
Article Figures & Data
Figures
- Fig 1.
Mechanisms of air- and bone-conducted sound in healthy and third window anatomy. A, Normal air conduction. Vibrations of the tympanic membrane are transmitted inward through the auditory ossicles and oval window. Energy is then conducted through the incompressible perilymph, producing equal and outward motion of the round window. The difference in vibration between the oval and round windows generates a pressure gradient across the basilar membrane, activating hair cells and creating the perception of sound. B, Decreased air conduction in third window anatomy. Due to shunting across third windows (semicircular canal dehiscence [SCCD], EVAS, cochlear dehiscence), there is decreased energy transmission from the oval window to the round window. The decrease in pressure gradient across the basilar membrane yields reduced sound perception. C, Normal bone conduction. Vibrations are transmitted throughout the otic capsule. This transmission results in differential outward motion of the oval and round windows due to unequal impedance of these 2 structures. The resulting pressure difference across the basilar membrane enables sound perception. D, Increased bone conduction in third window anatomy. Due to shunting across third windows, there is decreased motion of the oval window on the scala vestibuli side of the cochlea. However, the motion of the round window on the scala tympani side is unchanged. This phenomenon artifactually elevates the pressure difference across the basilar membrane, resulting in increased sound perception. TM indicates tympanic membrane; yellow, auditory ossicles; beige, otic capsule; red, oval window; green, round window; blue, perilymph; purple, basilar membrane. Adapted with permission from Merchant SN, Rosowski JJ. Conductive hearing loss caused by third window lesions of the inner ear. Otol Neurotol 2008;29:282–89.
- Fig 2.
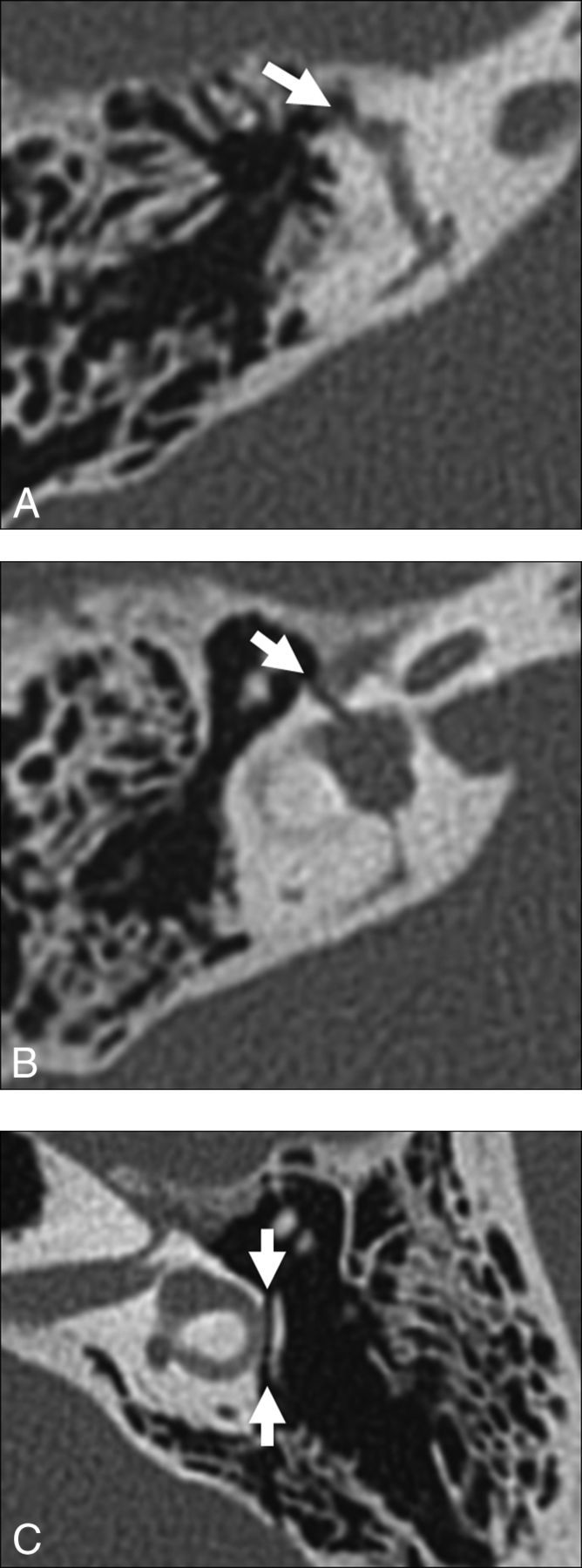
Temporal bone CT in the Pöschl (A) and Stenvers (B) planes demonstrating a large defect (arrows) in the roof of the right superior semicircular canal. C, Temporal bone CT Pöschl reconstruction demonstrates dehiscence of the left superior semicircular canal (arrow) into the superior petrosal sinus (S).
