
Abstract
SUMMARY: For effective transvenous embolization of DAVFs, it is important to place coils at the shunting venous pouch in the initial step of the procedure. When it was difficult to navigate a microcatheter to the shunting venous pouch due to the anatomic relationship of approach routes with targeted pouches, we navigated the microcatheters by a “turn-back technique” within the involved sinuses into the target pouches. Complete occlusion or regression of the DAVF was obtained in all cases.
ABBREVIATIONS:
- AP
- anteroposterior
- CS
- cavernous sinus
- DAVF
- dural arteriovenous fistula
- TSS
- transverse-sigmoid sinus
The treatment strategy used for transvenous embolization of a DAVF is particularly dependent on the drainage route and the shunt surgery point of the dural fistula.1⇓–3 For safe and effective treatment, the shunting point itself should be predominantly occluded by placing coils. However, in some cases, navigation of the microcatheter to the shunting point is difficult with a standard guidewire technique due to the anatomic relationships between the shunting point and the accessible route. In such cases, we attempted the “turn-back embolization technique,” in which a microcatheter is turned back in the affected sinus and is introduced into the shunted segment.
Description of Technique
Patients
Using the turn-back embolization technique, we treated 8 patients with DAVFs, including 5 TSS-DAVFs and 3 CS-DAVFs. All TSS-DAVFs showed ipsilateral sigmoid sinus occlusion, and 1 of the cases showed an “isolated sinus.” All except 1 patient demonstrated occipital cortical venous reflux. The Cognard classification was IIa in 1, IIa+b in 2, and III in 1 of the TSS-DAVFs.4
One patient with a CS-DAVF showed ipsilateral inferior petrosal sinus occlusion. All of CS-DAVFs were associated with superficial cortical venous system drainage or deep venous system drainage. All CS-DAVFs were classified as grade IIa+b.
Treatment Methods
We carefully determined the dataset of the diagnostic digital subtraction angiography and multiplanar reconstructed images from the rotational angiography, with particular focus on the location of the DAVF, the shunting point on the affected dural sinus, the patency of the dural sinus, and cortical venous reflux.
A 5F guiding sheath/catheter coaxial guiding system was advanced into the jugular vein, and then the microcatheter (Excelsior straight or 45° shape, Boston Scientific Japan, Tokyo) was advanced into the affected sinus by using a microguidewire (Radifocus Glidewire GT; Terumo, Tokyo, Japan). When the antegrade access into the shunting points was difficult, we attempted the turn-back method to navigate the microcatheter to the shunted pouch. This method entails navigating the microcatheter into the affected sinus, after which the microguidewire is turned back within the sinus via deflection off the contralateral sinus walls. The microcatheter could then be turned back within the sinus over the microguidewire and positioned into the shunting point. This process is shown in Fig 1. In the event that there is no point that could be used for the deflection of the microguidewire, 2 or 3 detachable microcoils not occluding the main drainage route are deployed without stemming drainage flow (Fig 2). These microcoils then serve as the deflection point from which the microguidewire and microcatheter are turned back.

