
Abstract
BACKGROUND AND PURPOSE: Gadobenate dimeglumine has markedly higher R1 relaxivity compared to gadopentetate dimeglumine meaning that lower doses can be used to achieve similar contrast enhancement. Our aim was to prospectively compare single-dose gadobenate dimeglumine with double-dose gadopentetate dimeglumine for contrast-enhanced MRA of the supra-aortic vasculature.
MATERIALS AND METHODS: Forty-six patients (37 men, 9 women; mean age, 63.5 ± 10.1 years) with known or suspected steno-occlusive disease of the supra-aortic vessels underwent 2 identical CE-MRA examinations at 1.5T. Contrast agents were administered in randomized order, with the 2-fold greater volume of gadopentetate dimeglumine injected at a 2 times faster rate. Image assessment was performed by 3 independent blinded readers for vessel anatomic delineation, detection/exclusion of pathology, and global preference. Diagnostic performance (sensitivity, specificity, accuracy, PPV, and NPV) for detection of ≥60% stenosis was determined for 39/46 patients who underwent preinterventional DSA. Data were analyzed by using the Wilcoxon signed-rank, McNemar, and Wald tests in terms of the noninferiority of single-dose gadobenate dimeglumine compared with double-dose gadopentetate dimeglumine. Quantitative enhancement (signal-to-noise ratio (SNR), contrast-to-noise ratio (CNR)) was also compared.
RESULTS: All images were technically adequate. No differences (P = 1.0) were noted by any reader for any qualitative parameter. All readers considered single-dose gadobenate dimeglumine and double-dose gadopentetate dimeglumine equivalent in at least 42/46 patients (91.3% three-reader agreement) for all parameters. Nonsignificant superiority for gadobenate dimeglumine was reported for all diagnostic performance indicators (sensitivity: 82.7%–88.5% versus 75.0%–80.8%; specificity: 96.4%–98.6% versus 94.6%–98.6%; accuracy: 94.6%–96.1% versus 92.4%–94.9%; PPV: 81.5%–91.5% versus 73.7%–90.7%; NPV: 96.8%–97.8% versus 95.4%–96.4%). No differences (P > .05) in quantitative enhancement were noted.
CONCLUSIONS: The image quality and diagnostic performance achieved with 0.1-mmol/kg gadobenate dimeglumine is at least equivalent to that achieved with 0.2-mmol/kg gadopentetate dimeglumine.
ABBREVIATIONS:
- CE-MRA
- contrast-enhanced MRA
- CI
- confidence interval
- MIP
- maximum intensity projection
- NPV
- negative predictive value
- PPV
- positive predictive value
Comparatively recent meta-analyses to determine the accuracy of contrast-enhanced MRA for the detection of severe carotid stenosis (70%–99% luminal narrowing) have reported sensitivity and specificity values of approximately 94% and 92%, respectively.1⇓–3 Many of the included studies, however, used either a double dose of gadolinium contrast agent or a standard volume of 25–30 mL (corresponding to 0.17–0.2 mmol/kg for a 75-kg patient). Although some studies have used lower doses, this use has often been associated with compromised spatial resolution and image quality.4 The risk of nephrogenic systemic fibrosis in patients with severe renal insufficiency and its possible association with high-dose administrations has refocused attention on the need to minimize the dose whenever possible.5
To date, few studies have compared contrast agent doses for supra-aortic CE-MRA. Published studies have used either an interindividual parallel group design in which subjects receive one or the other dose but not both5,6 or an intraindividual crossover design in which subjects receive both doses in otherwise identical examinations.7,8 Unfortunately, the former group is limited in that findings are subject to between-group variations in patient- and/or disease-related factors, while the latter group has typically evaluated relatively small populations of healthy volunteers7 or patients.8 Moreover, a reference technique (eg, DSA) was used in only a few patients in just one of the studies,5 thereby precluding the possibility of drawing meaningful conclusions regarding clinical impact.