- Fig 3.
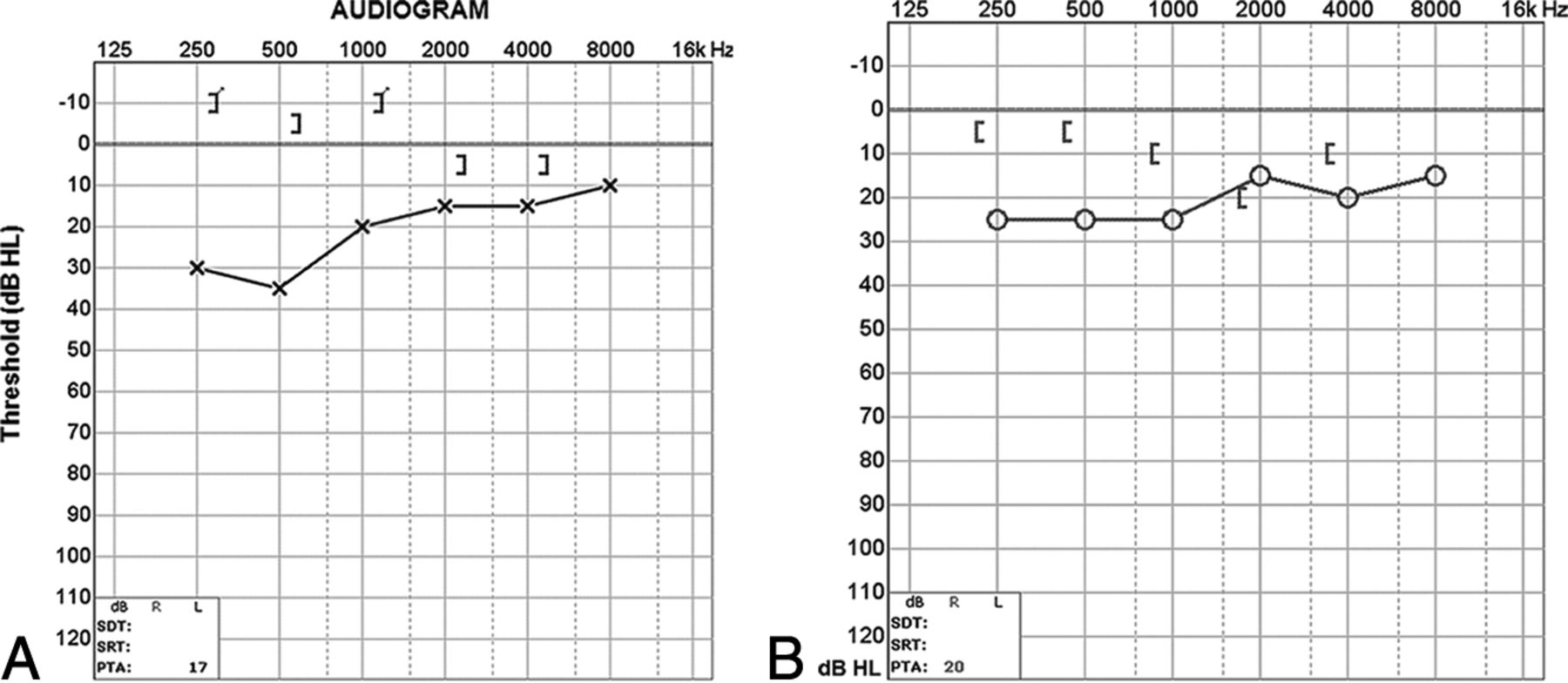
A, Audiogram of the right superior semicircular canal dehiscence with increased bone conduction (brackets) and decreased air conduction (crosses). The air-bone gap exceeds 10 dB at low sound frequencies (<1 kHz), the range at which acoustic energy is readily dissipated (described in the text). B, Audiogram of left superior semicircular canal dehiscence into the superior petrosal sinus. There is increased bone conduction (brackets) and decreased air conduction (circles), similar to typical SSCCD.
