
Abstract
BACKGROUND AND PURPOSE: DECT offers additional image datasets with potential benefits, but its use for H&N imaging is not justified unless image quality is preserved without increased radiation dose. The aim of this work was to compare image quality and radiation dose between a DE-derived WA image dataset and a standard SECT acquisition of the H&N.
MATERIALS AND METHODS: Thirty-two patients underwent DECT of the H&N (tube voltages 80 and Sn140 kVp) and were compared with the last 32 patients who underwent standard SECT (120 kVp) on the same dual-source scanner. WA images from the 2 DE tubes were compared with images obtained with an SE mode. Radiation doses and attenuation measurements of the internal jugular vein, submandibular gland, and sternomastoid and tongue muscles were compared. Objective image noise was compared at 5 anatomic levels. Two blinded readers compared subjective image quality by using 5-point grading scales.
RESULTS: CTDIvol was 12% lower with DE than with SECT, a difference of 1.5 mGy, (P < .0001). Objective noise was not significantly different between DE and SECT at any of the anatomic levels (P > .05). No significant differences in attenuation measurements were observed between DE and SECT (P > .05). No significant differences in subjective image quality scores were observed between DE and SECT at any of the 5 anatomic levels (P > .05).
CONCLUSIONS: DE-derived WA images of the H&N are equivalent to standard SE acquisitions and thus can be used for routine diagnostic purposes. Multiple additional image datasets can be obtained with no radiation dose penalty.
ABBREVIATIONS
- CI
- confidence interval
- CTDIvol
- CT volume dose index
- DE
- dual-energy
- DECT
- dual-energy CT
- DLP
- dose-length product
- H&N
- head and neck
- SE
- single-energy
- SECT
- single-energy CT
- WA
- weighted-average
DECT scanning refers to simultaneous acquisition of low and high peak voltage CT data. There is an increased interest in DE scanning, driven by the recent commercial availability of different DE hardware platforms (eg, dual-source CT and rapid kilovolt switching).1 DE scanning, in general, offers 2 main advantages: material characterization based on the difference in material and tissue attenuation observed at 2 different photon energies; and non-material-specific image fusion combining low and high peak voltage acquisitions.2 Material characterization proved beneficial for renal stone characterization, studying pulmonary perfusion through iodine distribution, and bone removal in CT angiography.3⇓⇓–6
Non-material-specific image fusion offers a wealth of information as well. Multiple additional image datasets could be generated, such as pure 80 kVp images with high contrast enhancement, pure 140 kVp images with low noise level, as well as any user-defined combination from low and high peak voltage acquisitions. This “linear image fusion” was used in CT angiography and liver imaging to increase the contrast-to-noise ratio.7,8 Moreover, a “nonlinear blending” method was described that selectively combines data from the 2 peak voltages according to a specific formula based on attenuation of structures of interest as a variable so that enhancement of such structures increases and background noise decreases.8,9
The H&N region is a well-known diagnostic challenge due to complex anatomy and diverse pathologic processes. The use of DE for H&N imaging seems appealing because of the possibility of generating multiple additional datasets based on both linear and nonlinear fusion, which would, theoretically, increase lesion contrast and decrease noise. Nonetheless, 2 conditions must be fulfilled before DE can be used for H&N imaging: First, images used for routine diagnosis must be of high diagnostic quality, at least comparable with the standard and well-optimized SE acquisitions; and second, the current DE scanning knowledge level does not justify any additional increase in a patient's radiation dose. The WA image dataset from the 2 tubes at a weighting factor of 0.3 from 80 kVp and 0.7 from 140 kVp was reported as equivalent to a standard acquisition at 120 kVp and was used for clinical interpretation in previous studies.10,11 To our knowledge, image quality of the WA image dataset has not been compared with standard SE acquisition of the H&N. Radiation doses of DE and SECT of the H&N have not been compared either.
The aim of this work was to compare image quality and radiation dose between a DE-derived WA image dataset and a standard 120-kVp acquisition of the H&N.
