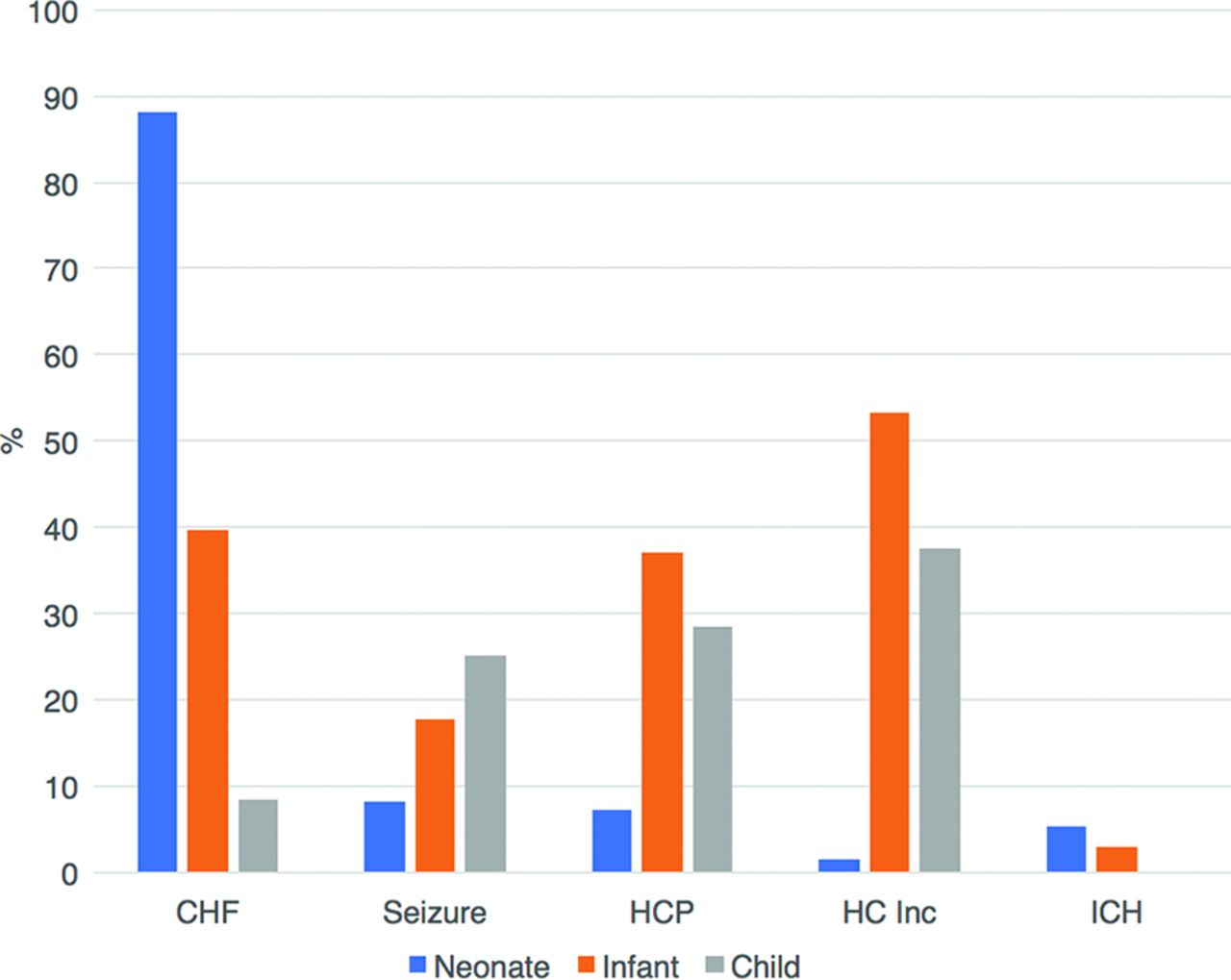
The median age of patients included in this study was 0.1 month. Age data were available for 547 patients; 229 patients were neonates (41.9%), 246 patients were infants (45.0%), and 72 patients were children (13.2%). Sex data were available for 252 patients, and 173 patients (68.7%) were male. Patient presentation data were available for 318 patients. The most common presentation was CHF (201 patients, 63.2%), followed by hydrocephalus (86 patients, 27.0%) and seizure (37 patients, 11.6%). Intracranial hemorrhage was present in 26 patients (8.2%). An age-related breakdown of patient presentation is provided in Fig 2. Briefly, the most common presentation in neonates was CHF (88.2%). The most common presentation in infants and children was increased head circumference (53.3% and 37.5%, respectively). Angioarchitectural characteristics were available for 276 patients, with 103 being mural (37.3%) and 173 being choroidal (62.7%).