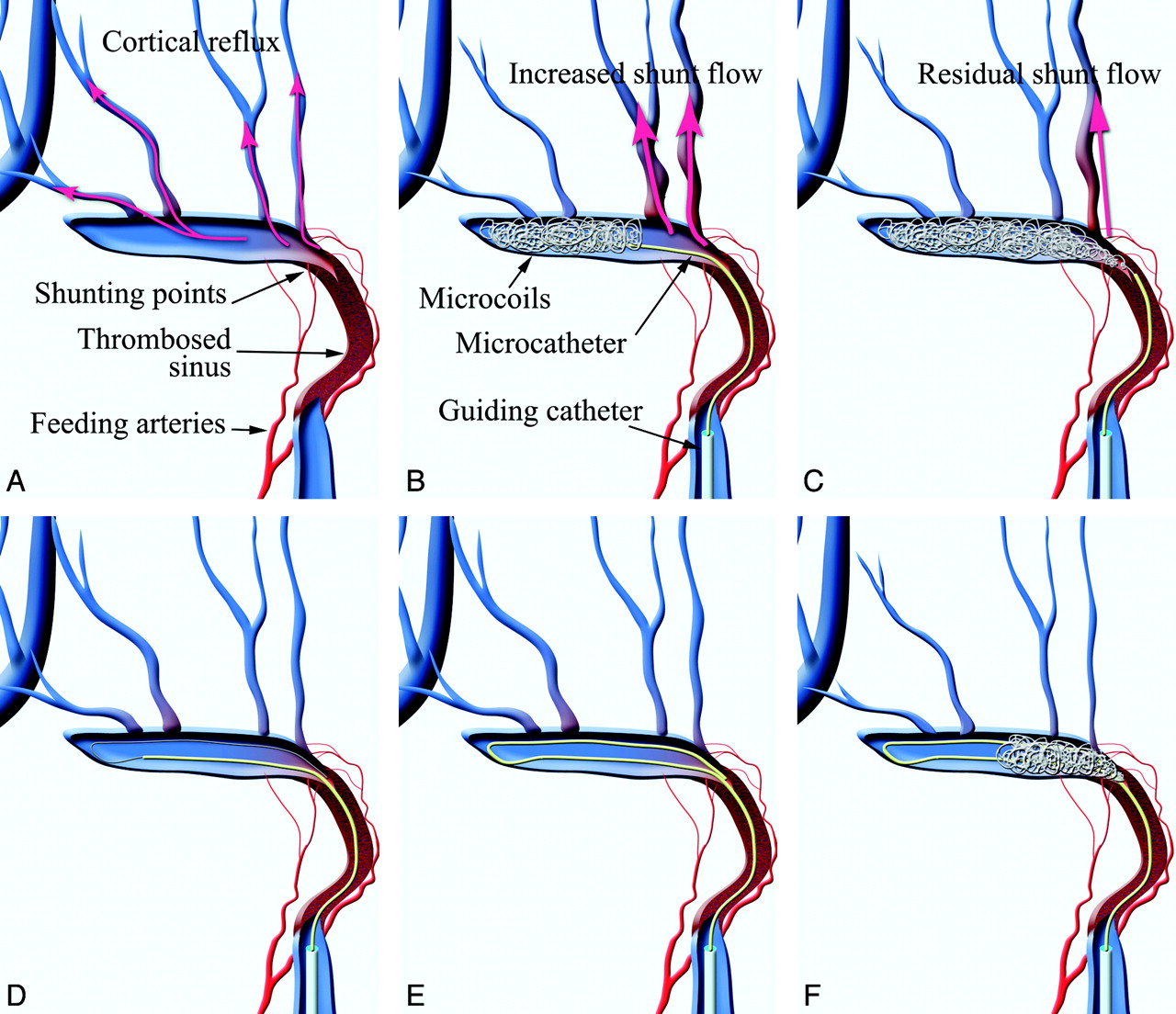
Schematic drawings of the risk of increasing and/or residual cortical reflux while placing coils from the distal-to-proximal segment and the turn-back embolization technique for DAVFs. A, In a TSS-DAVF with sinus occlusion like the Cognard type IIa+b or III, shunt surgery points and dangerous cortical reflux, such as the vein of Labbe and temporal veins, tend to be located at the proximal part of the transverse sinus, which is close to the occluded sinus. B and C, For such cases, standard transvenous embolization through the thrombosed sinus from the distal normal segment to the proximal abnormal segment has a risk of increased cortical venous reflux while packing from the distal to proximal part (B) or a risk of residual reflux due to insufficient packing of the shunt surgery point (C). D, In such cases, a transfemoral transvenous approach through the occluded ipsilateral sigmoid sinus can be performed. After antegrade navigation of a microcatheter into the sinus, a microguidewire is deflected at the distal end of the occluded sinus. E, Then the microcatheter is advanced to the shunt surgery point over the microguidewire. F, Microcoils can be placed into the shunt surgery point at the initial stage of sinus packing. This technique can minimize the risk of insufficient occlusion of the shunt flow when placing coils from an abnormal-to-normal segment rather than from a normal-to-abnormal segment.