Materials and Methods
Subjects
This prospective study was approved by the institutional review board. Informed consent was obtained from patients for CT scans, including possible anonymous use of data for research purposes. The study group included patients scheduled for clinically indicated H&N CT with no contraindications to CT examination or iodinated contrast material. Thirty-two consecutive patients underwent CT of the H&N in the DE mode. The last consecutive 32 patients who were scanned in the SE mode on the same scanner were included as a control group. To ensure randomization, consecutive patients were included in both groups regardless of age, sex, or primary pathology. Indications for CT scanning were suspected inflammatory or neoplastic diseases or tumor staging. All patients had to be older than 18 years of age. Patients scheduled for noncontrast studies or CT angiography were excluded. Patients under follow-up after recent surgery or irradiation (within 6 months) were also excluded. The DE group included 21 men and 11 women with ages ranging from 23 to 87 years (mean, 58 ± 17 years), and the SE group included 20 men and 12 women with ages ranging from 26 to 82 years (mean, 50 ± 15 years). The number of cases was calculated after a pilot study on 10 patients and 10 control subjects; a power analysis (power set at 0.9) was performed to determine the number of cases needed for a relevant difference in noise (judged as 25% of the mean image noise at the aortic arch level).
CT Protocols
All patients were scanned by using a dual-source CT scanner (Somatom Definition Flash; Siemens, Erlangen, Germany), which allows the operator to choose between running each scan in SE or DE modes. This scanner is considered the second generation of dual-source scanners, in which a new tin (Sn) filter was implemented in the high-voltage tube. The DECT protocol was as follows: tube A operated at peak kilovoltage, 80 kVp; and tube B, at (Sn) 140 kVp; reference milliampere-second, 257 and 180 mAs, respectively; gantry rotation time, 0.5 seconds; pitch, 0.9; and section collimation, 0.6 mm. Reference milliampere-second is a parameter used to specify image quality for CT examinations performed with a combined modulation type of an automatic exposure-control technique (CareDose 4D, Siemens).12 It represents an effective milliampere-second used for a reference adult (70–80 kg) or reference child (20 kg). The effective milliampere-second is defined as the product of tube current gantry rotation time (milliampere-second) divided by the pitch. The SECT protocol was the following: tube peak kilovoltage, 120 kVp; reference milliampere-second, 180 mAs; rotation time, 1 second; pitch, 0.8; and collimation, 0.6 mm. Other scanning parameters were kept constant between the 2 groups. Imaging started 70 seconds after intravenous administration of 100-mL nonionic iodinated contrast agent Iomeprol (Imeron, 400; Bracco Imaging Deutschland, Konstanz, Germany). Weighted-average DECT images were reconstructed by the technician at a weighting factor of 0.3 from the 80 kVp and of 0.7 from the 140 kVp acquisitions in the same reconstruction thickness (2 mm) and with a soft-tissue reconstruction kernel (B30) similar to that in the SECT images.
Radiation Dose Measurements
CTDIvol and DLP were recorded for every patient from the patient's protocol page. An arbitrary estimate of the patient's size was taken as the transverse diameter of the neck anterior to the midbody of the fourth cervical vertebra.13 A patient's cross-sectional diameter or circumference is considered a better parameter for dose comparison and optimization than body weight because a patient's diameter better correlates with the distance of the pathway traversed by the x-ray beam, hence with attenuation and image quality, while persons with identical weight may differ in height and hence body habitus.14,15
Objective Image Analysis
One radiologist with 3 years' experience in H&N radiology reviewed all examinations to verify the absence of significant motion artifacts and selected 5 images representative of the following anatomic levels for each patient: nasopharynx at the fossa of Rosenmuller, floor of the mouth, arytenoids, lower thyroid, and aortic arch.
Mean CT attenuation numbers were obtained by placing circular regions of interest (20–60 mm2) in the sternomastoid muscle, internal jugular vein, submandibular gland, and tongue (genioglossus muscles). Average values from measurements on both sides were recorded. Objective image noise was obtained as the average SD of 2 circular regions of interest (300–500 mm2) placed in air on both sides in front of the patient (Fig 1).