Presentation by age group. HCP indicates hydrocephalus; HC, head circumference; ICH, intracranial hemorrhage; inc, increase.
Angiographic Outcomes
Twelve studies primarily used transarterial embolization for treatment of VOGMs. The median number of treatments ranged from 1.5 to 4.1, with the overall median of included studies being 2.25; 27.9% of patients received 1 treatment, 29.1% received 2 treatments, and 43.0% received ≥3 treatments. The overall complete occlusion rate was 56.0% (95% CI, 46.0%–66.0%), with no difference between neonates and infants.
Perioperative Complications
The overall technical complication rate was 19.0% (95% CI, 12.0%–27.0%), with a trend toward a significantly higher rate of technical complications among neonates (29.0%; 95% CI, 17.0%–41.0%) compared with infants (10.0%; 95% CI, 0.0%–27.0%; P = .07). Overall perioperative hemorrhage rates were 9.0% (95% CI, 4.0%–15.0%), with no difference between age groups (P = .25). Overall perioperative ischemia rates were 1.0% (95% CI, 0.0%–2.0%), with a higher rate among neonates (3.0%; 95% CI, 0.0%–10.0%) compared with infants (0.0%; 95% CI, 0.0%–2.0%; P = .03). Non-neurologic complicate rates were 2.0% (95% CI, 0.0%–4.0%), with no difference among groups (P = 1.0). The overall technical mortality rate was 1.0% (95% CI, 0.0%–5.0%), with higher rates in neonates (2.0%; 95% CI, 0.0%–8.0%) than in infants (0.0%; 95% CI, 0.0%–2.0%; P = .03). These data are summarized in the Table.
Systematic review outcomes
Long-Term Outcomes
The overall rate of good neurologic outcome was 62.0% (95% CI, 57.0%–67.0%). Neonates had significantly lower rates of good neurologic outcomes (48.0%; 95% CI, 35.0%–62.0%) compared with infants (77.0%; 95% CI, 70.0%–84.0%; P < .0001). Overall rates of poor neurologic outcome were 21.0% (95% CI, 17.0%–26.0%), with higher rates among neonates (22.0%; 95% CI, 15.0%–31.0%) compared with infants (16.0%; 95% CI, 10.0%–23.0%; P = .01). The all-cause mortality rate was 14.0% (95% CI, 8.0%–20.0%), with significantly higher rates among neonates (27.0%; 95% CI, 15.0%–41.0%) compared with infants (1.0%; 95% CI, 0.0%–4.0%; P < .0001). These data are summarized in the Table. The forest plot for good neurologic outcomes is provided in Fig 3.

Forest plot for good neurologic outcome.
Follow-Up Time, Patient Selection, and Baseline Characteristics and Outcomes
Seven studies reported the use of the BNES in selecting patients for treatment of VOGMs. Studies that reported the use of the BNES had significantly higher rates of good neurologic outcome than those that did not (62%; 95% CI, 50.0%–72.0% versus 57%; 95% CI, 51.0%–65.0%; P = .04).
Patients with CHF were significantly less likely to experience good neurologic outcomes than those without CHF (49.4%; 95% CI, 21.7%–57.1% versus 66.2%; 95% CI, 55.1%–75.8%; P = .01). Patients with hydrocephalus (61.0%; 95% CI, 45.7%–74.4%) had similar rates of good neurologic outcome as those without it (62.0%; 95% CI, 53.4%–70.0%; P = .92). Patients with mural-type VOGMs had a good neurologic outcome rate of 73.8% (95% CI, 59.0%–84.7%) compared with 58.0% (95% CI, 47.2%–68.2%) for choroidal VOGMs (P = .11). There was no association between a prenatal diagnosis and good neurologic outcome (66.7%; 95% CI, 53.7%–77.5% versus 63.1%; 95% CI, 50.9%–73.8%; P = .68).