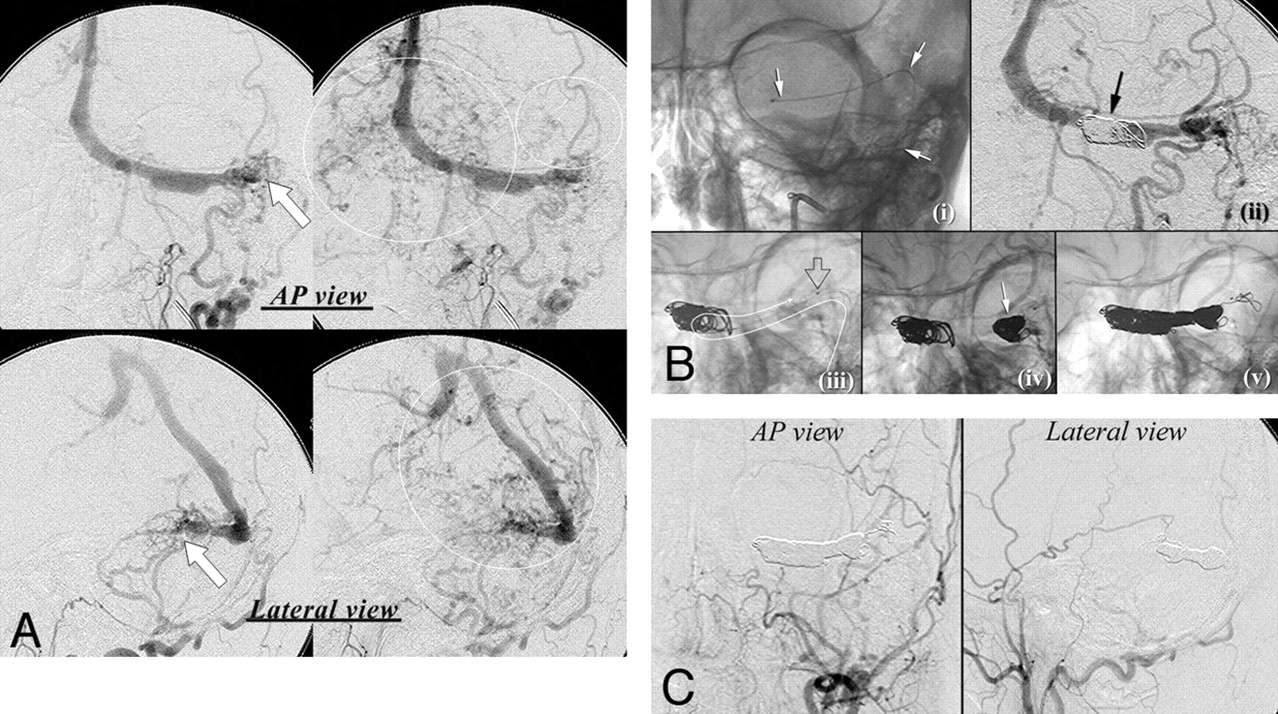
A 52-year-old man with hemianopsia and ataxia. A, The DAVF is fed mainly by the left occipital artery and drains into the straight sinus (arrows) on diagnostic angiography (upper images, frontal view; lower images, lateral view). The left transverse sinus does not communicate with the right transverse sinus. Marked cortical venous reflux into the vein of Labbe and the deep venous system is also seen (circle). B, Turn-back embolization method. i, AP view of the fluorogram. A microcatheter is navigated through the occluded ipsilateral TSS (arrow). ii, AP view of angiography. Because there is no toehold to turn the catheter, some coils not occluding the main drainage route are placed without stemming drainage flow (arrow). iii, AP view of the fluorogram. The microcatheter is turned back to the shunt surgery point at the proximal part of the TSS. The white curved arrow indicates the course of the microcatheter. The open arrow shows the tip of the microcatheter. iv, AP view of the fluorogram. The shunt surgery point is densely packed at the initial step of sinus packing (arrow). v, Fluorogram immediately after packing of the involved TSS. The TSS was packed with a drawing microcatheter after coiling of the shunt surgery point. C, Digital subtraction angiography immediately after embolization shows complete obliteration of the DAVF.
