
Abstract
SUMMARY: PLS is a disease of the UMN, distinguished from ALS in prognosis and absence of LMN signs. We present, to our knowledge, the first conventional MR imaging visualization of the callosal motor segment, a concept previously supported by primate models, electrophysiologic studies, and postmortem examinations. Modification of the Witelson topographic scheme of the CC is supported by MR tractography. On the basis of 2 cases of PLS, we present conventional imaging confirmation of the revised topographic scheme of fiber distribution across the CC.
Abbreviations
- ALS
- amyotrophic lateral sclerosis
- CC
- corpus callosum
- CST
- corticospinal tract
- DTI
- diffusion tensor imaging
- FA
- fractional anisotropy
- FLAIR
- fluid-attenuated inversion recovery
- LMN
- lower motor neuron
- PLS
- primary lateral sclerosis
- UMN
- upper motor neuron
PLS is a progressive pure UMN disorder first described in the late 1800s by Charcot and Erb; it can be distinguished from ALS by its characteristic absence of LMN signs. Both conditions arise sporadically, and both have been linked to specific mutations,1 though PLS is far less common than ALS, constituting as little as 1% of motor neuron diseases.2 Since diagnostic criteria for PLS were first proposed,3 reports have questioned its distinction from ALS, instead viewing PLS as an indolent variant with an exclusively UMN presentation.4–6 However, further case series7,8 have underscored the association between longer survival time and UMN-predominant disease, making the distinction between ALS and PLS clinically relevant and suggesting at least a separate syndromology.
ALS and PLS share MR imaging features such as T2 hyperintensity within the CST,9–11 atrophy of the motor and premotor cortex,3,12 MR imaging signal-intensity changes within the precentral gyrus,10 and decreased FA on tensor imaging of the descending motor pathway.13,14
Furthermore, PLS and ALS both manifest involvement of the CC, including loss of contralateral motor inhibition on behavioral testing,15,16 decreased FA on DTI,17,18 and an isolated report of callosal T2 hyperintensity in a case of ALS.19 We present 2 cases of PLS demonstrating increased T2/FLAIR signal intensity within the posterior body of the CC and discuss their relevance to understanding the topographic distribution of cortico-cortical interhemispheric projections.
Case Reports