There was a wide range in the follow-up times across studies, from 6 months to 6.8 years. The median follow-up time was 2 years, and the median age at which follow-up was performed was 2 years. Studies that reported a follow-up of >2 years had a good neurologic outcome rate of 60.3% (95% CI, 55.1%–65.3%), while studies reporting a follow-up of ≤2 years reported a good neurologic outcome rate of 64.6% (95% CI, 54.6%–73.4%) (P = .45).
Study Heterogeneity
When we considered all patients, I2 values were >50%, indicating substantial heterogeneity for perioperative hemorrhage. I2 values were <50% for all other outcomes, indicating lack of substantial heterogeneity. When we considered neonates, I2 values were >50%, indicating substantial heterogeneity for all-cause mortality. I2 values were <50% for all other outcomes, indicating a lack of substantial heterogeneity. When we considered infants, I2 values were >50%, indicating substantial heterogeneity for complete occlusion. I2 values were <50% for all other outcomes, indicating a lack of substantial heterogeneity. These data are summarized in the Table.
Discussion
Our study of >500 patients receiving endovascular treatment for VOGMs demonstrated many interesting findings. First, the most common presentation varied substantially by age of presentation as neonates were more likely to present with symptoms related to CHF, while infants were more likely to present with head circumference increases or hydrocephalus. Given the poor natural history of VOGMs and the poor functional status of many patients who require treatment for these lesions, rates of good long-term neurologic outcomes were satisfactory at >60%. Patients who underwent treatment during the neonatal period were less likely to have a good neurologic outcome than those who were treated later in life, likely due to poorer cardiologic status at presentation and increased severity of disease. Perioperative complications were not negligible and were more frequent in neonates than in infants. However, procedure-related mortality rates were low. We found that patients who were treated according to the Bicêtre guidelines were more likely to experience good outcomes than those who were not; this finding highlights the importance of patient selection. Overall, our results suggest that endovascular treatment of VOGMs is generally safe and effective and can result in good long-term outcomes for patients in experienced centers. However, an emphasis on patient selection and timing is key.
As demonstrated in our study, the principal clinical manifestations of VOGMs are related to high-output cardiac failure or neurologic symptoms secondary to venous congestion and abnormal CSF flow.4,23,35,36 CHF is the most common clinical presentation for neonates and is rarely the presenting symptom in infants or children because these patients often have fewer severe cardiac symptoms. In our study, approximately 90% of patients treated in the neonatal stage had CHF compared with 40% of patients treated in the infant stage. Many of the treated infants with CHF had medical stabilization of CHF during neonatal life with delay of treatment later in the first or second year of life. CHF can manifest itself on prenatal sonography or soon after birth, with symptoms ranging from mild overload to multisystem organ failure secondary to cardiogenic shock. On the contrary, patients with mild cardiac dysfunction may not have their VOGMs recognized until later in life when cerebral venous hypertension results in intracranial hypertension and subsequent macrocrania and hydrocephalus. As demonstrated in our study, >50% of infants presented with macrocrania and nearly 40% presented with hydrocephalus. Other neurologic presentations, including seizure and intracranial hemorrhage, are present in roughly 20% and 10% of patients, respectively, with increased prevalence as age increases.
One of the important findings from our study was that studies that used a predefined selection criteria, the BNES, demonstrated higher rates of good neurologic outcome than those that did not.23 These findings highlight the importance of appropriate patient selection to ensure good neurologic outcomes. The BNES is a 21-point score that assesses a combination of cardiac, neurologic, respiratory, hepatic, and renal functions.51 Patients with a score of ≤8 are thought to be poor candidates for endovascular treatment, and typically the recommendation is to withhold therapy from these patients. In the series of Lasjaunias et al, 30% of all neonates and 17% of all infants had treatment withheld due to such low scores. A score between 8 and 12 indicates normal neurologic function but cardiac function that is refractory to medical management and, thus, emergency embolization, regardless of patient age. In the Lasjaunias series, only 25% of neonates met these criteria and underwent emergent embolization.51 However, in these patients, all-cause mortality was high and rates of good neurologic outcome were relatively low. Patients with a neonatal score of 13–21 could have embolization delayed until 3–5 months of age with stabilization of their cardiac function. This population comprised about two-thirds of patients in the series of Lasjaunias et al.51 Our study found that close to 50% of treated patients were treated in the neonatal stage, while only 5% of treated patients in the series of Lasjaunias et al23 were neonates.