Therapeutic Results
The microcatheters were advanced via the contralateral TSS in 2 patients with TSS-DAVFs and via the thrombosed ipsilateral SS in 3 patients with TSS-DAVFs. All CS-DAVFs could be accessed via the ipsilateral inferior petrosal sinuses. The microcatheters were turned back with the toehold of the contralateral side of the sinus wall in 6 patients or with predeployed coils in 2 patients (Fig 2).
All patients with CS-DAVFs except for 1 were treated by packing of the affected sinus with detachable microcoils. One CS-DAVF was treated by targeted embolization of the shunting venous pouch alone (Fig 3). Transarterial angiography immediately after the procedures showed complete obliteration of shunt flow in 4 patients and nearly complete obliteration in 4. No procedure-related complication was observed in any patient.

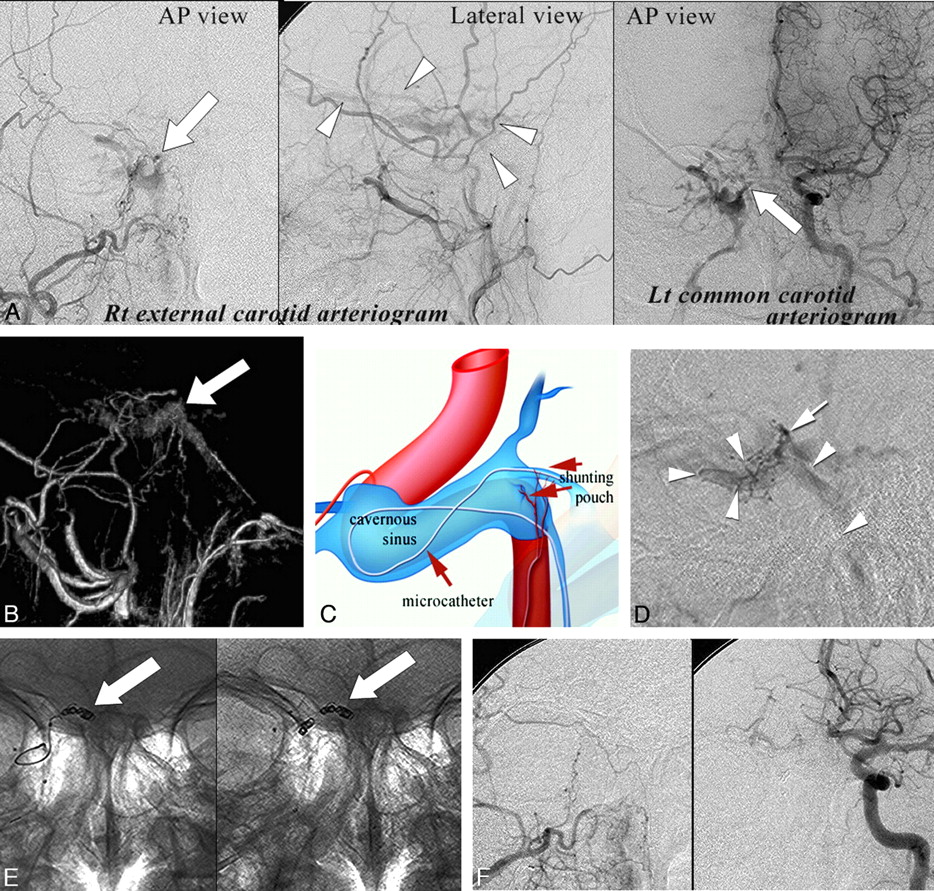
A 55-year-old man with double vision. A, Right external carotid angiography and left common carotid angiography show the CS-DAVF (arrow) fed by the ascending pharyngeal artery and the artery of the foramen rotundum. Arrowheads indicate drainage veins. B, The shunt surgery venous pouch can be identified on surface rendering of rotational digital subtraction angiography at the posteromedial wall of the right cavernous sinus. C, Schematic drawing of navigation of the microcatheter into the shunt surgery venous pouch. Because the shunt surgery venous pouch is acutely angulated from the accessible ipsilateral inferior petrosal sinus, a microcatheter is navigated into the pouch by the turn-back technique as shown in the schematic drawing. D, Lateral view of the selective shunt surgery pouch venography. Arrowheads indicate the course of the microcatheter; the arrow indicates the tip of the microcatheter. E, AP view of the fluorogram. After navigation of the microcatheter, detachable microcoils are selectively placed in the shunt surgery venous pouch without sinus packing (arrows). F, Anterior views of the right external and left common carotid arteriogram immediately after the procedure show complete obliteration of the DVAF.