In this study, we compared single-dose gadobenate dimeglumine (MultiHance; Bracco Imaging, Milan, Italy) with double-dose gadopentetate dimeglumine (Magnevist; Bayer Healthcare, Berlin, Germany) by using a multicenter intraindividual crossover study design. Whereas both agents have a linear ionic molecular structure and are widely used for CE-MRA, they differ in that gadobenate dimeglumine possesses markedly higher R1 relaxivity in vivo (6.3–7.9 compared with 3.9–4.1 L × mmol−1 × second−1 at 1.5T9,10). Numerous studies across a range of CE-MRA applications have shown that gadobenate dimeglumine is superior to gadopentetate dimeglumine in terms of diagnostic performance and/or contrast enhancement and image quality when these agents are administered at equivalent doses.11⇓–13 Similarly, intraindividual crossover comparisons between single-dose gadobenate dimeglumine and double-dose gadopentetate dimeglumine have revealed equivalent or better imaging performance with the former agent and dose.8,14 The present study extends these investigations to assess the diagnostic performance achieved on CE-MRA of the supra-aortic vasculature with single-dose gadobenate dimeglumine relative to double-dose gadopentetate dimeglumine by using DSA as reference standard.
Materials and Methods
The study was a Phase III randomized crossover comparison of 0.1-mmol/kg gadobenate dimeglumine and 0.2-mmol/kg gadopentetate dimeglumine for CE-MRA of the supra-aortic arteries. The study was registered at www.clinicaltrials.gov (reference NCT01260636). Institutional review board and regulatory approval were granted from each center, and all enrolled patients provided written informed consent.
Patients
Patients with moderate-to-severe renal impairment (glomerular filtration rate or estimated glomerular filtration rate <60 mL/min/1.73 m2), congestive heart failure (New York Heart Association classification IV), or a known allergy to either agent were ineligible for enrollment. Patients were also ineligible if they had received or were scheduled to receive another contrast medium in the 24 hours preceding until 24 hours following either examination or any other investigational compound and/or medical device within 30 days before until 24 hours after administration of the second agent or were scheduled to undergo any intervention for arterial occlusive disease between the 2 examinations. Finally, patients were ineligible if they were pregnant or lactating or if they had any medical condition or other circumstance (eg, metallic vascular stent, pacemaker, severe claustrophobia) that would decrease the chances of obtaining an adequate examination or which would preclude proximity to a strong magnetic field.
Of 52 screened adult patients, 46 with suspected steno-occlusive disease of the supra-aortic vasculature or clinical symptoms of cerebral ischemia were deemed eligible for the study and were enrolled at 3 sites in China between December 2009 and December 2011. The 3 centers enrolled 19, 16, and 11 patients. Eligible patients were randomized to 2 groups. Patients randomized to group A (n = 24) received gadobenate dimeglumine for the first examination and gadopentetate dimeglumine for the second; patients randomized to group B (n = 22) received the agents in reverse order.
MRA Examinations
CE-MRA was performed at 1.5T by using scanners (Avanto [n = 30], Sonata [n = 16]; Siemens, Erlangen, Germany) equipped with a gradient system of at least 40 mT/m. The supra-aortic vasculature from the brachiocephalic trunk up to and including the carotid bifurcation and the extracranial internal carotid artery was imaged in each examination.
The image-acquisition parameters varied slightly between centers within a narrow range (TR: 3.4–3.58 ms; TE: 1.14–1.29 ms; flip angle: 30°; excitations: 1; FOV: 184 × 280–300 × 300; matrix: 320 × 200–384 × 240; section thickness: 0.7-1.3 mm; acquisition time: 13–19 seconds), though both examinations in each patient were identical in terms of orientation, FOV, sequence parameters, and spatial resolution. The interval between examinations in each patient ranged between 3 and 5 days.
CE-MRA was performed after administration of 0.1-mmol/kg (0.2-mL/kg) gadobenate dimeglumine or 0.2-mmol/kg (0.4-mL/kg) gadopentetate dimeglumine. The mean volume of gadobenate dimeglumine administered was 13.8 ± 2.5 mL (range: 6.8–20 mL) injected at a mean rate of 1.4 ± 0.24 mL/s (range: 0.7–2.0 mL/s). To ensure identical bolus geometry for the 2 examinations in each patient, we administered the 2-fold greater volume of gadopentetate dimeglumine at a 2-fold faster rate. All injections were made by power injector and flushed with 20-mL saline. Timing for the CE-MRA sequence was based on automatic bolus detection (Care Bolus [Siemens] in 35 subjects; MR fluoroscopic triggering in 11 subjects). The approach to sequence timing was the same for both examinations in each patient.
