
Abstract
SUMMARY: We present a patient with an acute cervical spinal cord infarction resulting from the use of sildenafil (Viagra) in combination with his hypertension medication. Symptoms were acute and rapidly progressive, and MR imaging with DWI was crucial in confirming the diagnosis.
ABBREVIATIONS:
- DWI
- diffusion-weighted imaging
- STIR
- short tau inversion recovery
Cervical spinal cord infarction is rare due to the rich anastomotic networks between the vertebral and the posterior inferior cerebellar arteries in the upper cervical cord and the thyrocervical and costocervical branches of the subclavian arteries in the lower cervical cord.1 Spinal cord infarction is caused by various etiologies, including atherosclerosis, vertebral artery occlusion or dissection, trauma, fibrocartilaginous embolism, cervical cord herniation, and surgery.2 Aortic dissection and aortic aneurysm repair, arteriovenous malformation, cryptogenic transient ischemic attack, and cardiac arrest are also relatively frequent causes of cord infarction as well.3 We report a patient with a cervical spinal cord infarction after the concomitant administration of sildenafil citrate (Viagra) and hydrochlorothiazide.
Case Report
A 59-year-old man with a medical history significant for hypertension and hyperlipidemia presented to a local hospital due to weakness in his arms and an inability to move his legs. Three hours earlier, the patient had taken 50 mg of sildenafil along with hydrochlorothiazide (a component of his antihypertensive regimen) at the same time. Approximately 10 minutes later, while in the shower, the patient noticed right-shoulder weakness that rapidly spread to his left body. Soon after, he could no longer hold the soap in his hand. During the following hour, he could not move his legs, he began to feel dizzy, and his vision became blurry. The patient's wife called the paramedics when his symptoms did not improve. On arrival at a local hospital, he was found to have low systolic blood pressure of 80 mm Hg. A cervical/thoracic spine MR imaging performed approximately 7 hours after the onset of symptoms demonstrated high T2 signal intensity in the anterior spinal cord from C4 to C6.
The patient was transferred to our hospital. Repeat MR imaging of the cervical and thoracic spine with DWI, which was performed approximately 33 hours after symptom onset, again showed abnormal increased T2 and STIR signal intensity in the anterior spinal cord beginning at C4 and extending to T1. There was corresponding restricted diffusion in this region, and the findings were thought to be consistent with acute cord infarction (Fig 1). Additional studies included a CT angiography that showed no aortic dissection and normal cardiac telemetry. It was concluded that the spinal cord infarction was induced by hypotension due to coadministration of sildenafil and hydrochlorothiazide. Although the patient had taken sildenafil previously, he had not ever taken it with his antihypertensive medication. Two months after presentation and physical therapy, the patient was paraplegic and had recovered sensation and some strength in his upper extremities. Three months after presentation, the patient still had not regained lower extremity function, and required a motorized wheelchair.

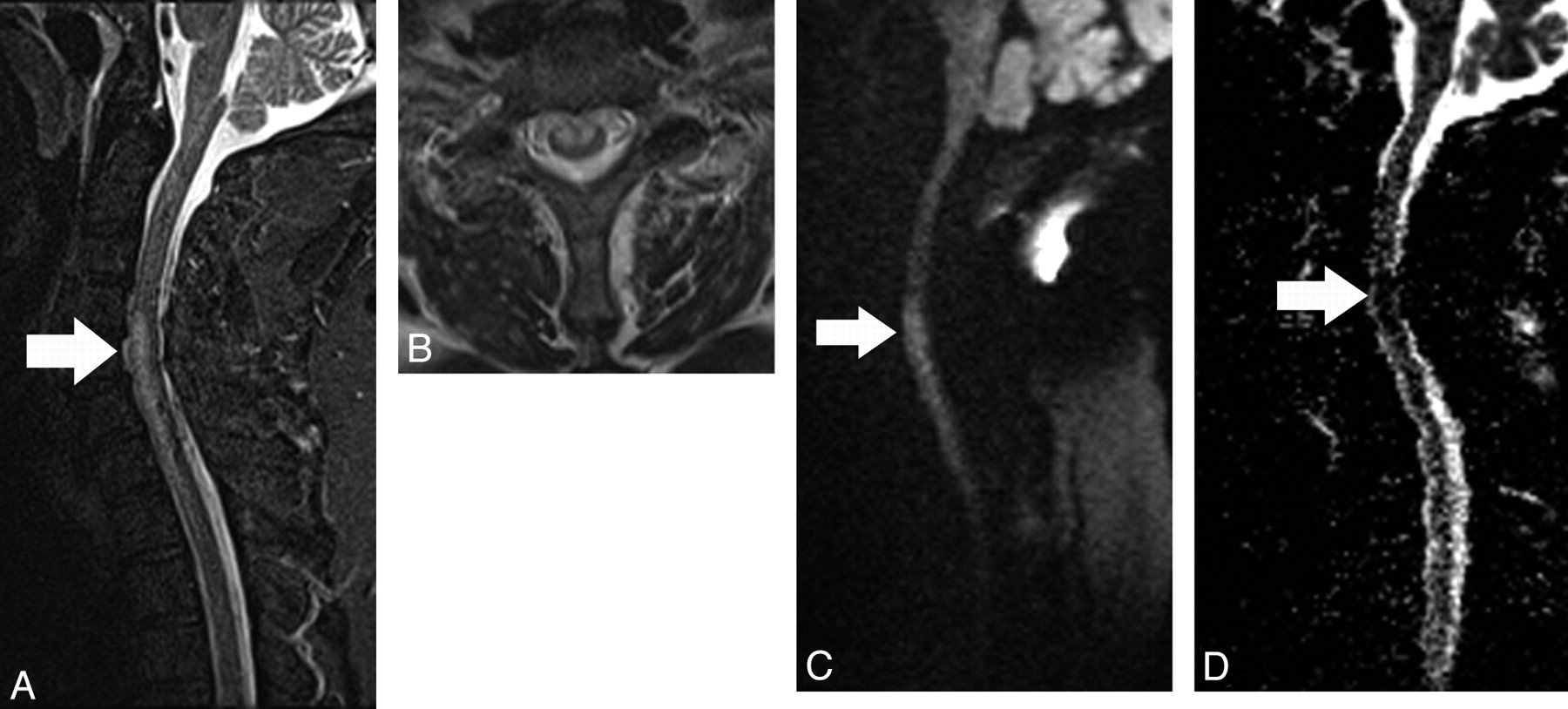
