
Article Figures & Data
Figures
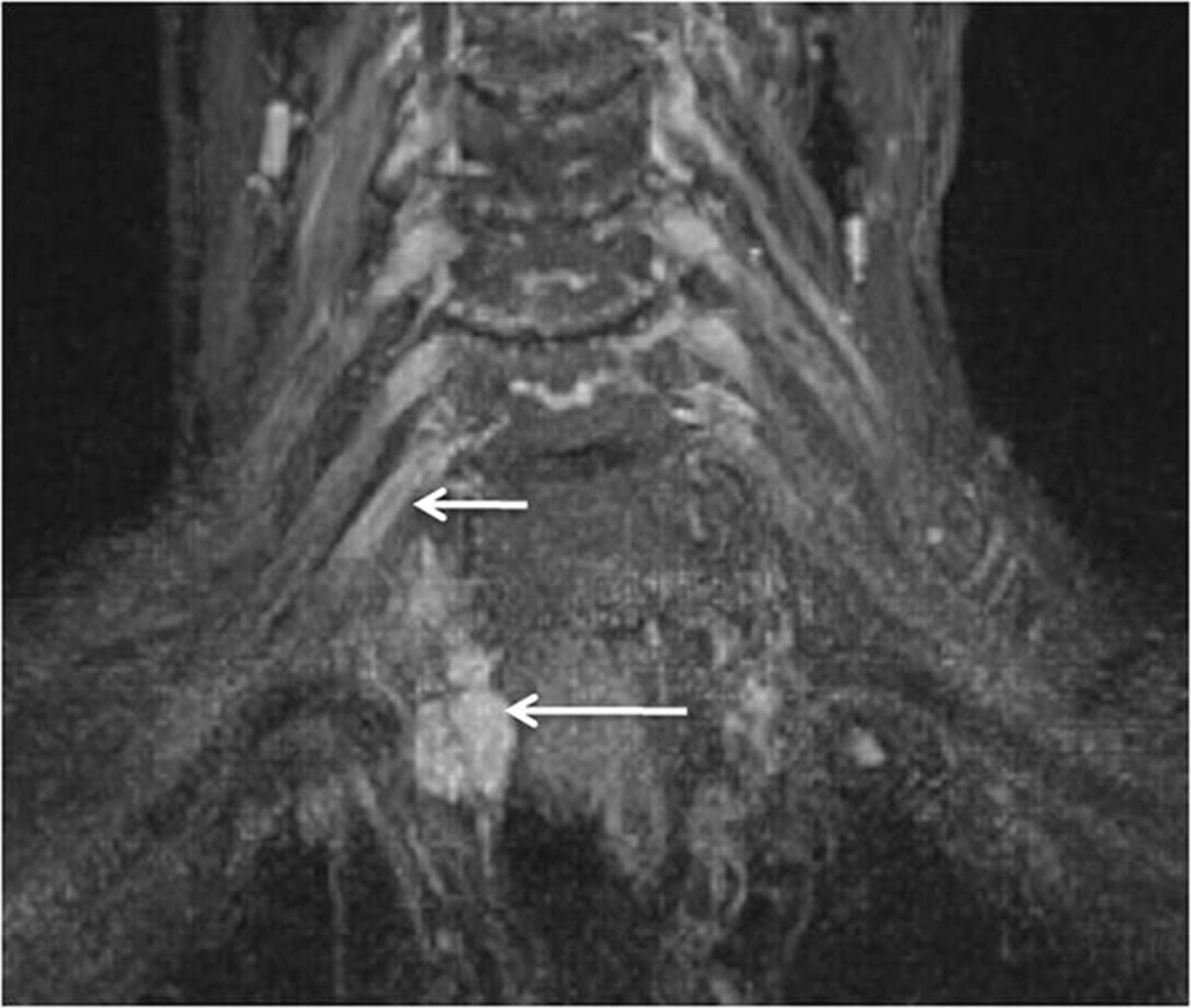
- Fig. 1.