- Fig 4.
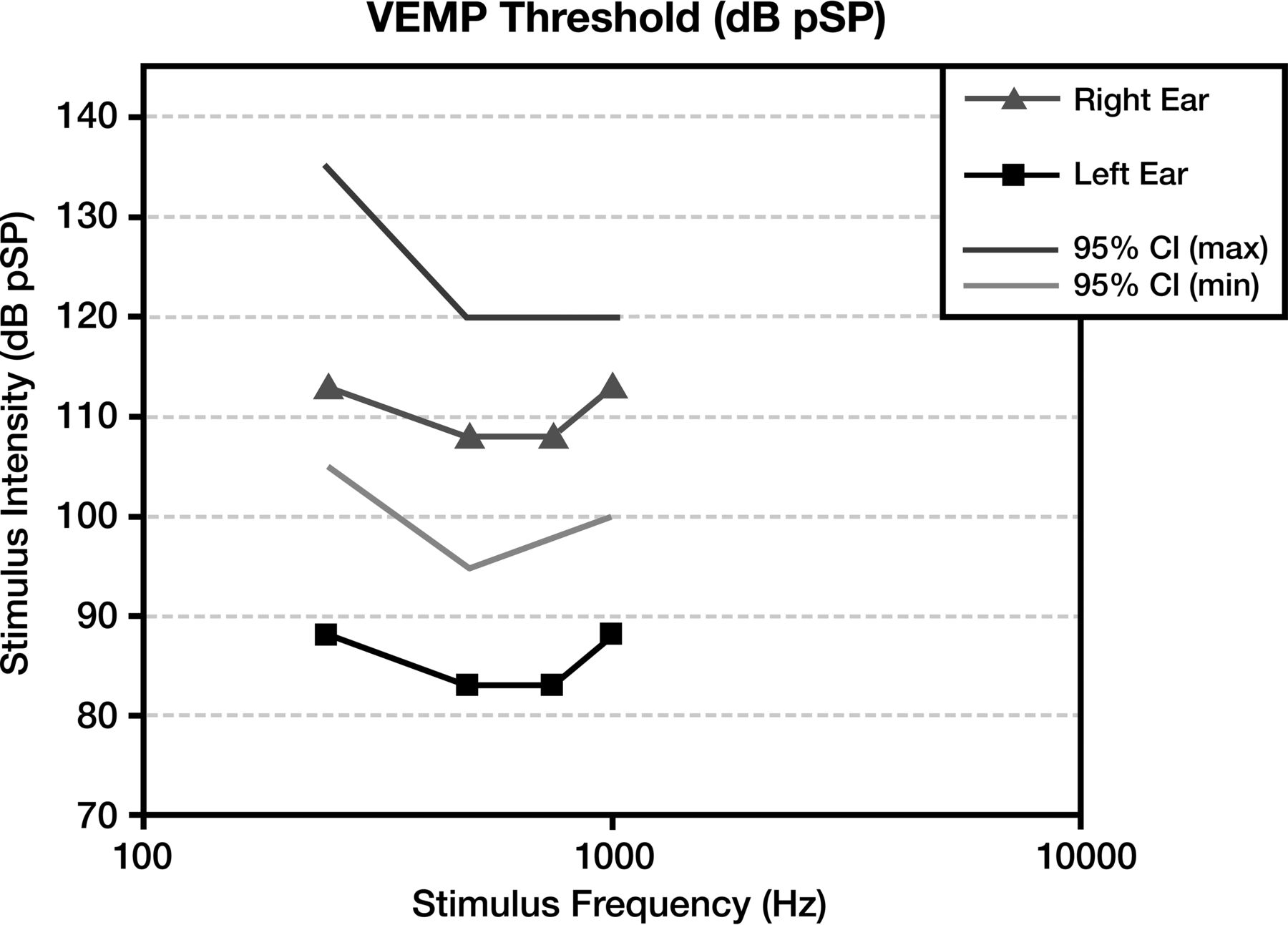
Vestibular-evoked myogenic potentials in superior semicircular canal dehiscence. Compared with the normal right ear (triangle) range (lines), the left ear demonstrates an abnormally sensitive response threshold (squares) across all tested stimulus frequencies. The lower thresholds indicate increased excitation of otolithic organs due to third window acoustic transmission.