The 2 patients presented herein were referred from the neurology department with a diagnosis of PLS. For both patients, clinical and laboratory findings were consistent with a diagnosis of “clinically pure PLS” according to the diagnostic criteria put forth by Gordon et al.7
Case 1
A 50-year-old man presented for adjustment of his medications. His medical history was significant for the onset of progressive right-leg weakness beginning in his late 20s, followed 3 years later by right upper extremity weakness. Within 5 years, spasticity and weakness of all 4 extremities prevented the patient from working. Electromyography was negative for lower motor neuron involvement. As the disease progressed, the patient became wheelchair-dependent. One year prior, he underwent bilateral tendon release surgeries for Achilles contractures.
His examination was significant for hyperreflexia and spasticity in all 4 limbs, minimal voluntary movement of his upper extremities, lower extremity paresis, and dysarthria.
Case 2
A 59-year-old man, diagnosed previously with multiple sclerosis presented to the neurology clinic for a second opinion. He experienced the onset of right-hand weakness at 39 years of age, and during the next decade, developed right-leg weakness, dysarthria, and chronic urinary urgency. Neurologic examination in the clinic demonstrated right-sided spasticity, right pronator drift, dysarthria, frontal release signs, and global hyperreflexia. Ankle clonus and Babinsky signs were elicited bilaterally. Lumbar puncture was negative for oligoclonal bands.
Results
MR mages were acquired on a Magnetom Sonata 1.5T scanner (Siemens, Erlangen, Germany).
Case 1
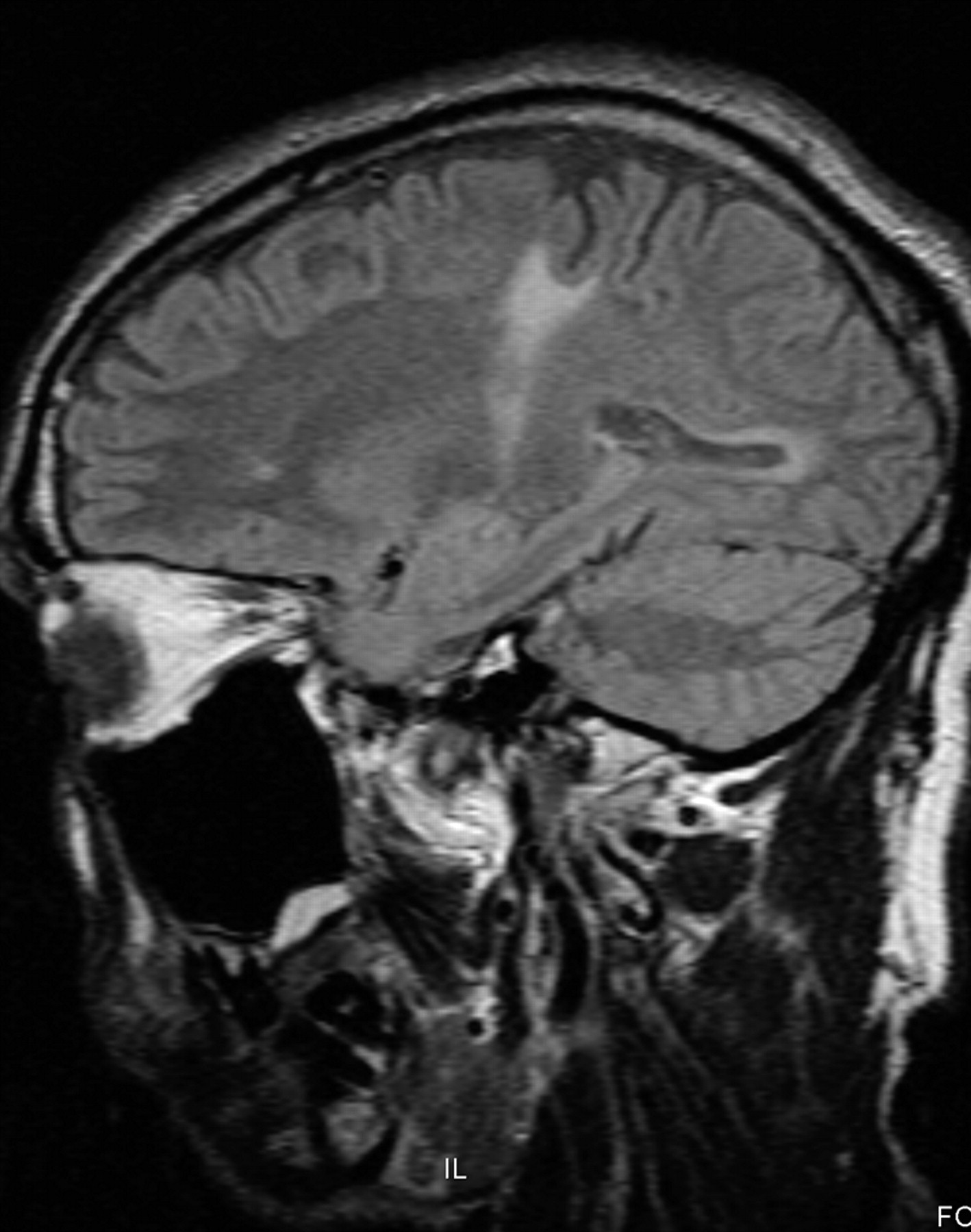
MR images included axial FLAIR (TR, 9000 ms; TE, 79 ms; TI, 2500 ms; flip angle, 15°; section thickness, 5 mm; matrix, 256 × 192; FOV, 240 × 240; NEX, 1), sagittal T1 (TR, 535 ms; TE, 15 ms; section thickness, 5 mm; matrix, 256 × 192; FOV, 240 × 240; NEX, 1), and coronal TI postcontrast sequences(TR, 687 ms; TE, 15 ms; section thickness, 5 mm; matrix, 256 × 192; FOV, 240 × 240; NEX, 1). Figure 1 is a representative axial FLAIR image (section 8) with a zone of T2 hyperintense signal in the left precentral gyrus extending across the CC toward the contralateral motor region. A midsagittal T1-weighted image from the same patient shown in Fig 2 (section 11) demonstrates focal volume loss in the posterior body of the CC. Figures 3 and 4 are coronal (section 9) and sagittal (section 14) T1 images demonstrating low signal within the CST. The bilateral CST involvement illustrated in Fig 3 was concordant with the patient's clinical presentation.