MRA Image Assessment
Image assessment was performed by 3 independent radiologists (Y.L., X.W., F.D.C.; each with ≥12 years' experience in CE-MRA) who were unaffiliated with the study sites and blinded to patient information and contrast agent. Images were evaluated in matched pairs; in each case, axial source images and volumetric maximum-intensity-projection reconstructions from the 2 examinations in each patient were managed by using an AquariusNET client server (Version 4.4.5.36; TeraRecon, San Mateo, California) and displayed simultaneously on 2 monitors. Evaluations were performed by using a segmentation scheme comprising 9 arterial segments covering the brachiocephalic trunk (segment 1), subclavian arteries (segments 2 and 3), common carotid arteries (segments 4 and 5), carotid bifurcations (segments 6 and 7), and extracranial ICA (segments 8 and 9).
Image evaluation was performed initially for technical adequacy (adequate/inadequate; images were inadequate if the vessels of interest were outside the scanning volume or if the acquisition was mistimed). Thereafter, qualitative assessments were made of vessel anatomic delineation, disease detection/exclusion, and global preference in the neck vessels and carotid bifurcation/extracranial ICA. All qualitative comparisons were performed by using 3-point scales from −1 (examination 1 superior) through 0 (examinations equal) to +1 (examination 2 superior).
Quantitative measurements of signal intensity were made by each reader at regions of interest positioned in 1 vessel in the neck and in either the carotid bifurcation or the extracranial ICA. Additional ROIs were positioned in muscle in the same image as that of the vessel ROI. ROIs were typically circular and large enough (≥0.5 cm2) to obtain reliable measurements at areas of maximum signal intensity within the lumen and on homogeneous regions of muscle. Region-of-interest positioning was similar for the 2 examinations in each patient. Signal intensity measurements were made on a pixel-by-pixel basis by using quantitative analysis software in the Aquarius ET server. The signal intensity values recorded within each ROI were used to calculate the signal-to-noise ratio and contrast-to-noise ratio according to the equations below in which SIvessel represents the signal intensity measured in the vessel, SImuscle represents the signal intensity measured in the muscle in the same image and noise represents the SD of the signal intensity in the muscle.

Diagnostic Performance
Digital Subtraction Angiography.
The 46 enrolled patients included 39 who also underwent conventional DSA. DSA was performed from 2–5 days before the first CE-MRA examination or from 0–20 days after the second CE-MRA examination by injecting an iodinated contrast medium through a pigtail or straight 4F–5F catheter inserted via a femoral artery puncture by using the Seldinger technique. The approach to DSA was at the discretion of the investigating center and involved imaging of 1 or 2 sides. Images were acquired by using anteroposterior and right and/or left anterior oblique projections. All DSA examinations were performed by using contrast media with an iodine concentration of ≥300 mg I/mL. The mean total volume administered was 110.9 ± 25.6 mL (range: 40–167 mL). Injections of 15–40 mL were administered at rates of 2–20 mL/s, depending on the vessel of interest. Angiograms were obtained by using a 1024 × 1024 matrix.
Assessment of Diagnostic Performance.
Evaluation of DSA images was performed by a radiologist (R.I., with >15 years' experience) who was unaffiliated with the study centers and blinded to all clinical and radiologic information. Images were managed and displayed in randomized order by using DICOMed Review Version 4.0 software (AetMed, Genova, Italy). The presence and extent of disease was determined segmentally by using a 4-point scale in which 1 = a vessel with no or mild stenosis (<30%), 2 = a vessel with moderate stenosis (≥30% but <60%), 3 = a vessel with clinically relevant disease (≥60% to <100%), and 4 = a vessel with occlusion (100% lumen blockage). The presence and grading of stenoses were in all cases performed qualitatively. There was no use of digital calipers to determine the degree of stenosis. Stenoses detected at DSA were labeled for subsequent lesion matching with findings from the blinded reading of CE-MRA images.
CE-MRA images were randomized and evaluated separately and independently in a blinded fashion by using the same qualitative criteria used for the DSA assessment. Stenoses detected at CE-MRA were labeled on MIP images for lesion matching.
Safety Assessments
All subjects were monitored for adverse events for 24 hours after administration of each agent. Measurements of vital signs were made immediately before and at 30 minutes and 24 hours after each examination. Evaluation of laboratory parameters was performed on samples acquired within 24 hours before and within 24 hours after each administration.