MRN technique. 3T MR neurography imaging sequences with isotropic multiplanar reconstruction. 3D T2 SPACE with multiplanar reconstruction of the cervical spine (medium arrows). Axial T1-weighted image shows the bilateral brachial plexus through the lower aspect of the scalene triangle (small arrows). Coronal MIP 3D STIR SPACE image shows the brachial plexus (thick arrow). Sequential sagittal STIR images show the normal and symmetric C5-T1 nerve roots (curved arrows), trunks (circle), and cords (oval).
- Fig. 2.
Normal brachial plexus. Coronal MIP 3D STIR SPACE image focused on the left side shows the anatomy of the brachial plexus (arrows).
- Fig. 3.
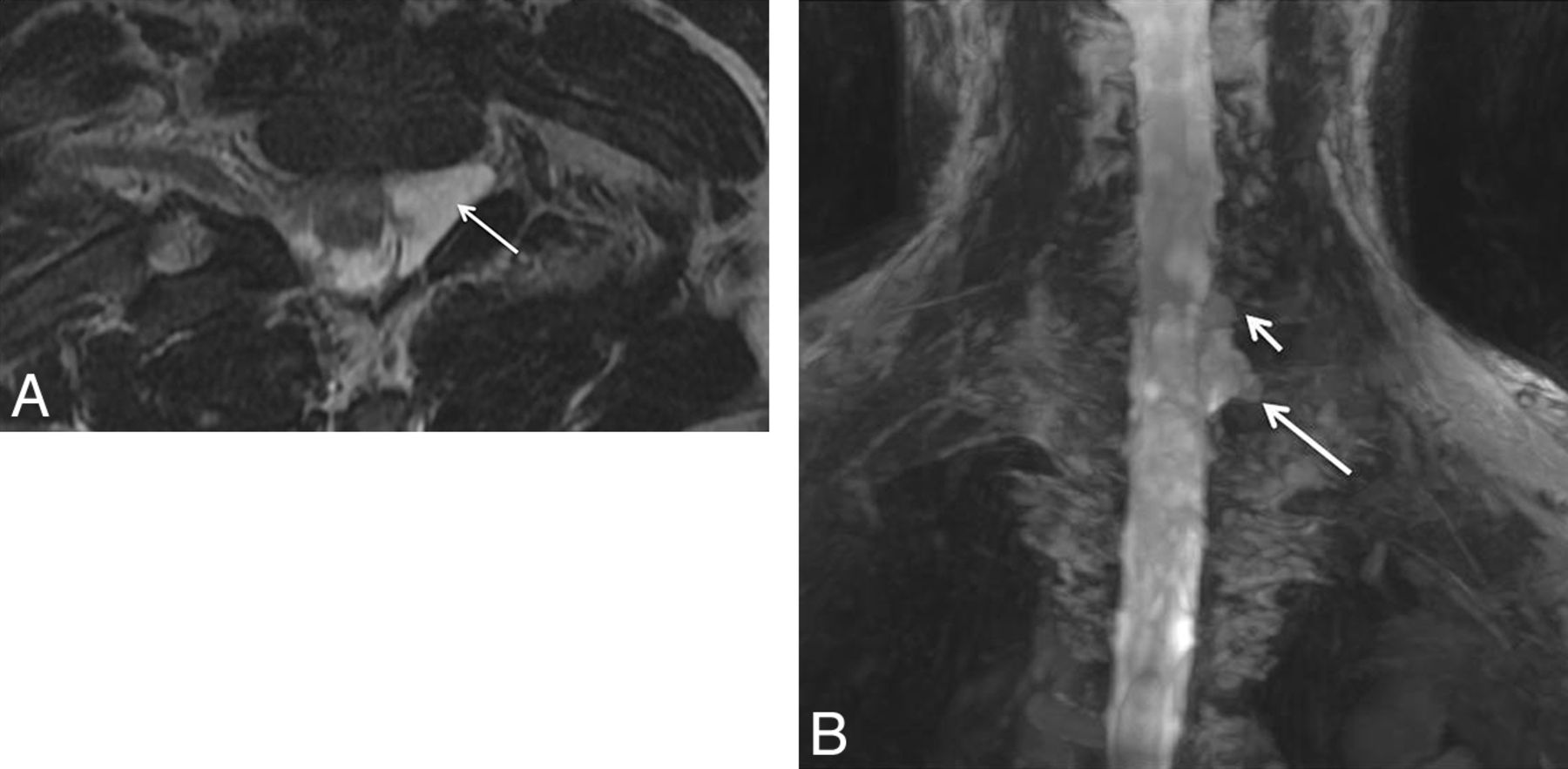
Isolated C6 radiculopathy. A 51-year-old woman with right arm pain and a tingling sensation, clinically suspected of having brachial plexitis versus radiculopathy. Sagittal STIR (A), axial T2 SPACE (B), and coronal 3D MIP STIR SPACE (C) images show an asymmetrically