Axial contrast-enhanced CT images obtained through the level of the floor of the mouth in 2 different patients. DE-derived WA image (A) and standard SE (120 kVp) image (B). Mean attenuation values (in Hounsfield units) of the sternomastoid muscle, tongue muscle, and internal jugular vein were obtained at this level by using circular regions of interest, as shown. Objective noise was obtained as the SD of the circular regions of interest drawn in air outside the patient. Noise was obtained in all anatomic levels in a similar way.
Subjective Image Analysis
All image annotations were then removed, and images were presented for 2 radiologists with 10 and 4 years' experience, respectively, in random patient order for each anatomic level separately. Blinded to the imaging-acquisition technique, the 2 radiologists in consensus subjectively rated each image on 5-point rating scales for subjective image noise defined as image graininess (ranging from 1 = marked unacceptable noise level to 5 = absent perceivable noise); image sharpness defined as delineation of organ contours (ranging from 1 = marked blurring to 5 = perfect delineation of contours); beam-hardening artifacts assessed at the lower thyroid and aortic arch levels (ranging from 1 = marked affecting diagnostic ability to 5 = absent artifacts); and finally, an overall image quality scale (1 = nondiagnostic, 2 = suboptimal, 3 = sufficient, 4 = good, 5 = very good).
Statistical Analysis
The means and SDs of metric data as well as the medians and ranges of ordinal scales were calculated. After testing continuous variables for normality by using the Kolmogorov-Smirnov test, an independent-samples t test was used to compare the means of patient ages, transverse neck diameters, CTDIvol, DLP, objective noise measurements, and attenuation measurements between DE and SECT. A nonparametric Mann-Whitney U test was used to compare subjective image-quality scores at each level.
Results
All patients completed CT examinations without complications. All CT scans were free of severe motion artifacts. There were no significant differences in the age and sex distribution between DE and SECT patients (P = .053 and 0.5). The transverse neck diameters were also not significantly different between DE (124 ± 12.3 mm) and SECT patients (123.6 ± 14.1 mm) (P = .89).
Radiation Dose
CTDIvol and DLP were 12% and 10% lower with DE than SECT, respectively. The mean ± SD CTDIvol was 10.96 ± 0.6 mGy with DE and 12.4 ± 1.4 mGy with SECT, and DLP was 305 ± 26.3 mGy cm with DE and 341 ± 52.9 mGy cm with SECT. The differences in CTDIvol and DLP were statistically significant (P < .0001 and P = .001).
Objective Image Analysis
Table 1 summarizes the results of objective noise measurements at the 5 selected anatomic levels. No significant differences in noise measurements between DE and SECT were observed at any of the 5 anatomic levels; all P values were >.05. As expected, noise was maximal at the level of arch of aorta and minimal at the arytenoid level with both DE and SECT.