Statistical Analysis
The study was powered to show a 4:1 ratio of diagnostic preference for either contrast agent with an effect size of 0.23 and assuming an “equal” response in 50% of cases. Based on a χ2 test of specified proportions in 3 categories (nQuery, Version 5.0; Statistical Solutions, Cork, Ireland), 48 subjects were needed for 85% of power at an α level of .05.
Comparison of diagnostic preference, vessel anatomic delineation, and pathology detection/exclusion was performed by using the Wilcoxon signed-rank test. Comparison of quantitative enhancement was performed by using a mixed model with subject, period, sequence, and contrast agent group as variables.
Determinations of diagnostic performance (sensitivity, specificity, accuracy, positive and negative predictive values, and 95% confidence intervals) for the detection of clinically relevant disease [≥60% stenosis or occlusion]) were performed by using DSA as a reference standard. Differences in sensitivity, specificity, and accuracy were compared by using a paired binary approach. Noninferiority for 0.1-mmol/kg gadobenate dimeglumine compared with 0.2-mmol/kg gadopentetate dimeglumine was demonstrated if the lower limit of the 95% CI was within −5%. We compared differences in PPV and NPV by using the Wald test derived from a generalized estimating equation, with intra-individual correlation taken into account.
Inter-reader agreement was determined by using generalized weighted kappa (κ) statistics and was measured as percentage agreement. Agreement was classified as excellent (κ values >0.8), good (κ = 0.61–0.8), moderate (κ = 0.41–0.6), fair (κ = 0.21–0.4), or poor (κ ≤ 0.2).
All statistical tests were 2-sided at the P < .05 level of significance and were performed by using SAS, Version 9.2 (SAS Institute, Cary, North Carolina).
Results
Forty-six patients (37 men, 9 women; mean age, 63.5 ± 10.1 years; range, 33–80 years) underwent CE-MRA to confirm or evaluate a previously detected stenosis (23/46 [50%]), because of clinical symptoms suggestive of stenosis (3/46 [6.5%]), or to guide revascularization (20/46 [43.5%]). Patients were randomized to group A (19 men, 5 women; mean age, 63.6 ± 9.4 years) or B (18 men, 4 women; mean age, 63.5 ± 11.0 years). There were no between-group differences in sex (P = .821), age (P = .978), or weight (P = .905). All patients received both agents and were evaluated for safety; no patient discontinued before study completion.
DSA was performed in 39/46 (84.8%) patients (22 from group A, 17 from group B). There were no between-group differences in sex (P = .679), age (P = .901), or weight (P = .536).
Image Assessment
Ninety-two vascular stations (46 neck + 46 bifurcation/ICA stations) were considered within the FOV across the 46 evaluated patients. All 92 stations were considered technically adequate after both examinations.
Qualitative Evaluation
Reader assessment of qualitative enhancement in matched pairs revealed no difference between 0.1-mmol/kg gadobenate dimeglumine and 0.2-mmol/kg gadopentetate dimeglumine (Table 1). Three-reader agreement was noted for 84.8%–91.3% of patients, depending on the end point.
Qualitative assessment of images from 46 patients in matched pairs
Quantitative Evaluation
Quantitative enhancement in the neck and carotid bifurcation/ICA was similar (Fig 1). Although each reader noted slightly greater SNR and CNR with 0.1-mmol/kg gadobenate dimeglumine in the neck, none of the differences were significant.

Mean signal-to-noise ratio (A) and contrast-to-noise ratio (B) after 0.1-mmol/kg gadobenate dimeglumine and 0.2 mmol/kg gadopentetate dimeglumine as determined by 3 independent blinded readers.
Diagnostic Performance
A total of 340 arterial segments were within the FOV across the 39 patients who underwent DSA. Of these segments, 332 (97.6%) were considered technically adequate and 8, (2.4%) technically inadequate. Readers 1, 2, and 3 considered 332, 332, and 332 segments following gadobenate dimeglumine and 332, 331, and 331 segments following gadopentetate dimeglumine to be in the FOV on CE-MRA and to match technically adequate segments on DSA.