hyperintense and diffusely enlarged isolated C6 nerve root (arrows), corresponding to the markedly narrowed right C6 neural foramen. The findings are in keeping with cervical radiculopathy, in the setting of cervical spondylosis.
- Fig. 4.
Nerve root avulsion. A 22-year-old man after a motor vehicle crash and ulnar-sided arm weakness. Axial T2-weighted (A) and coronal MIP 3D STIR SPACE (B) images show the avulsed left T1 nerve root (large arrows) and C8 nerve root (small arrow) with pseudomeningocele formation.
- Fig. 5.
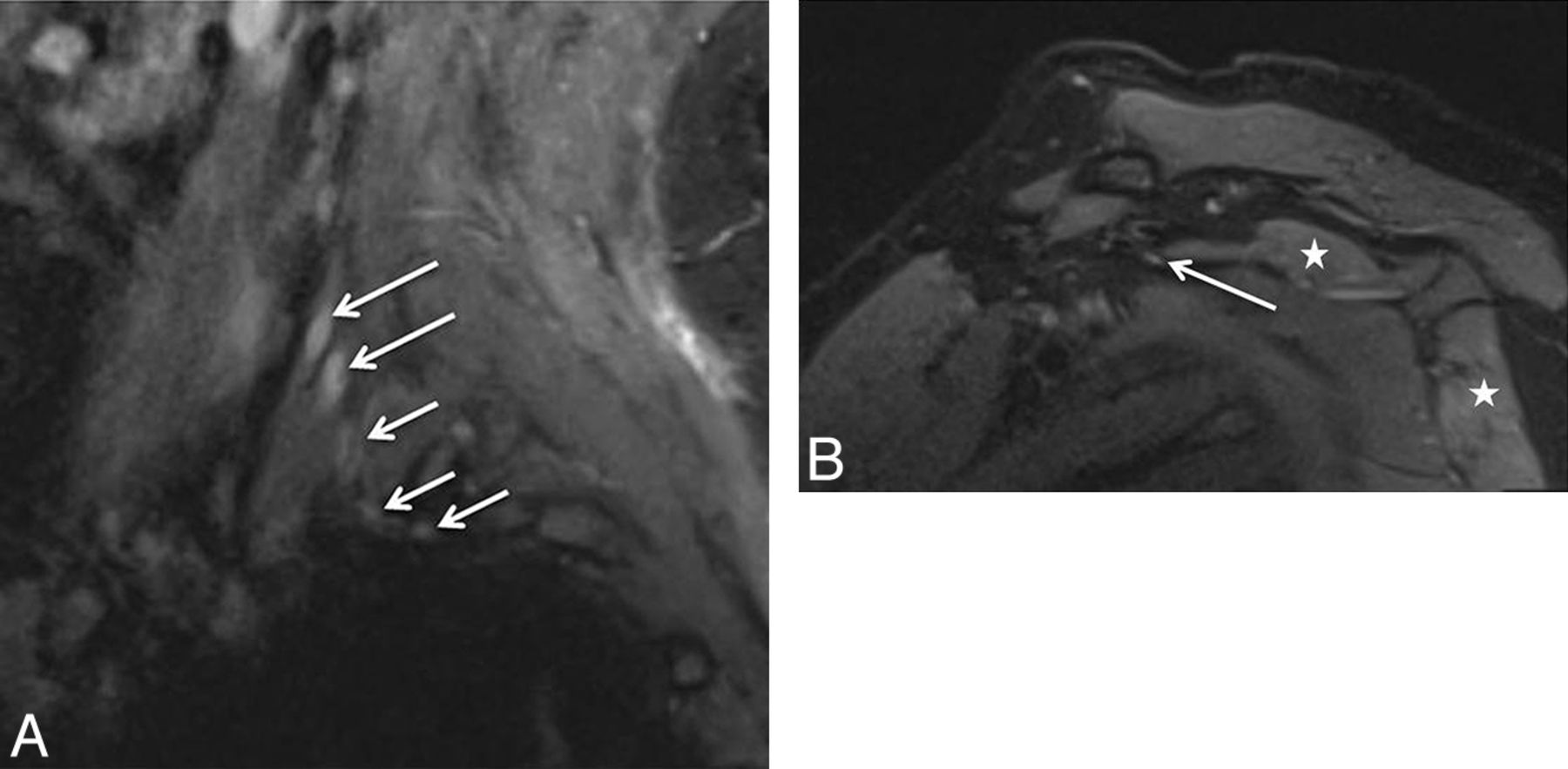
Stretch injury with suprascapular neuropathy. A 48-year-old man after a recent motor vehicle crash. Sequential sagittal STIR images (A and B) show asymmetrically enlarged and hyperintense C5 and C6 nerve roots (large arrows in A) relative to other normal nerve roots (small arrows). All the nerve segments are in continuity. Notice the hyperintense suprascapular nerve (large arrow in B) and mild denervation edema of the supraspinatus and infraspinatus muscles (stars).
- Fig. 6.
Multiple acute nerve root avulsions. A 51-year-old man with loss of function in the left upper extremity due to recent motor vehicle crash. Coronal MIP 3D STIR SPACE (A) and sagittal STIR (B) images show avulsed C6, C7, and C8 nerve roots (arrows) with abnormal morphology due to hemorrhage and edema from a recent injury, obscuring clear details of the nerve roots. Notice the normal C5 nerve root (large arrows in A) and the normal T1 nerve root (small arrow in B).
- Fig. 7.
Neurotmesis. A 43-year-old woman with loss of function in the left upper extremity following recent neck surgery. Coronal MIP 3D STIR SPACE image shows severed, enlarged, and hyperintense C5 and C6 nerve roots with distal end bulb neuromas (arrows), just proximal to the formation of the left upper trunk. The findings were confirmed on re-exploration, and the patient underwent immediate nerve transfer.
- Fig. 8.
