
Abstract
SUMMARY: We noted enlargement of the internal auditory canal in several of our patients with posterior fossa malformations, hemangiomas, arterial anomalies, cardiac defects, eye abnormalities, and sternal or supraumbilical defects (PHACES) association and hence evaluated children with PHACES for the presence of an enlarged internal auditory canal and potential associated findings, including infantile hemangioma within the internal auditory canal, to understand the genesis of this enlargement. We reviewed our records to identify children with PHACES association who had been evaluated with MR imaging at our institutions. Imaging was reviewed for abnormal enhancement in the internal auditory canal, internal auditory canal enlargement, cerebellar hypoplasia, prominence of the petrous ridge, and deformity of the calvarium. We raise the possibility of an association between enlargement of the internal auditory canal in PHACES and a generalized malformation of the posterior fossa with cerebellar and calvarial hypoplasia.
ABBREVIATIONS:
- IAC
- internal auditory canal
- PHACES
- posterior fossa malformations, hemangiomas, arterial anomalies, cardiac defects, eye abnormalities, and sternal or supraumbilical defects
Posterior fossa malformations, hemangiomas, arterial anomalies, cardiac defects, eye abnormalities, and sternal or supraumbilical defects compose the PHACES association.1,2 The regional facial infantile hemangiomas of PHACES association are frequently associated with ipsilateral cerebellar hypoplasia and ipsilateral anomalies of the intracranial internal carotid artery.3,4 More recently, attention has