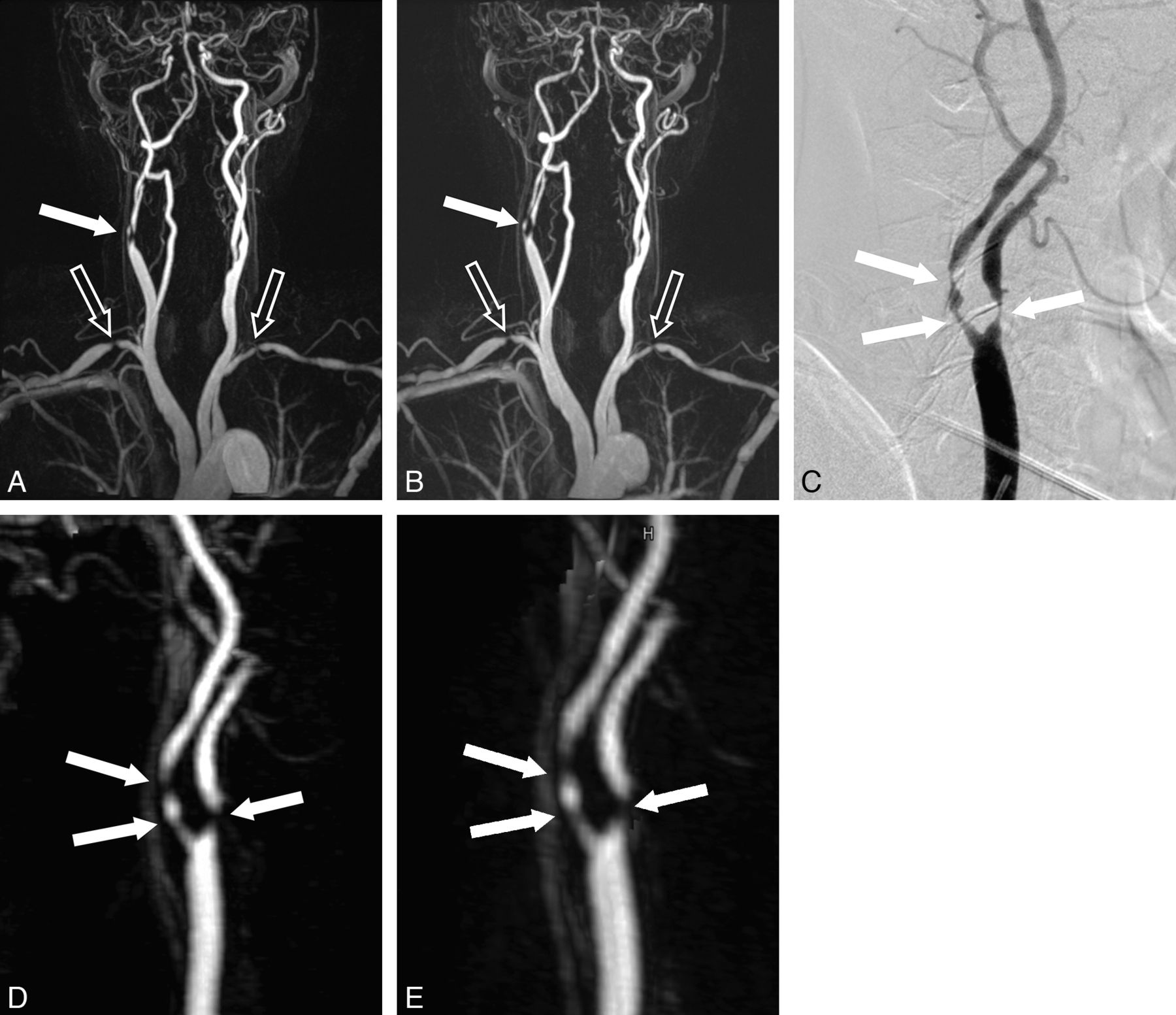
The diagnostic performance of CE-MRA for the detection of hemodynamically relevant stenosis is summarized in the On-line Table. Consistently superior performance was noted for gadobenate dimeglumine relative to gadopentetate dimeglumine, with significant superiority noted by reader 2 for determinations of accuracy (95.8% versus 92.4%, P = .016) and PPV (85.2% versus 73.7%, P = .008). Examples of the comparable quality and diagnostic efficacy achieved with 0.1-mmol/kg gadobenate dimeglumine and 0.2-mmol/kg gadopentetate dimeglumine are shown in Figs 2 and 3.