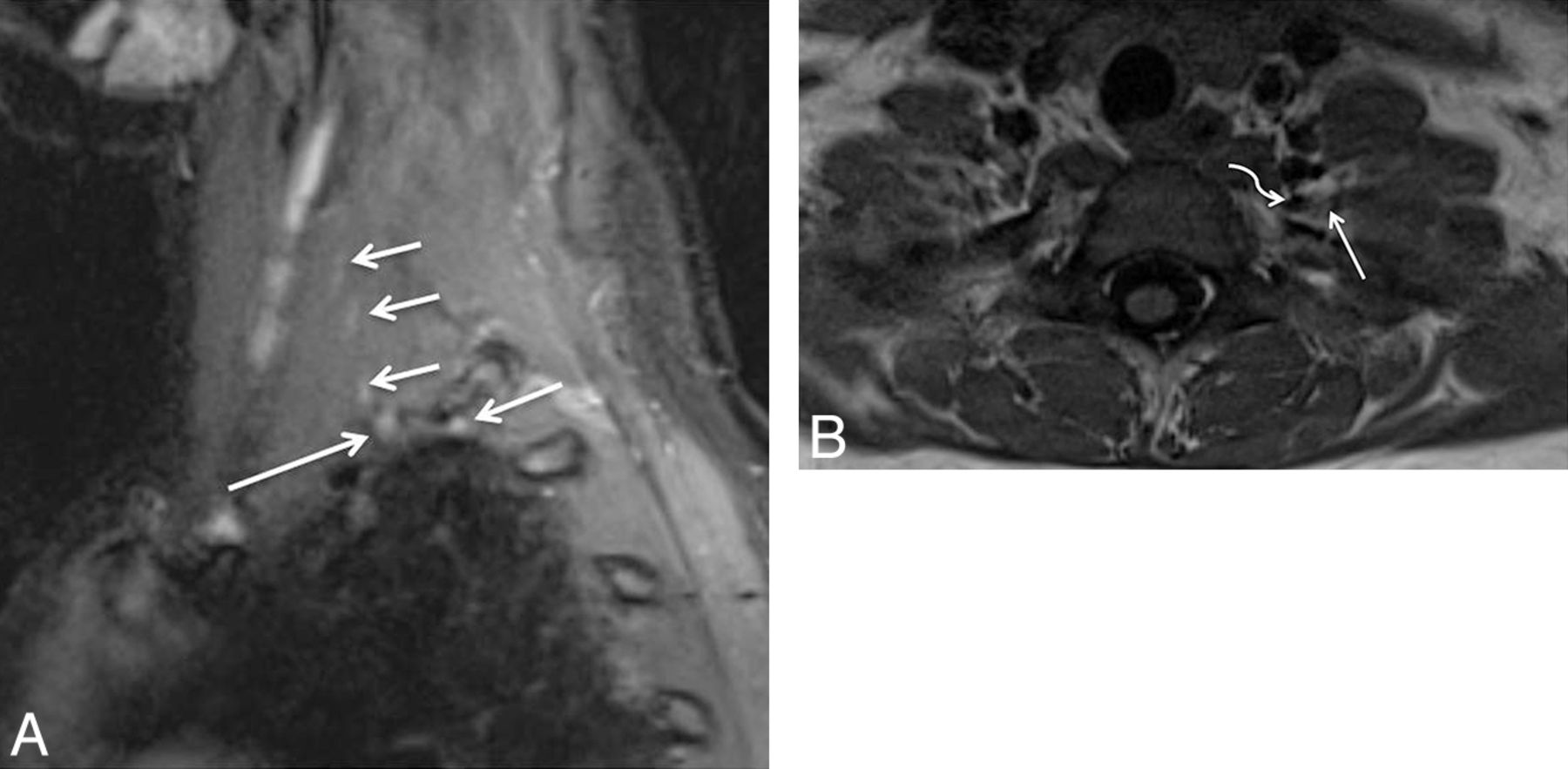
TOS with C8 neuropathy. A 17-year-old girl (trumpet player) with left arm and hand weakness in an ulnar distribution, exacerbated by shoulder abduction. Sagittal STIR (A) image shows an asymmetrically enlarged and hyperintense C8 nerve root (large arrow) compared with the other normal nerve roots (small arrows). Notice minimal asymmetric hyperintensity of the T1 nerve root, a common nonspecific finding. Axial T1-weighted (B) MR image through the lower neck shows a prominent flow void (curved arrow) indenting the left C8 nerve root (large arrow). The EMG findings were normal in this case. On surgery, the flow void turned out to be a prominent branch of the left thyrocervical trunk, which was ligated. C8 neurolysis was also performed. The patient's symptoms completely resolved following surgery.