- Fig 5.
Posterior semicircular canal dehiscence. Temporal bone CT in the coronal plane demonstrates a defect (arrow) in the roof of the posterior semicircular canal.
- Fig 6.
Audiogram of posterior semicircular canal dehiscence with increased bone conduction (brackets) and decreased air conduction (circles). Findings are compatible with posterior semicircular canal dehiscence (described in the text).
- Fig 7.
Inflammatory causes of perilabyrinthine fistula. A, Cholesteatoma. Axial CT shows an expansile, widely destructive soft-tissue mass centered in the middle ear with erosion into the cochlea, vestibule, and posterior semicircular canal (arrows). B, Recurrent otitis media. Axial CT identifies residual soft-tissue opacity in the middle ear, with a fistula (arrow) extending through the otic capsule into the lateral semicircular canal. C, Invasive fungal infection. Axial CT illustrates heterogeneous soft tissue centered in the middle ear, with invasion through the otic capsule into the lateral semicircular canal (arrow).
- Fig 8.
Audiogram of a cholesteatoma shows an air-bone gap of middle ear origin. There is decreased air conduction (crosses) relative to normal bone conduction (brackets). The resulting air-bone gap is present at both high and low sound frequencies. Given the background abnormality, it is not possible to detect the presence of superimposed third-window effects.
- Fig 9.
Carotid-cochlear dehiscence. Axial CT (A), Pöschl reformat (B), and Stenvers (A) reformat demonstrate communication between the apical turn of the cochlea and the carotid canal (arrows).
- Fig 10.
Audiogram of carotid-cochlear dehiscence. There is increased bone conduction (brackets) and decreased air conduction (circles), with a progressively larger air-bone gap at lower frequencies. In this case, the ipsilateral acoustic reflex was present, indicating that the ossicular chain was free to move with the action of the stapedius muscle. Therefore no middle ear pathology such as serous otitis, otosclerosis, or cholesteatoma was responsible for the air-bone gap.
- Fig 11.
Traumatic causes of perilabyrinthine fistula. A, Transverse temporal bone fracture through the superior semicircular canal (arrow). B, Transverse temporal bone fracture across the bony vestibule (arrow). C, Transverse temporal bone fracture through the otic capsule (arrows) with unroofing of the lateral semicircular canal.
- Fig 12.
Neoplastic causes of perilabyrinthine fistula. A, Squamous cell carcinoma. Axial CT scan shows destructive soft tissue filling the middle ear and eroding through the otic capsule (arrow). B, Facial nerve venous malformation. Axial CT scan shows a lobulated soft-tissue density extending from the geniculate ganglion (white arrow) through the otic capsule and into the superior semicircular canal (black arrow).
- Fig 13.
A, Enlarged vestibular aqueduct syndrome. Axial CT scan shows a dilated vestibular aqueduct (arrow) at its junction with the vestibule. B, Axial CT scan shows dehiscence of the vestibular aqueduct (arrow) into the jugular foramen (J).
- Fig 14.