A 72-year-old male patient referred for MR imaging to guide revascularization of symptomatic carotid artery stenosis. The MIP image (A) acquired after 0.1-mmol/kg gadobenate dimeglumine (8 mL injected at 0.8 mL/s) reveals severe stenosis in both the left and right subclavian arteries (open arrows) and a ≥60% stenosis (closed arrow) of the right carotid bifurcation/ICA. Similar findings are seen on the analogous MIP image (B) acquired after 0.2-mmol/kg gadopentetate dimeglumine (16 mL injected at 1.6 mL/s). Selective DSA of the right carotid bifurcation/ICA (C) confirms the findings of the CE-MRA examinations after gadobenate dimeglumine (D) and gadopentetate dimeglumine (E). Note the sharper vessel delineation and greater contrast enhancement achieved with gadobenate dimeglumine.

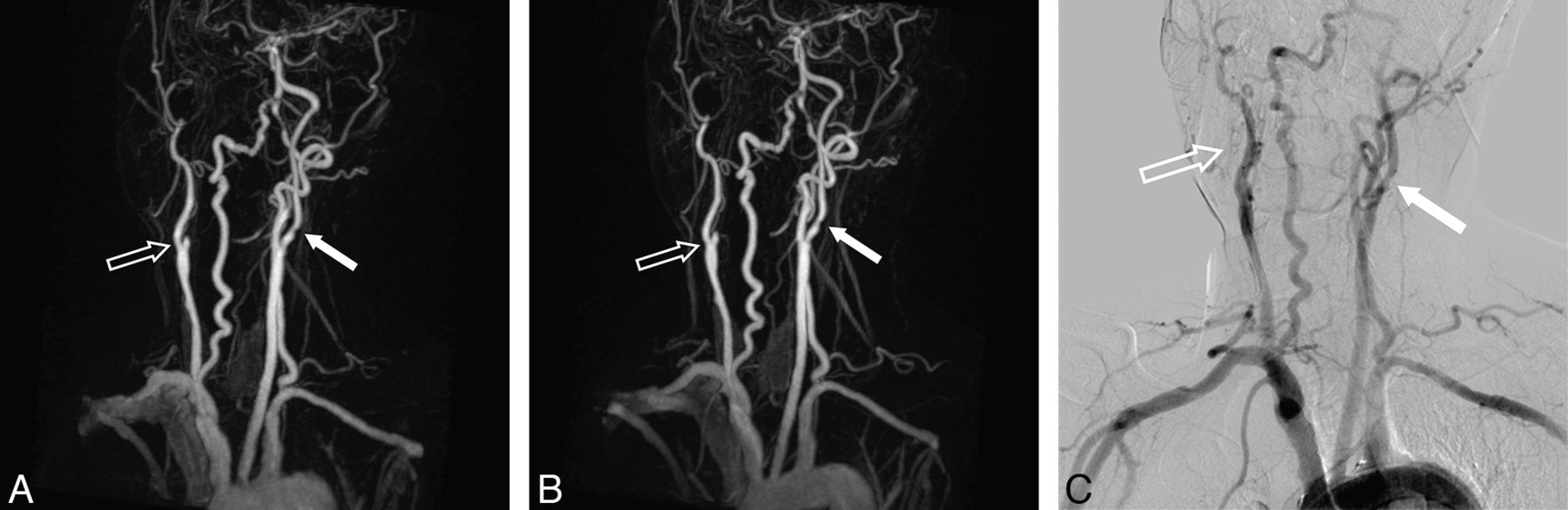
A 62-year-old male patient referred for MR imaging to guide revascularization of symptomatic carotid artery stenosis. The MIP image (A) acquired after 0.1-mmol/kg gadobenate dimeglumine (12 mL injected at 1.2 mL/s) reveals occlusion of the right carotid bifurcation and right ICA (open arrow) and a ≥60% stenosis (closed arrow) of the left carotid bifurcation. Similar findings are seen on the analogous MIP image (B) acquired after 0.2-mmol/kg gadopentetate dimeglumine (24 mL injected at 2.4 mL/s). There is no improvement in image quality or disease/vessel delineation with the higher dose of gadopentetate dimeglumine. DSA (C) confirms the findings of the MRA examinations.