- Fig. 9.
Thoracic outlet syndrome. A 55-year-old woman with weakness of the left upper extremity with tingling in the hand. Coronal T2 SPACE image shows the deviated path of the C8 nerve root with abnormal flattening (arrow) due to pseudoarthrosis between the left cervical rib and first rib, which was subsequently proved on the surgery. The patient improved after surgery.
- Fig. 10.
Intramuscular course and entrapment of the C5 nerve root. A 48-year-old man after a recent motor vehicle crash. Sagittal STIR (A) and coronal MIP 3D STIR SPACE (B) images show the intramuscular course of the C5 nerve root with relatively anterior and lateral positioning and mild flattening (large arrow) compared with the other brachial plexus nerve roots (small arrows). The patient had no symptoms referable to TOS pathology.
- Fig. 11.
Malignant peripheral nerve sheath tumor. A 56-year-old man with right shoulder and arm pain. Coronal MIP 3D STIR SPACE image shows enlarged right C5 and C6 nerve roots and upper trunk (small arrows) with a surgically proved malignant nerve sheath tumor (large arrow).
- Fig. 12.
Lymphoma involving the terminal branches of the left brachial plexus. A 59-year-old man with left arm pain and weakness. Coronal MIP 3D STIR SPACE image shows mildly hyperintense peripheral nerve branches of the left brachial plexus (small arrows); distally encased by the B-cell lymphoma mass lesion (large arrow).
- Fig. 13.
Neurofibromatosis type 1. Coronal MIP 3D STIR SPACE image in a 24-year-old woman shows numerous cutaneous and subcutaneous hyperintense peripheral nerve sheath tumors along with diffuse nodular thickening of bilateral brachial plexus segments (arrows).
- Fig. 14.
Plexiform neurofibroma in neurofibromatosis type-1 (NF-1). A 36-year-old man with known NF-1 presenting with right shoulder and neck pain with weakness of the arm. Coronal postcontrast fat-suppressed T1-weighted image shows a large infiltrative mass showing a “bag of worms” appearance (large arrows), encasing the brachial plexus (small arrow), in keeping with a plexiform neurofibroma.
- Fig. 15.
Lymphoma. A 65-year-old man with a history of lymphoma who presented with new-onset weakness of the right upper extremity. Coronal MIP 3D STIR SPACE (A) and sagittal STIR (B) images show fusiform enlargement of the right C7 nerve root (arrows) in keeping with lymphomatous involvement.
- Fig. 16.
Radiation plexopathy. A 67-year-old woman with a history of left breast carcinoma and radiation treatment 20 years ago who presented with weakness and pain in the left upper extremity. Coronal MIP 3D STIR SPACE (A) image shows diffusely enlarged and abnormally hyperintense left C8 and T1 nerve roots and lower trunk (arrows). Corresponding coronal fat-suppressed postcontrast T1-weighted (B) image shows no focal enhancement (arrows) to suggest recurrent disease. Axial non-fat-suppressed T1-weighted (C) image shows perineural radiation fibrosis encasing the left C8/T1 nerve roots and the lower trunk of the brachial plexus (arrows).
- Fig. 17.
Radiation neuropathy. An 81-year-old woman, previously treated for right breast carcinoma, who presented with right arm and neck pain. Coronal 3D STIR SPACE image shows a focal mass (large arrow) encasing the right T1 nerve root. Additionally, there are mild enlargement and hyperintensity of the right C8 nerve root (small arrow).
- Fig. 18.