Objective noise with DE and standard SECTa
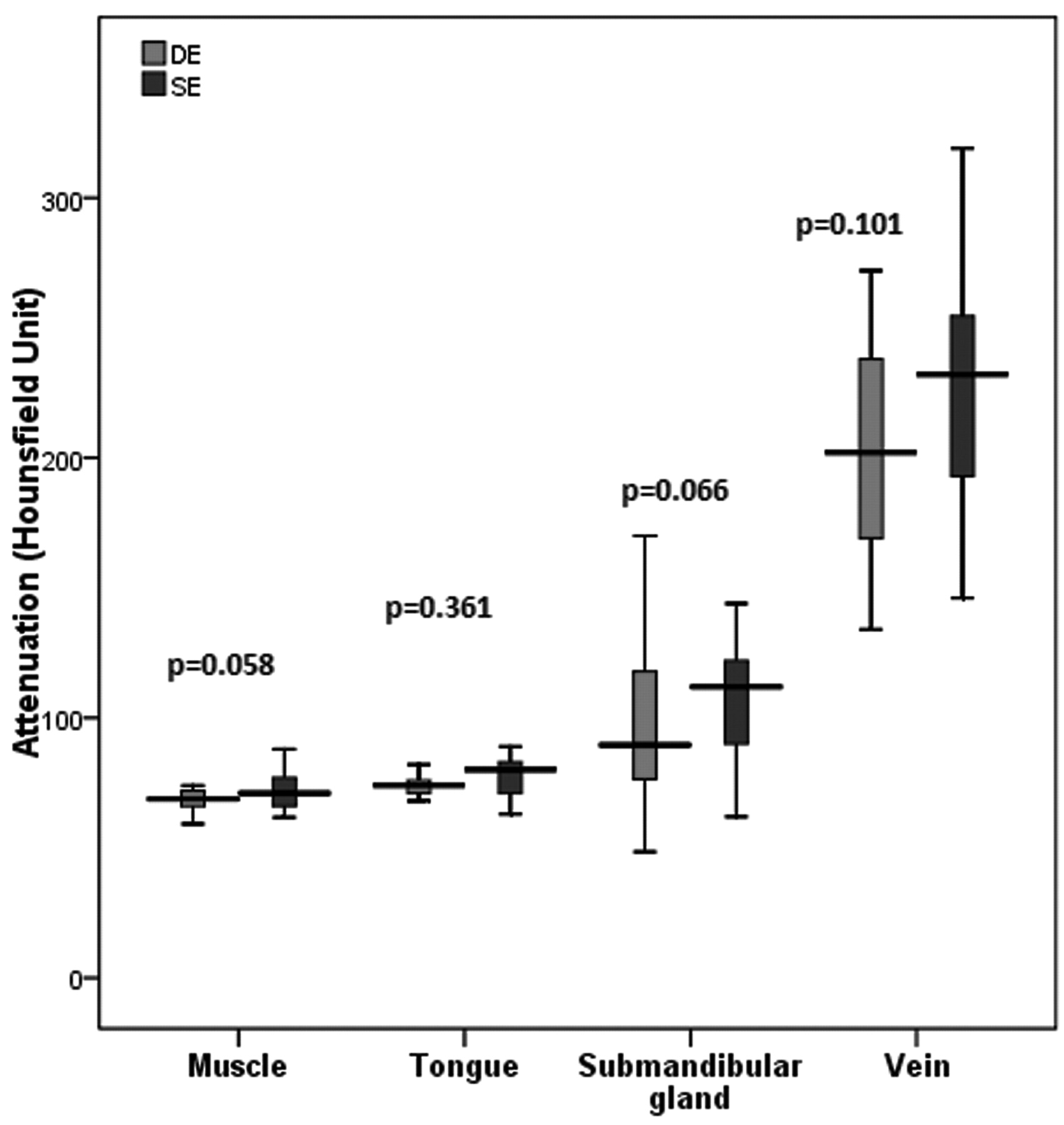
There were no significant differences between DE and SECT in muscle, submandibular gland, and tongue attenuation measurements; all P values were >.05 (Fig 2). Venous enhancement ranged between 134 and 319 HU and was >150 HU in all except 3 cases (2 DE, 1 SECT). The difference between mean venous enhancement with DECT (205.8 ± 41.3 HU) and SECT (224.2 ± 46.7 HU) was not significant (P = .101) (Fig 2).

Box-and-whisker plot of attenuation measurements with DE and SECT. Boxes represent the middle 50% of cases, horizontal lines within mark median values, and whiskers represent minimal and maximal extremes. Differences between attenuation values with DECT and SECT are nonsignificant (P > .05).