Overall Reader Agreement
Good-to-excellent reader agreement for stenosis detection and grading was noted. Complete (3-reader) agreement was noted in 91.3% of 414 segments (κ = 0.776) assessed by all 3 readers following gadobenate dimeglumine administration and in 91.0% of 413 segments (κ = 0.763) assessed by all 3 readers following gadopentetate dimeglumine administration.
Safety
No adverse events were reported by any patient following administration of either contrast agent. Similarly, there were no marked or meaningful changes in vital sign measurements or laboratory determinations.
Discussion
A previous intraindividual crossover comparison of 0.1-mmol/kg gadobenate dimeglumine and 0.2-mmol/kg gadopentetate dimeglumine for CE-MRA in patients with known or suspected renal artery stenosis revealed no difference in image quality or quantitative contrast enhancement.14 The conclusions were that 0.1-mmol/kg gadobenate dimeglumine is comparable with 0.2-mmol/kg gadopentetate dimeglumine and that the lower dose and injection volume may be clinically advantageous, particularly in patients with compromised renal function. Unfortunately, that study lacked information on diagnostic performance. Our study in patients with symptomatic or asymptomatic disease of the supra-aortic vasculature supports the conclusions of that study,14 not only in showing no meaningful differences in image quality or quantitative contrast enhancement but also in showing no benefit for 0.2-mmol/kg gadopentetate dimeglumine in terms of diagnostic performance. On the contrary, 3 independent blinded readers in our study consistently reported slightly superior diagnostic performance with 0.1-mmol/kg gadobenate dimeglumine (sensitivity: 82.7%–88.5% versus 75.0%–80.8%; specificity: 96.4%–98.6% versus 94.6%–98.6%; accuracy: 94.6%–96.1% versus 92.4%–94.9%), though significant superiority was noted only by reader 2 for accuracy (P = .016) and PPV (P = .008). Although it is well-established that too high a gadolinium dose can obscure certain vessels or increase the risk of artifacts,15 it is unclear whether this was the reason for the consistently slightly inferior performance with 0.2-mmol/kg gadopentetate dimeglumine.
Although our values for sensitivity are slightly lower than values reported elsewhere,1⇓–3 this result may have been due to the relatively low number of true-positive segments on CE-MRA (44, 46, and 43 for gadobenate dimeglumine; 39, 42, and 39 for gadopentetate dimeglumine; readers 1, 2, and 3, respectively) or to the fact that our definition of hemodynamically relevant disease (≥60% lumen narrowing) due to the presence of both symptomatic and asymptomatic patients was slightly wider than the ≥70% definition of the North American Symptomatic Carotid Endarterectomy Trial and the European Carotid Surgery Trial.16,17 Additional factors are that image evaluation in our study was performed in a purely qualitative fashion (no digital calipers) and that evaluation was performed by readers who were unaffiliated with the enrollment centers and entirely unaware of patient eligibility criteria as well as all clinical and radiologic information. Whereas a blinded, independent approach to image evaluation eliminates much of the potential for bias, it imposes a condition that does not exist in clinical routine and that is not always present in studies that do not use a blinded reading methodology. A possible consequence is that the clinical significance of a borderline stenosis maybe be underappreciated; this result could lead to lower overall agreement with DSA. On the other hand, the good-to-excellent 3-reader agreement in our study for both qualitative interpretation and stenosis detection and grading highlights the good reproducibility and high validity and reliability of our approach, despite the limitations imposed by the blinded reading methodology.
In terms of quantitative contrast enhancement, our findings confirm expectations based on relaxivity considerations in showing no difference between 0.1-mmol/kg gadobenate dimeglumine and 0.2-mmol/kg gadopentetate dimeglumine. Most interesting, a tendency toward greater SNR and CNR with 0.1-mmol/kg gadobenate dimeglumine was noted in the neck vessels by all 3 readers. Although none of the differences were significant, Prokop et al14 noted a similar tendency toward greater SNR and CNR with 0.1-mmol/kg gadobenate dimeglumine compared with 0.2-mmol/kg gadopentetate dimeglumine in the abdominal aorta while Pediconi et al8 reported significantly greater CNR with 0.1-mmol/kg gadobenate dimeglumine, albeit in a relatively small population undergoing carotid CE-MRA. A similar significant benefit for 0.1-mmol/kg gadobenate dimeglumine compared with 0.2-mmol/kg gadopentetate dimeglumine in terms of quantitative enhancement has recently been reported in patients undergoing pulmonary CE-MRA,18,19 though the study in question was not a standardized intraindividual comparison but rather an assessment of study data following a protocol switch from 0.2-mmol/kg gadopentetate dimeglumine in response to concerns over the risk of nephrogenic systemic fibrosis with high-dose gadopentetate dimeglumine.