been drawn to the incidence of intracranial hemangiomas, especially in the internal auditory canal (IAC) and cerebellopontine angle cistern.5⇓⇓–8 The purpose of this study was to document the incidence and imaging appearance of anomalies of the IAC and the potential for associated posterior fossa anomalies in patients with PHACES association.
Case Series
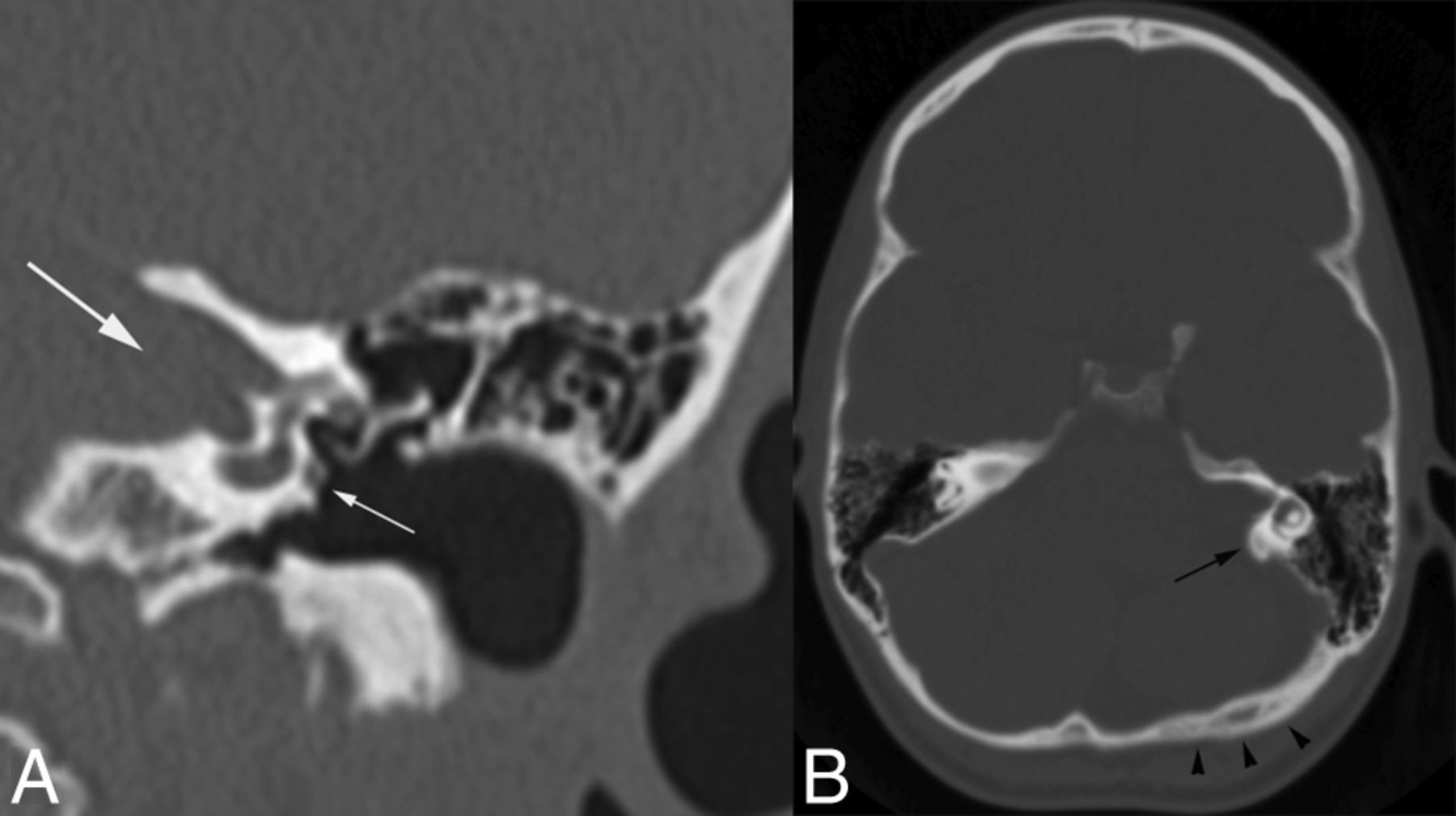
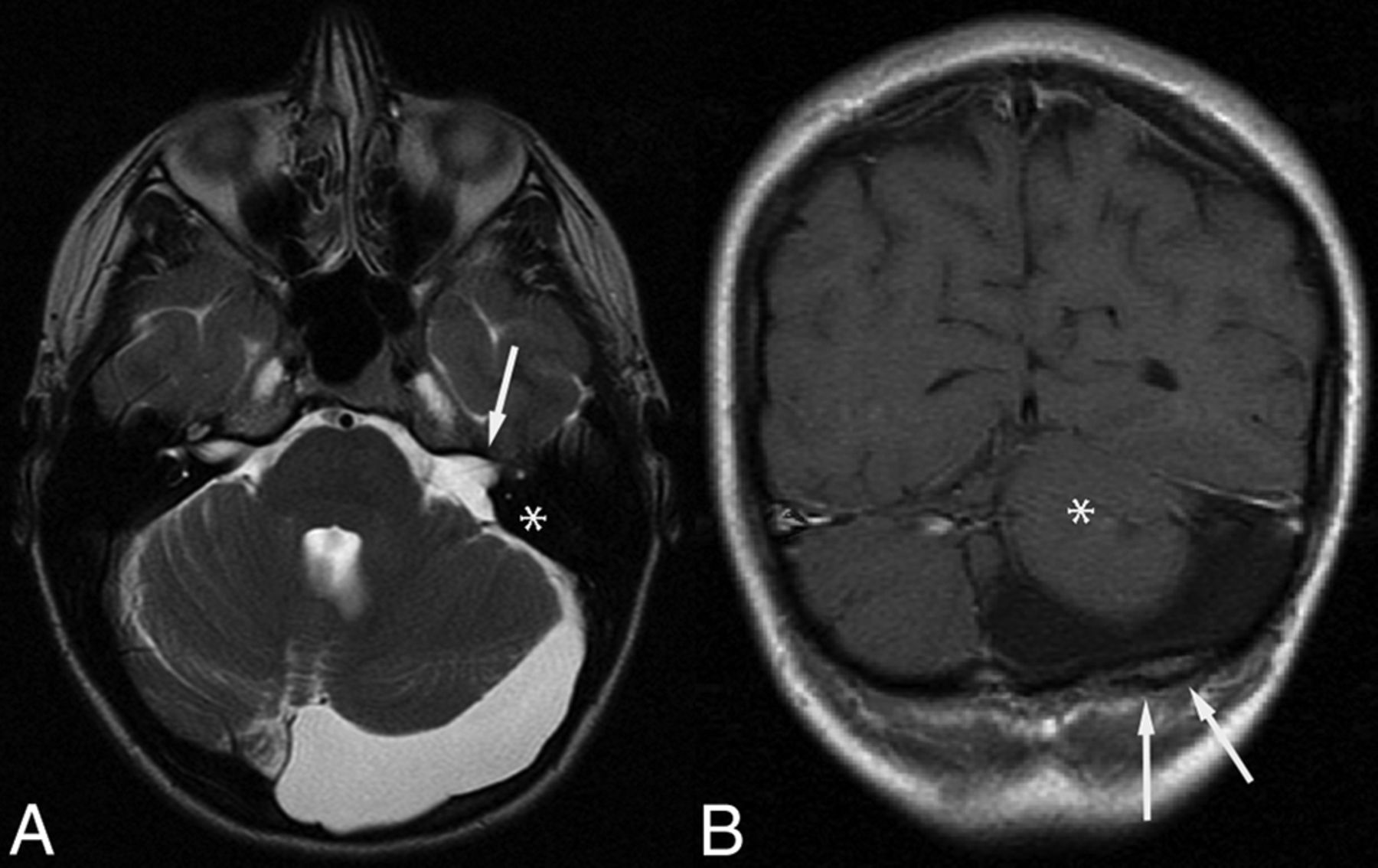
The index patient was a 25-year-old woman who presented with chronic hearing loss and a history of a facial hemangioma in infancy. Initial temporal bone CT revealed a funnel-shaped configuration of the prominent left IAC, prominence of the left posterior petrous ridge, hypoplasia of the left occipital bone, and findings consistent with a persistent left stapedial artery (Fig 1). Subsequent MR imaging demonstrated left cerebellar hypoplasia, enlargement of the left IAC, and an asymmetrically prominent left retrocerebellar CSF space (Fig 2). No abnormal enhancement was observed in the IAC or posterior fossa.

Coronal CT image of the left temporal bone (A) shows a prominent IAC (large white arrow) and a persistent stapedial artery (small white arrow). Axial CT image of the head (B) shows prominence of the left posterior petrous ridge (black arrow) and a relatively flattened, slightly thickened ipsilateral occipital calvarium (arrowheads).

MR imaging of the same adult patient as in Fig 1. Axial T2-weighted image (A) shows prominent CSF in the left posterior fossa, enlarged left IAC (white arrow), and prominence of the posterior petrous ridge (asterisk in A). B, Coronal postcontrast T1-weighted image. The left cerebellum is hypoplastic (asterisk in B), and there is subtle calvarial deformity with focal thickening of the diploic space (arrows in B).