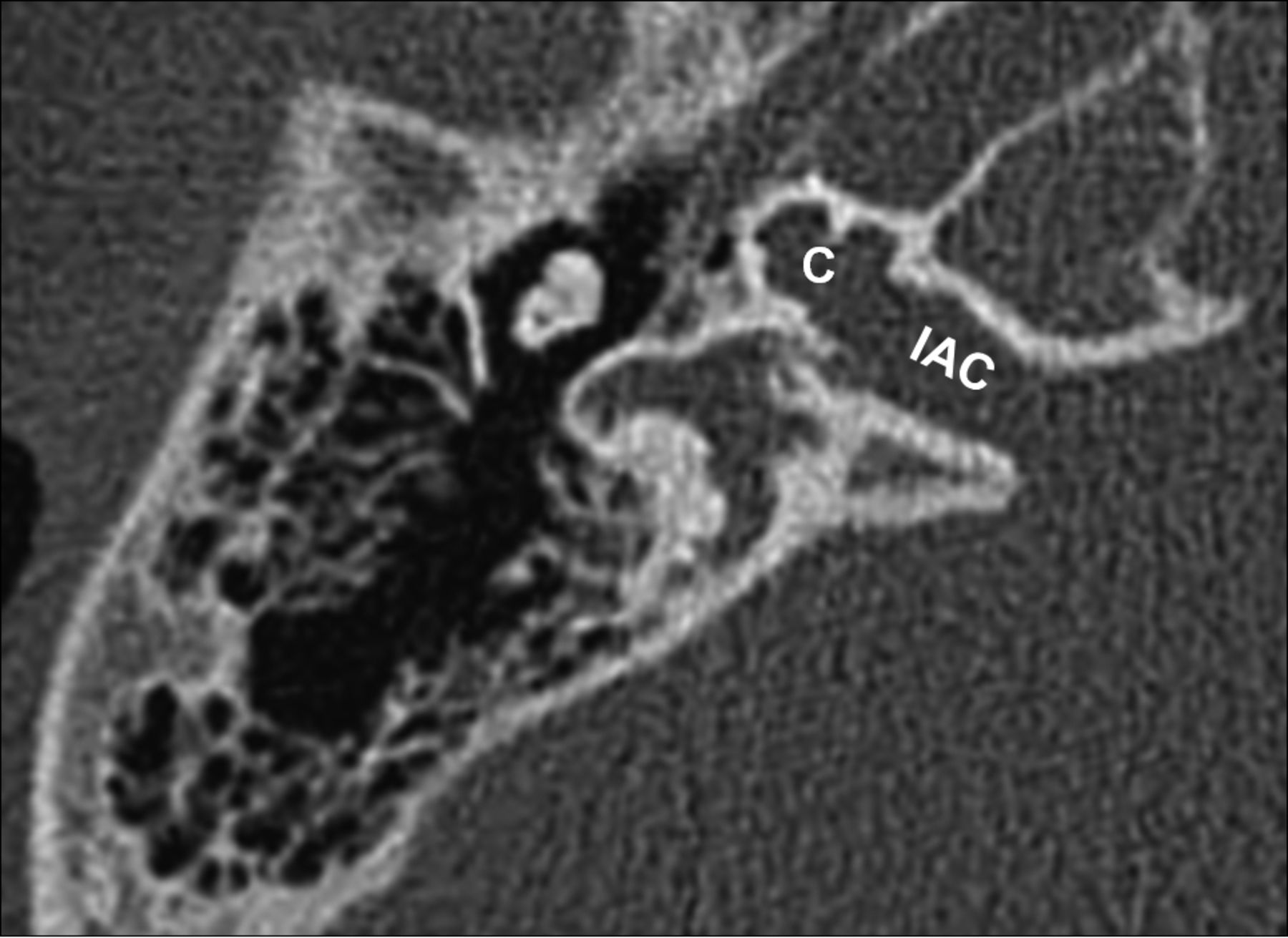
X-linked stapes gusher. Axial CT scan shows a dysplastic cochlea (C) with a modiolar deficiency and absence of the lamina cribrosa, resulting in a direct communication with an enlarged internal auditory canal (IAC).
- Fig 15.
Otospongiosis. A, Fenestral otospongiosis. Axial CT scan shows lucency at the fissula ante fenestram (arrow). B, Fenestral and retrofenestral otospongiosis. Axial CT scan shows lucency at the fissula ante fenestram (white arrow) and surrounding the cochlea (black arrows). C, Advanced otospongiosis. Axial CT scan late in the course of disease demonstrates a complete ring of pericochlear lucency.
- Fig 16.
Osteogenesis imperfecta. Axial CT scan shows otic capsule demineralization with multiple vague lucencies, including the fissula ante fenestram, pericochlear region, and area adjacent to the internal auditory canal. Radiologically, this is indistinguishable from otospongiosis.





















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}