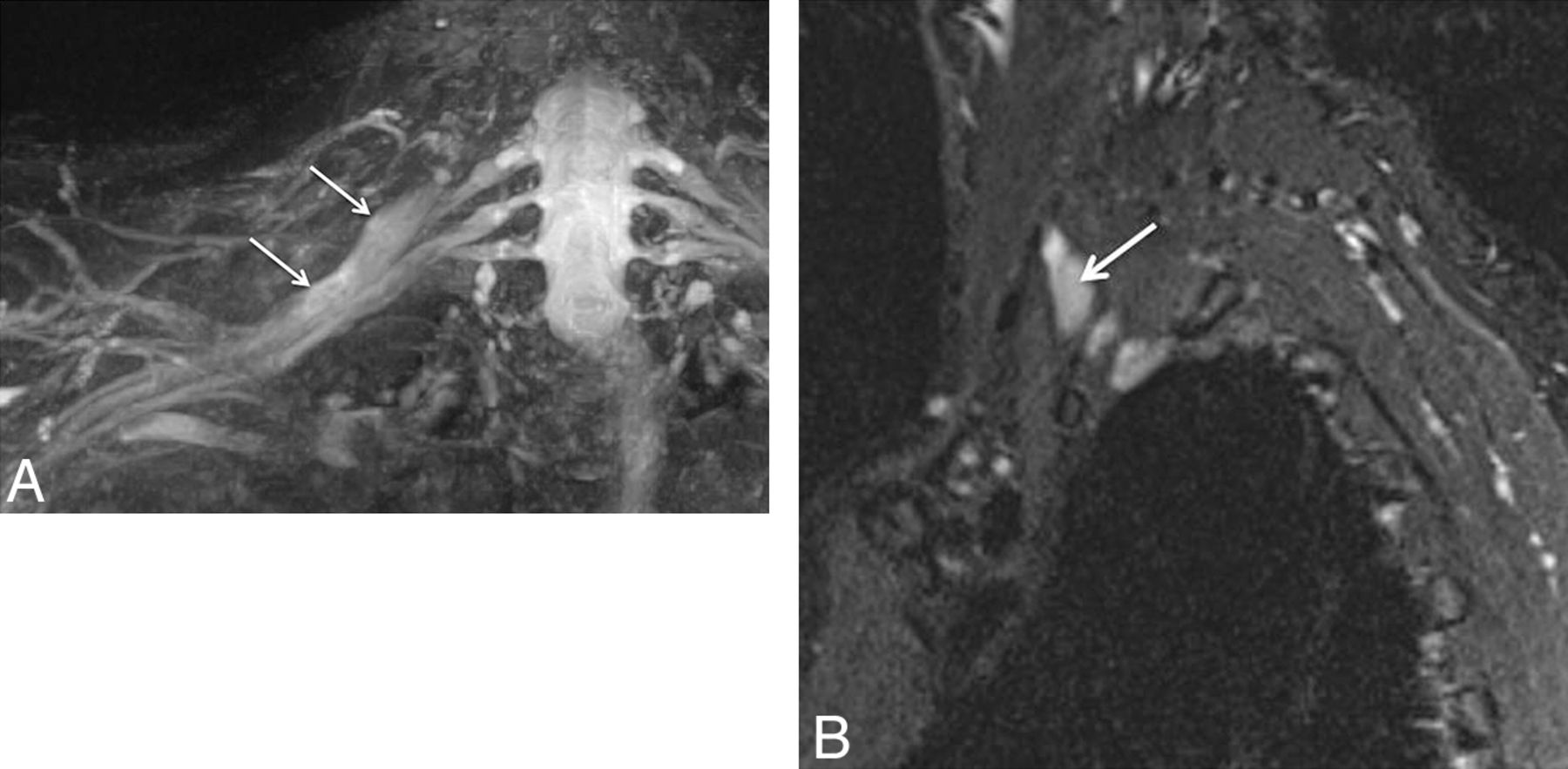
A, Brachial neuritis with long thoracic nerve neuritis. A 54-year-old man with right shoulder pain and right scapular winging for a few months. Coronal 3D STIR SPACE image shows the asymmetrically hyperintense and enlarged C7 nerve (large arrows). The abnormality extended into the middle trunk and its divisions (not shown). Notice normal left C7 nerve root (small arrows). Sagittal STIR (B) image shows the abnormally enlarged and hyperintense long thoracic nerve along its course (arrow). Axial STIR (C) image through the chest shows atrophy and edema like signal of the right serratus anterior muscle (small arrows). Notice the normal left serratus anterior muscle (large arrow).