Subsequent review of clinical data bases at 2 institutions identified 44 patients (37 male, 7 female) diagnosed with PHACES association who underwent diagnostic MR imaging of the brain between 2003 and 2012. Institutional review board approval was obtained from the 2 participating institutions for this retrospective review. A neuroradiologist with 9 years of experience and a pediatric neuroradiologist with 20 years of experience performed a consensus review of MR imaging examinations of the brain from pediatric patients with an established diagnosis of PHACES association based on accepted clinical criteria.
MR imaging techniques varied slightly among the patients, depending on the location of their scans and whether the brain examinations were modified for inclusion of imaging of the face to evaluate facial hemangiomas. Typically, axial T2-weighted images were obtained by using an FSE or TSE technique at section thicknesses ranging from 2.5 to 5 mm, with a 0- or 1-mm gap. Multiplanar postgadolinium T1-weighted images were acquired at a 3- to 5-mm section thickness with a 0- or 1-mm gap, with or without a fat-saturation technique. All MR imaging studies were evaluated for asymmetric caliber or contour of the IAC, intracanalicular enhancement, cerebellar asymmetry, and asymmetric size or morphology of the petrous and occipital bones (Fig 3). All abnormal findings were classified as ipsilateral or contralateral to the patients' facial hemangiomas (Fig 4).