Discussion
For the transvenous embolization of a DAVF, it is important to obliterate the shunting point. However, some cases exist where the shunting point is located at an anatomically difficult site for antegrade navigation of microcatheters. In TSS-DAVFs with ipsilateral sinus occlusion like Cognard type IIa+b or III, transvenous embolization through the thrombosed sinus has been reported as a safe and effective technique.5⇓–7 However, in such cases, the shunting point and dangerous cortical reflux (eg, the vein of Labbe and temporal veins) tend to be located at the proximal part of the transverse sinus, which is close to the occluded sinus. Antegrade sinus packing has a risk of increased cortical venous reflux while placing the coils from the distal normal segment to the proximal abnormal segment or a risk of residual reflux due to incomplete packing of the shunting point (Fig 1). To prevent increased cortical reflux while sinus packing, we attempted the turn-back embolization technique for some patients. This technique allowed us to place the microcoils preferentially into the shunting point at an early stage of the procedure and to minimize the risk of insufficient occlusion of the shunt flow when placing coils from an abnormal to a normal segment rather than from a normal to an abnormal segment. In addition, it allowed us to easily perform selective packing in cases with a parasinus shunting point, which is sharply angulated from the accessible route.
All patients with TSS-DAVFs showed ipsilateral sigmoid sinus occlusion. Three of these TSS-DAVFs were approached through the thrombosed sinus because 1 case was an isolated sinus and 2 cases had no communication with the contralateral TSS. Moreover, the shunting points were located predominantly at the proximal end of the affected sinus. Thus, the packing of proximal parts by using the turn-back technique was considered an effective method that avoided increasing the pressure in the cortical veins during embolization. The remaining 2 TSS-DAVFs were approached through the contralateral TSS. However, they exhibited a parasinus shunting venous pouch, in which an antegrade approach into the venous pouch was difficult. Recent investigators reported the usefulness of targeted embolization of DAVFs while preserving the patency of dural sinuses.2,8⇓–10 By using the turn-back technique, we could advance the microcatheters into the venous pouch and could selectively obliterate the shunting point in our patients.
All CS-DAVFs were approached via the ipsilateral inferior petrosal sinus. Because both patients had a shunting point at the posterior wall of the CS, the turn-back method was effective to obliterate the shunting point at the initial stage of sinus packing. One CS-DAVF was completely occluded by using only targeted embolization, owing to the good holding effect of the microcatheter by this technique.
For the deflection of the microcatheter, it must adhere once to the opposite side of the sinus wall, and the wall then can act as a toehold for turning it back and placing coils. In 2 patients in our series, we used the predeployed coils as toeholds. These 2 patients had no toeholds to turn the catheter near the shunting point. In this situation, it was useful to place some coils initially to make the wall for the deflection of the microcatheters and for holding the catheters while placing the coils.
References
- Received July 7, 2010.
- Accepted after revision November 8, 2010.
- © 2012 by American Journal of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.