A, Midsagittal T2 STIR image shows high signal intensity (arrow) in the midcervical spinal cord predominantly in its anterior aspect. B, Axial T2-weighted image demonstrates that the high signal intensity abnormality predominantly involves the anterior gray matter horns. C, Midsagittal DWI shows high signal intensity (arrow) in the cord corresponding to the abnormality shown in A. D, Corresponding apparent diffusion coefficient map shows low signal intensity (restricted diffusion, arrow) in the same location.
Discussion
Infarction of the cervical spinal cord is exceptionally rare due to its rich anastomotic arterial network.4 In the upper cervical spine, blood cord supply is from the vertebral arteries and the posterior inferior cerebellar arteries. Below the upper cervical levels, the anterior and posterior spinal arteries become narrow in caliber and form an anastomotic network with radicular arteries. These radicular arteries arise from the subclavian artery via the ascending cervical branch of the thyrocervical trunk or via the deep cervical branch of the costocervical trunk.1 This anastomotic network contributes to the vascularization of the lower cervical and upper thoracic cords.1 The blood supply of the anterior spinal artery is at its most marginal in the upper thoracic region, T2-T4; thus, this watershed zone is vulnerable to hypotension.1,6 Additionally, the pattern of cervical radicular arteries suggests a minor watershed zone at C4.1 The pattern of our patient's spinal cord infarct corresponded to these watershed zones, with his cord infarct spanning C4-T1.
After other etiologies were excluded as the source of our patient's cord infarct, we concluded that the cause was the combined simultaneous use of sildenafil citrate and hydrochlorothiazide. This drug combination likely led to systemic hypotension, resulting in cord infarction in the watershed zones of the cervical and upper thoracic cord. Reported cardiovascular side effects of sildenafil citrate are usually minor and associated with vasodilation, leading to small decreases in systolic and diastolic blood pressures.7 Sildenafil typically produces a transient 8- to 10-mm Hg reduction in systolic blood pressure and a 5- to 6-mm Hg reduction in diastolic blood pressure. This transient reduction in blood pressure generally returns to baseline 4 hours later. Sildenafil may be hazardous to patients on multidrug antihypertensive drug regimens. Although the significant risk of potentially life-threatening hypotension with coadministration of nitrates and sildenafil is well-known, to our knowledge, no formal drug-drug interaction studies have been conducted with sildenafil and hydrochlorothiazide. The effects of sildenafil may be augmented by hypotension caused by nitrates, drugs that inhibit its metabolism, and comorbidities that increase its levels such as kidney/liver diseases.8 Transient ischemic attacks, transient global amnesia, and ischemic optic neuritis have been reported to occur after sildenafil use.9⇓⇓–12 The addition of other drugs, such as hypoglycemic agents, to sildenafil may result in diffuse cerebral anoxia.13 Intracerebral and subarachnoid hemorrhages and seizures have been reported with sildenafil.8
In conclusion, the possibility that rarely sildenafil, particularly in combination with other drugs, may cause significant neurologic abnormalities, including spinal cord infarction, must be kept in mind.
References
- Received December 1, 2010.
- Accepted after revision January 15, 2011.
- © 2012 by American Journal of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.