A 6-month-old girl. Axial (A) and coronal (B) T2-weighted images show unilateral enlargement and downsloping of the right IAC (white arrows). Note ipsilateral cerebellar hypoplasia (asterisk in A) and prominence of the posterior petrous ridge (black arrow). Additional coronal T2-weighted image (C) shows mild occipital calvarial flattening (arrowheads) ipsilateral to the cerebellar hypoplasia.

A 26-month-old girl. Axial T2-weighted image shows a right facial hemangioma (white arrow), ipsilateral to the enlarged right IAC (black arrow), and cerebellar hypoplasia (asterisk).
Nineteen of 44 (43%) cases demonstrated unilateral funnel-shaped IAC enlargement; this group of 19 patients included 16 female and 3 male patients between 8 days and 18 years of age (average age, 40 months) at the time of initial MR imaging. IAC enlargement was ipsilateral to the facial hemangioma in 17/19 patients and contralateral in 1/19. One patient with enlargement of the left IAC had bilateral facial hemangiomas.
Fifteen of 19 patients with unilateral IAC enlargement underwent contrast-enhanced thin-section imaging through the posterior fossa during the first 3 years of life. Of the remaining 4 patients, 3 were initially imaged with intravenous contrast at ages 8, 17, and 18 years. One neonate did not receive intravenous contrast.
Of the 15 patients in whom MR imaging was performed with contrast during the first 3 years of life, 6 had avidly enhancing IAC masses consistent with hemangiomas. Asymmetric IAC enhancement without a discrete mass was identified in 1 patient. Follow-up studies were available on 4 of these 7 patients, all of which demonstrated resolution of enhancement or reduction in lesion size (Fig 5). IAC enhancement was ipsilateral to the facial hemangioma in 7/7 patients. Resolution of IAC enhancement appeared to parallel resolution of the facial hemangiomas.

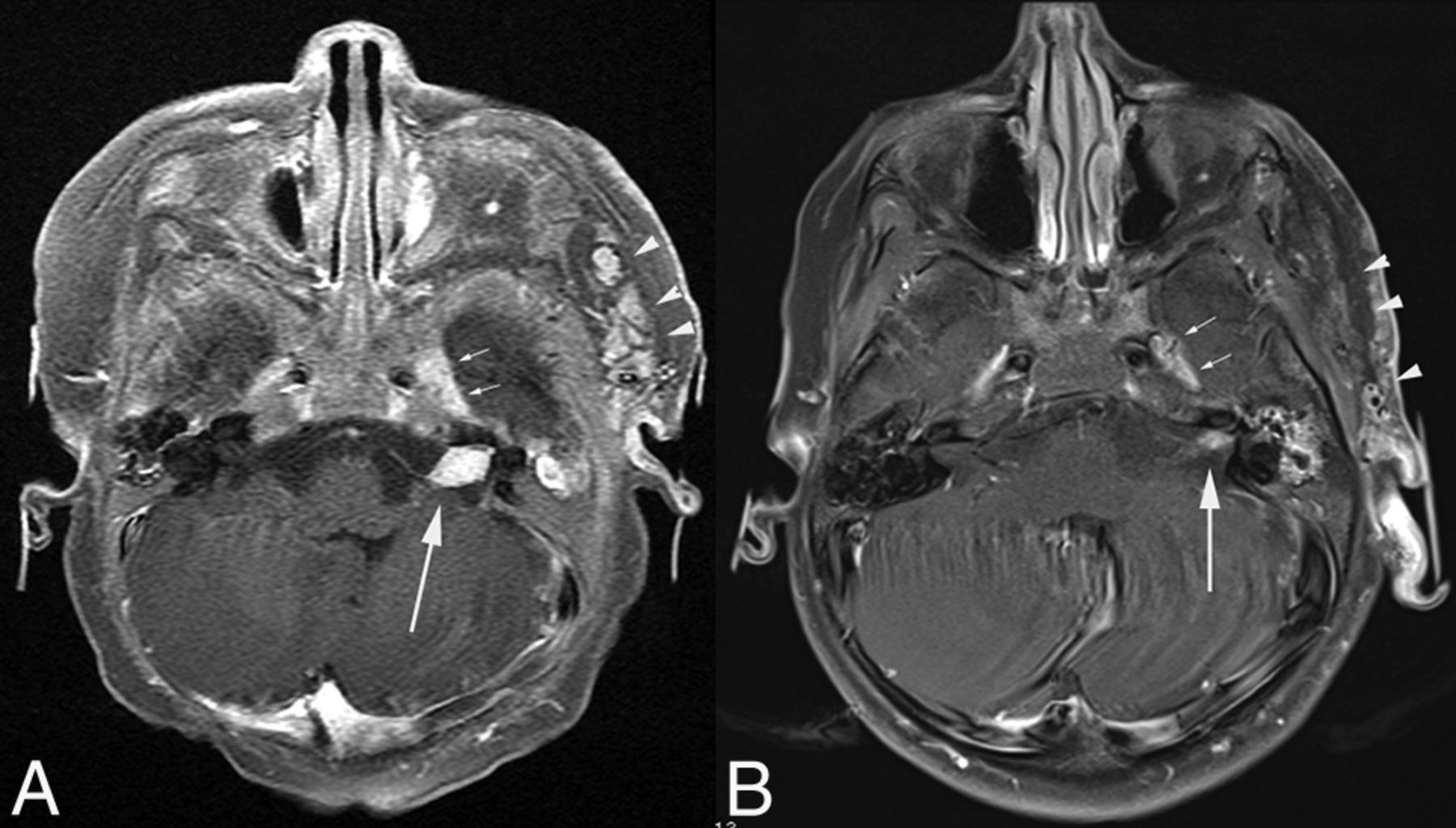
A 4-month-old girl. Axial postcontrast fat-suppressed T1-weighted images show an enhancing mass in the left IAC (arrow in A), which markedly diminishes in size on follow-up imaging at 3 years of age (arrow in B). Note the ipsilateral left facial and preauricular hemangioma, which similarly involutes (arrowheads in A and B). Note also mild prominence of the left cavernous sinus, thought to harbor an additional small hemangioma (small arrows in A and B). Minimal left cerebellar hypoplasia was better demonstrated on T2-weighted images (not shown).