That higher contrast agent relaxivity is of fundamental importance in permitting the use of lower doses in CE-MRA procedures has recently been demonstrated by Achenbach et al,20 who compared gadobenate dimeglumine interindividually with the 1-mol/L agent gadobutrol (Gadovist; Bayer Healthcare) at an equivalent total volume of 0.1-mL/kg bodyweight (corresponding to 0.1-mmol/kg gadobutrol but only 0.05-mmol/kg gadobenate dimeglumine). In their study, 3 blinded, independent investigators found no differences in quantitative enhancement, image quality, or diagnostic accuracy, indicating that the T1 shortening achieved per unit time with 0.05-mmol/kg gadobenate dimeglumine was equivalent to that achieved with 0.1-mmol/kg gadobutrol. Comparative studies in other indications have similarly highlighted the value of high-relaxivity gadobenate dimeglumine in permitting the use of lower doses.21,22 As noted elsewhere,23⇓–25 the higher in vivo R1 relaxivity of gadobenate dimeglumine is due to weak, transient interaction of the gadobenate contrast-effective molecule with serum albumin,26 which slows its molecular tumbling rate, leading to greater shortening of the T1 relaxation time and thus substantially increased signal intensity enhancement.
Taken together, our results confirm that 0.1-mmol/kg gadobenate dimeglumine can fully replace 0.2-mmol/kg gadopentetate dimeglumine for CE-MRA of the supra-aortic vasculature. As pointed out by Prokop et al14 in 2004 before the recognition of nephrogenic systemic fibrosis as a serious life-threatening disease associated with high-dose gadolinium, the possibility of using a lower dose and a lower total volume can be considered an important clinical advantage, particularly in patients with renal insufficiency. In this regard, despite the increased use of gadobenate dimeglumine in CE-MRA procedures following the advent of nephrogenic systemic fibrosis and the decision of regulatory authorities to contraindicate certain gadolinium agents in patients with severe renal impairment, there have been no published cases of nephrogenic systemic fibrosis following the sole administration of this agent.27 Unfortunately, to our knowledge, prospective studies aimed at investigating the effects of lower doses of contrast agents on the incidence of nephrogenic systemic fibrosis are lacking and unfeasible, given the recent changes in the approval status of certain agents. From an imaging perspective, the possibility of using a lower dose and volume without compromising contrast enhancement or diagnostic performance is potentially invaluable if the need is for rapid image acquisition or when assessing narrow, small, or otherwise difficult-to-visualize vasculature.11,28
The blinded intraindividual design of our study renders the results robust, reliable, reproducible, and free of bias. Nevertheless, a possible limitation is that invasive DSA was used as the reference technique. Although DSA has excellent spatial resolution and is invariably the reference standard for determination of diagnostic performance across the gamut of MRA applications, a possible limitation of the technique is that vascular anatomy is depicted in only 2 or 3 projections. For the supra-aortic vasculature in particular, in which stenoses often develop asymmetrically, this may result in underestimation of the narrowest portion of the residual lumen and potentially result in patients not receiving appropriate treatment.29,30 However, this was a potential limitation only for the assessment of diagnostic performance; it would not have influenced the blinded readers' subjective assessment of CE-MRA image quality. A second possible limitation is that examinations were performed at 1.5T only. However, a comparison of gadobenate dimeglumine and gadopentetate dimeglumine for supra-aortic CE-MRA at 3T has already established that gadobenate dimeglumine is likewise effective at higher field strengths.13
Conclusions
Our study confirms that 0.1-mmol/kg gadobenate dimeglumine can fully replace 0.2-mmol/kg gadopentetate dimeglumine for CE-MRA of the supra-aortic vasculature.
Footnotes
Disclosures: Yuan Li—RELATED: consulting fee or honorarium: Bracco, Comments: Bracco Diagnostics Inc provided a fee for blinded image reading.
This study was supported by Bracco Diagnostics Inc.
References
- Received May 18, 2012.
- Accepted after revision July 4, 2012.
- © 2013 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}