Subjective Image Analysis
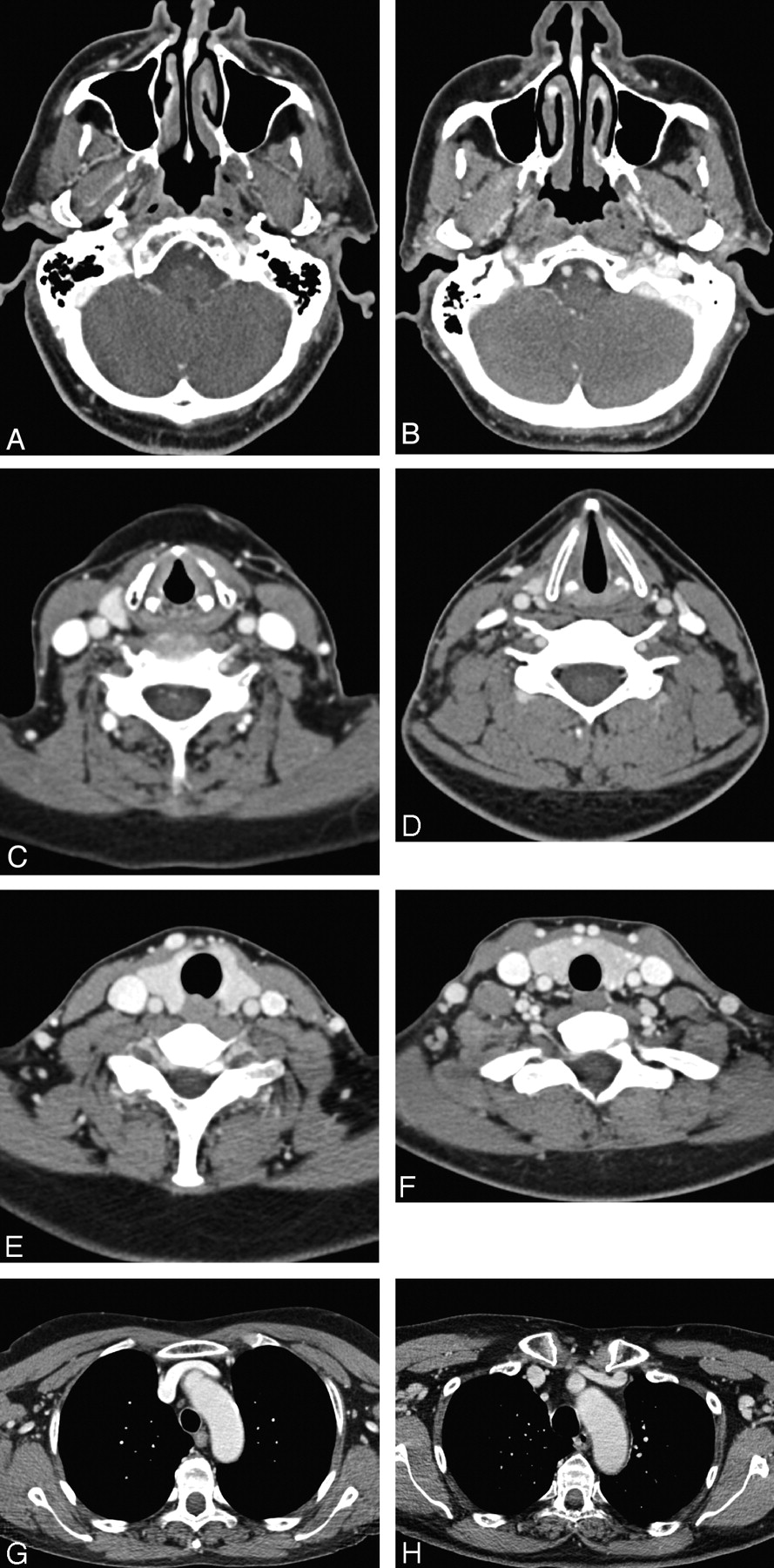
The results of subjective image analysis are summarized in Table 2. No significant differences in image noise, sharpness, or overall image quality were observed between DE and SECT at any of the 5 anatomic levels (Fig 3). No significant differences in streak artifacts were observed at the levels of the lower thyroid and arch of the aorta. The mean ranks (not shown) of overall image quality were slightly higher with DECT than with SECT at the nasopharynx and floor-of-the-mouth levels, slightly lower with DECT at the lower thyroid and arch-of-the-aorta levels, and nearly the same at the arytenoids level. The median image-quality scores were ≥3 (sufficient image quality) at all anatomic levels with both DE and SECT. None of the studies required repeat CT examinations as a result of unacceptable image quality.