In 2 of the 7 patients with IAC enhancement, there was also abnormal enhancement within the fourth ventricle, consistent with an additional intracranial hemangioma. Involution of this enhancement also paralleled the involution of the facial hemangioma (Fig 6).

A 3-month-old boy. A, Axial postcontrast T1-weighted image shows an enhancing mass in the right IAC (white arrow). There is also abnormal enhancement in the fourth ventricle (black arrow), suspicious for an additional hemangioma. B, Fifteen-month follow-up imaging of the same patient. Fat-suppressed T1-weighted image shows diminished enhancement in the right IAC (white arrow). The previously seen enhancement in the fourth ventricle is also less conspicuous, beginning to resemble normal choroidal enhancement (black arrow). The cerebellum appears normal.
Of the 7 patients with IAC enhancement, 6 demonstrated prominence of the ipsilateral posterior petrous ridge, 5 had ipsilateral cerebellar hypoplasia, and 5 had a deformity of the ipsilateral occipital bone.
Of the 12 patients without documented IAC enhancement, 10 demonstrated prominence of the ipsilateral posterior petrous ridge, 11 had ipsilateral cerebellar hypoplasia, and 11 had a deformity of the ipsilateral occipital bone.
Overall, 13/19 patients demonstrated a combination of enlargement of the IAC, ipsilateral cerebellar hypoplasia, prominence of the ipsilateral posterior petrous ridge, and deformity of the ipsilateral occipital bone.
The findings discussed above are summarized in the Table.
Posterior fossa anomalies in 19 patients with PHACES with IAC enlargement
Discussion
Approximately 36% of the pediatric patients with enlarged IACs imaged with contrast-enhanced MR imaging during the first 3 years of life had abnormal IAC enhancement indicating the presence of an ipsilateral IAC hemangioma. The percentage increased to 70% of patients when imaging was performed during the first year of life.
One limitation to the detection of IAC hemangioma is the requirement of MR imaging during infancy with intravenous contrast and thin-section, high-resolution T1-weighted images through the IAC. In 1 patient, the examination during infancy was performed without sedation, following feeding and swaddling, and contrast was not administered. In another, the initial facial lesion was mistaken for a port-wine stain, and imaging before 2 years of age was performed for evaluation of possible Sturge-Weber syndrome. Eight patients underwent initial imaging beyond infancy, at which time any intracranial hemangioma would presumably have involuted.