The high proportion of neonates treated in our study implies that there may be a reflexive instinct to treat neonates presenting with VOGM at some centers without allowing a trial of medical stabilization. Such practice patterns may be detrimental to patients because treatment of neonates is associated with higher rates of technical complications and lower rates of good neurologic outcomes; and in select cases in which the neonate can be stabilized, delaying treatment for a few months may confer a benefit on the patient.23 Ultimately, due to the complex medical needs of this patient population, an argument can be made for centralization of medical and endovascular treatment for these patients.
Due to substantial heterogeneity and lack of specifics in reporting technical details of embolization procedures, we were unable to perform an extensive evaluation of the safety and efficacy of various techniques in the treatment of VOGMs.23 However, there are a few important implications from our study. First, as mentioned above, technical complications are more common in neonates than infants, likely due to a combination of smaller size, vascular fragility, and a more tenuous hemodynamic state. While most of the included studies predominantly treated patients transarterially, several series reported the exclusive use of transvenous or transtorcular techniques.27,37,45 Earlier series were more likely to report exclusive transvenous treatment or transtorcular embolization than more modern series however. In general, isolated transvenous treatment is thought to result in higher rates of technical complications due to higher rates of postoperative venous infarction, hemorrhage, and consumptive coagulopathy.19,23 Transtorcular embolization has become less and less common during the past decade due to extraordinarily high rates of such complications. Ultimately, treatment should be tailored to the angioarchitecture of the lesion and available routes for embolization.9 When we considered all patients, complete occlusion rates were approximately 60%. Complete occlusion should not necessarily be the goal of VOGM embolization; rather, improvement in the physiologic and neurologic status of the patient should be the primary treatment goal.
Limitations
Our study has limitations. Ecologic bias (ie, comparisons are made across studies and not within studies), the presence of publication bias, and statistical heterogeneity are limitations that affect all meta-analyses. Our study also had limitations due to the methodologic limitations of included studies. All included studies were retrospective case series, which are prone to substantial selection bias. The use of the BNES in selecting patients also introduced selection bias because patients in whom treatment was thought to be futile were excluded in those studies. Little is known regarding the outcomes of patients who were untreated. It is also conceivable that with advancements in techniques and experience, many of the patients who were excluded on the basis of the BNES could now be treated. Many of the included studies had a small sample size and incomplete follow-up data. In some cases, definitions of outcomes (ie, good neurologic outcome, complete occlusion, technical versus all-cause mortality, and so forth) were not well-defined. In addition, many of the series in our analysis included cases collected during several years. It is possible that complication rates have improved because of increased operator experience and skill, improved patient selection, and improved devices and technology. We do not have enough data to determine clinical and angiographic outcomes by type of embolic agent used. Last, it is difficult to sort out short- and long-term morbidity and mortality related to the pathology of the underlying VOGM itself and of endovascular treatment.
Conclusions
Endovascular embolization of VOGMs can be successfully performed; however, complications are not negligible. Patient selection and timing of treatment are key to achieving good clinical outcomes. Further work is needed to provide improved outcomes associated with endovascular treatment of VOGMs. Large multi-institutional registries may be helpful for collecting data in a standardized manner on the presentation and outcomes of these patients. Ultimately, these treatments are extremely challenging and should probably be reserved for centers with expertise in pediatric critical care and neurointervention.
References
- Received June 14, 2017.
- Accepted after revision August 7, 2017.
- © 2017 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Vein of Galen aneurysmal malformation treatment with direct open surgical access of the transverse sinus and transvenous selective endovascular embolization: a hybrid approach
- Cerebrovascular Anomalies in the Fetus
- Use of a mini balloon microcatheter to facilitate penetration of fine vascular networks and curative embolization in vein of Galen malformations
- Genetic dysregulation of an endothelial Ras signaling network in vein of Galen malformations
- Fine, Vascular Network Formation in Patients with Vein of Galen Aneurysmal Malformation
- Vein of Galen Malformation
- Fetal and Neonatal MRI Predictors of Aggressive Early Clinical Course in Vein of Galen Malformation
- Outcome of vein of Galen malformation presenting in the neonatal period
- Occlusion of a mural type vein of Galen malformation in a 10-month-old boy with three Woven EndoBridge (WEB 17) and two coils
- Anatomy of the deep venous system in vein of Galen malformation and its changes after endovascular treatment depicted by magnetic resonance venography
- Non-enhanced MR imaging for preinterventional assessment of the angioarchitecture in vein of Galen malformations