Case 1. Axial FLAIR image.

Case 1. Midsagittal T1-weighted MR image.

Case 1. Coronal T1-weighted MR image.

Case 1. Parasagittal T1-weighted MR image.
Case 2
Axial FLAIR (TR, 8000 ms; TE, 110 ms; TI, 2500 ms; flip angle, 15°; section thickness, 3 mm; matrix, 320 × 240; FOV, 240 × 240; NEX, 2), sagittal FLAIR (TR, 8710 ms; TE, 79 ms; TI, 2500 ms; flip angle, 15°; section thickness, 3 mm; matrix, 320 × 240; FOV, 240 × 240; NEX, 2), and coronal T1 postcontrast (TR, 450 ms; TE, 14 ms; section thickness, 3 mm; matrix, 256 × 192; FOV, 240 × 240; NEX, 2) sequences were performed. Figure 5A is a midsagittal FLAIR image (section 12) revealing T2 signal-intensity hyperintensity and volume loss in the posterior body of the CC. The parasagittal FLAIR image (section 19) in Fig 6 demonstrates T2 hyperintense signal within the expected course of the CST and corresponds to the distribution of T1 hypointensity in the coronal image shown in Fig 7. Figure 8is an axial FLAIR image (section 33); increased T2 signal intensity is demonstrated in the bilateral CSTs as they travel within the posterior limbs of the internal capsules. Bilateral CST involvement was concordant with the patient's clinical presentation.

Case 2. A, Midsagittal FLAIR image. B, Primary motor segment of the CC, as defined by tractography.27 Reprinted with permission from Hofer and Frahm,27 and the Copyright Clearance Center of Elsevier. C, Graphic overlay of images from Fig 5A and B. MR imaging findings depicted in Fig 5A appear to involve the primary motor segment of the CC.

Case 2. Parasagittal FLAIR image.

Case 2. Coronal T1-weighted MR image.

Case 2. Axial FLAIR image.
Region-of-Interest Analysis
Representative axial FLAIR images from patients 1 and 2 were selected, and regions of interest were generated within pathologic subcortical white matter (increased T2 signal) and normal-appearing ipsilateral white matter. A midsagittal FLAIR image from patient 2 (Fig 5A) was used for region-of-interest analysis of the CC: Regions of interest were generated within the pathologic white matter in the posterior body and the normal-appearing white matter in the anterior body. Measurements of region-of-interest area and signal intensity are displayed in the Table
Region-of-interest analysis for white matter MR imaging findings in cases 1 and 2
Discussion
The CC is the largest white matter tract in the human brain. Knowledge of its functional anatomy derives from several lines of inquiry. Aspects of callosal function are revealed through observation of individuals who have undergone callosotomy for intractable seizures, patients with so-called “split-brain.” Comparison of these patients with those with focal callosal lesions has led to inferences about the organization of transcallosal fibers. Autoradiographic techniques in primates have visualized transcallosal projections of the primary motor cortex to homotopic and heterotopic areas of the contralateral precentral gyrus.20 Postmortem studies in humans have revealed a topographic distribution of fibers in the CC21–23 and have demonstrated heterotopic and homotopic transcallosal projections.24
Transcranial magnetic stimulation, initially a technique used to assess CST integrity,25 has been applied to the study of cortico-cortical interactions. Meyer et al15 demonstrated that stimulation of the primary motor cortex inhibits the contralateral motor cortex, a finding diminished or absent in patients with callosal lesions. By comparing patients with a range of focal callosal lesions, the investigators deduced that motor inhibitory pathways occupy the posterior body of the CC.26 Loss of motor inhibition explains the finding of increased involuntary contralateral comovements in patients with ALS 16 and is consistent with decreased FA values in the CC of patients with ALS and PLS.17,18
The Witelson scheme for partitioning the midsagittal CC had been widely accepted for more than a decade on the basis of data derived from humans and nonhuman primates. The scheme has been challenged by data from DTI-based tractography,27 which modifies the standard scheme (Fig 9), relocating the Witelson motor region (II, anterior midbody) more posteriorly within the CC (III, posterior body). Figure 5B depicts the primary motor segment of the CC, as defined by the tractography data of Hofer and Frahm.27 Figure 5C is a simple overlay of the images in 5A and 5B, localizing the midsagittal MR imaging findings from patient 2 to the callosal motor segment.

Midsagittal schematic of the CC, showing Witelson scheme (top) and Hofer and Frahm scheme (bottom). Witelson scheme: I, premotor; II, motor; III, somesthetic; IV, parietal/temporal; V, temporal/occipital. Hofer and Frahm scheme: I, prefrontal; II, premotor; III, motor; IV, sensory; V, parietal/occipital/temporal. Note the posterior shift in the location of the primary motor segment from Witelson segment II to Hofer and Frahm segment III. Reprinted with permission from Hofer and Frahm,27 and the Copyright Clearance Center of Elsevier.
We presented 2 cases of PLS, a degenerative disease of the UMN, which demonstrate volume loss and high T2 signal within the posterior body of the CC, corresponding to the primary motor segment in the Hofer and Frahm revised topographic scheme of fiber distribution within the midsagittal CC.27
References
- Received November 30, 2009.
- Accepted after revision January 20, 2010.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}