Eighty-four percent of patients with IAC enlargement had ipsilateral prominence of the petrous ridge, 79% had ipsilateral cerebellar hypoplasia, and 79% had ipsilateral abnormality of the overlying calvarium. Sixty-eight percent of the patients with IAC enlargement had all 3 of these findings. This result would suggest that the enlarged IAC may be part of a spectrum of related posterior fossa abnormalities in a subset of patients with PHACES association, possibly due to abnormal embryogenesis, but 28% of patients with IAC enhancement did not have cerebellar hypoplasia or occipital deformities.
All 19 patients with IAC enlargement had segmental facial hemangiomas as expected in PHACES association. All except 1 of the facial hemangiomas were ipsilateral to their posterior fossa anomalies, consistent with the prevailing theories regarding the underlying pathogenesis of conditions such as PHACES association. PHACES is an example of a metameric association, similar to other entities such as cerebrofacial venous metameric syndromes and cerebrofacial arteriovenous metameric syndromes. These syndromes share an underlying etiology related to the cephalic migration of neural crest cells.9⇓–11
Cerebrofacial venous metameric syndromes and cerebrofacial arteriovenous metameric syndromes tend to have an axial, segmentally arranged distribution of lesions, with lesions in a single metamere. In contrast, the anomalies in PHACES (sternal, aortic, arterial, ocular, and posterior fossa) suggest a longitudinal dysfunction in the migration of the cephalic neural crest cells. Krings et al9 suggested that the association between hemangiomas of the cerebellopontine angle and ipsilateral agenesis of the ICA indicates links between migrational aberrations affecting the third aortic arch, the third branchial arch, and the rhombencephalon.
Although the presence or absence of a hemangioma in the IAC or cerebellopontine angle cistern could be incidental to the other posterior fossa findings described, a hemangioma in this region occurs with a frequency that suggests, at least in some cases, a causal relationship. In addition, the demonstration of unilateral cerebellar hypoplasia with ipsilateral funnel-shaped IAC enlargement later in childhood or in adulthood may be helpful in suggesting a diagnosis of PHACES association. This finding is useful in distinguishing PHACES association from other causes of cerebellar hypoplasia. Detection of fetal cerebellar hypoplasia, particularly when unilateral, should prompt consideration of PHACES association in the differential diagnosis. A diagnosis of PHACES association should prompt questioning about a history of prior regional infantile hemangioma and a critical assessment with MR imaging and MRA for associated intracranial arterial anomalies and/or steno-occlusive disease.
Conclusions
We demonstrate a high incidence of funnel-shaped IAC enlargement in patients with PHACES association, and many of these patients were found to have hemangiomas within the enlarged IAC, particularly when scanned with contrast-enhanced MR imaging during the first year of life. Those patients with IAC enlargement, in the presence or absence of an enhancing mass, have a high incidence of abnormalities of the petrous bone, occipital bone, or cerebellum The results raise the possibility that the enlarged IAC in PHACES is related to a generalized malformation of the osseous components of the posterior fossa, in association with cerebellar hypoplasia and sometimes with IAC hemangioma. Unilateral enlargement of the IAC in an adult patient without an apparent mass in the IAC should prompt questioning and evaluation for possible PHACES association.
Footnotes
Disclosures: Caroline D. Robson—UNRELATED: Royalties: Amirsys, Comments: Editor and content author. Francine Blei—UNRELATED: Consultancy: Pierre Fabre, Comment: Medical Advisory Board; Grants/Grants Pending: Pierre Fabre,* Comments: Burden of Disease (Infantile Hemangiomas) Study. *Money paid to the institution.
Paper previously presented as an electronic poster at: American Society of Neuroradiology Annual Meeting and the Foundation of the ASNR Symposium, May 18–23, 2013; San Diego, California.
References
- Received December 31, 2013.
- Accepted after revision March 17, 2015.
- © 2015 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}