- Fig. 19.
Brachial and axillary neuritis. A 43-year-old woman with right shoulder pain. Sagittal fat-suppressed T2-weighted image shows an abnormally hyperintense axillary nerve (small arrows) and denervation edema in the teres minor muscle (large arrow).
- Fig. 20.
Neurotmesis with suprascapular nerve severance and axillary neuropathy. A 46-year-old man with a dirt bike injury. Coronal MIP 3D STIR SPACE (A) image shows complete disruption of the left C5 and C6 nerve roots (arrows), proximal to the formation of the upper trunk. Sagittal STIR (B) image shows an enlarged and hyperintense suprascapular nerve proximal to its disruption (large arrow). Also note hyperintense trunks of the brachial plexus (small arrows). Further lateral sagittal STIR (C) image shows denervation changes in the rotator cuff (small arrows) muscles (C5 and C6 distribution) and an abnormally hyperintense but continuous axillary nerve (large arrows).
- Fig. 21.
A, Stretch Injury to right sided brachial plexus. Coronal 3D STIR SPACE (A) image shows diffusely enlarged right sided brachial plexus (large arrows) following a recent clavicular fixation for fracture. Notice normal left brachial plexus (small arrows). The patient improved over a few months of expectant treatment. B and C, Stretch injury of the C6 nerve root and musculocutaneous nerve. A 60-year-old man with weakness of the right biceps and brachialis muscles following a recent injury. Axial T2 SPAIR (B) image through the proximal right arm shows an abnormally hyperintense and enlarged musculocutaneous nerve (large arrow) with denervation changes in the biceps and brachialis muscles (small arrows).





















Tables
3T MRN examination protocol for the evaluation of the brachial plexus (FOVs from C2 to T2)
FOV Section Thickness TR/TE/TF (ms) Matrix MR imaging sequence T1 coronal (T1 axial) 30 4.0 881/11/7 512 × 512 3D coronal STIR SPACE 30 1.0 1500/97/53 256 × 256 3D sagittal T2 SPACE 25 1.0 1000/97/81 256 × 256 STIR sagittal, bilateral, affected side 22–24 3.0 5210/18/22 256 × 256 Additional arm examination if desired Axial T1 20–22 3.0–4.0 550/7.9/6 256 × 384 Axial T2 SPAIR 20–22 3.0–4.0 2840/70/13 256 × 384 Note:—TF indicates turbo factor; SPAIR, spectral-attenuated inversion recovery.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- ABBREVIATIONS:
- Anatomic Considerations
- Pathologic Conditions
- MRN Indications
- Abnormal MRN Findings in the Brachial Plexus
- Brachial Plexus Injuries
- Interpretation Pitfalls
- Thoracic Outlet Syndrome
- Tumor and Tumor Variants
- Radiation Neuropathy
- Brachial Plexitis (Neuralgic Amyotrophy or Parsonage Turner Syndrome)
- Peripheral Branch Nerves of Brachial Plexus
- Conclusions
- Footnotes
- References
- Figures & Data
- Info & Metrics
- Responses
- References
Related Articles
Cited By...
- Role of MR Neurography for the Diagnosis of Peripheral Trigeminal Nerve Injuries in Patients with Prior Molar Tooth Extraction
- MR Imaging of the Superior Cervical Ganglion and Inferior Ganglion of the Vagus Nerve: Structures That Can Mimic Pathologic Retropharyngeal Lymph Nodes
- High-Resolution MRI Evaluation of Neonatal Brachial Plexus Palsy: A Promising Alternative to Traditional CT Myelography