Axial contrast-enhanced CT images through the nasopharynx (A and B), arytenoids (C and D), lower thyroid (E and F), and arch-of-the-aorta (G and H) levels in different patients. On the left panel are DE-derived WA images (A, C, E, G) and on the right panel are images acquired in single energy mode (B, D, F, H). There is no perceivable difference in image noise, sharpness, or overall image quality. All images are of excellent diagnostic quality.
Subjective image-quality analysis scores for DE and SECTa
Discussion
In this study, we showed that DE-derived WA images are equivalent to standard SE acquisitions and can be used for routine diagnostic purposes. Multiple additional image datasets are thus obtained with no radiation dose penalty. The CTDIvol and DLP were significantly lower by 12% and 10% with DECT compared with SECT protocols; with no significant differences in noise level, attenuation measurements, or subjective image quality between the 2 protocols. The described SECT protocol is routine for H&N imaging used at our institution, with lower radiation doses than other reported protocols16 and official dose limits.17
The introduction of DE scanning and dual-source CT was accompanied by concerns about increased radiation dose, as was the case with the early years of multidetector CT, because of the focus on optimization of image quality, ignoring the effect on radiation dose.16,18 Soon afterward, effort was directed toward decreasing radiation exposure, such as the installation of adaptive tube-current-modulation techniques in modern scanners.15,16,18,19 Increased awareness of radiologists and familiarity with scanning parameters affecting radiation dose are at least of equal importance.15 A good practice that must be encouraged by all radiologists is the comparison of radiation doses before applying any change of the scanning parameters and especially before implementing new protocols or techniques. Current CT scanners display the values for the CTDI and DLP on the operator's console, allowing comparison of patients' radiation doses from different imaging protocols.20 One should compare radiation doses with recent data rather than older publications at the beginning of the multidetector CT era, many of which report higher radiation doses.18
The assumption that the DE-derived WA image dataset is, by convention, equivalent to a standard 120-kVp acquisition could be challenged by the technical limitations of dual-source CT in the form of additional image noise caused by overlap between low- and high-energy photon spectra as well as scatter radiation from high-voltage tubes to low-voltage detectors.21,22 Early studies on abdominal DECT reported higher radiation doses because a higher tube current−time product was necessary for the 80 kVp acquisition due to the inherent lower penetration.23 Alternatively, the use of thicker collimation was recommended (1.2 mm instead of 0.6 mm) when possible.21 Compared with thoracic and abdominal imaging, H&N imaging is usually more demanding in terms of image quality but has the advantage of thinner cross-sections of anatomy. Thin collimation should be preserved because it is necessary for quality reformats, and noise levels should not increase. The described DE protocol in the current study with the new second-generation dual-source scanner implementing tin filtration for the high-voltage tube (supposed to decrease scatter radiation and extra noise) preserved thin collimation (0.6 mm) with no increase in noise level even with lower radiation doses than SECT. A similar protocol for chest DECT was reported by Schenzle et al,24 implementing thin collimation without an increase in noise or radiation dose compared with SECT (by using the same scanner as in the current study), while thicker collimation was necessary to maintain the noise level and radiation dose with a first-generation dual-source scanner.
If collimation was kept constant, then the trade-off is between image quality on one hand and radiation dose on the other. This is not an easy task. Image quality is not only a nonmeasurable entity, at least objectively, but it cannot even be precisely defined. Assessing image quality both objectively by noise and attenuation measurements11,13,25 and subjectively by experienced radiologists blindly rating images with predefined scores is generally accepted.11,13,16,18,25 The complex anatomy and wide variation of thickness and attenuation of the H&N region imply differences in noise levels and image quality; therefore, we chose representative anatomic levels similar to those described in a previous study,18 instead of collectively judging all images. Objective noise was similar with DE and SECT protocols at the 5 anatomic levels. As expected, noise was highest at the aortic arch and thyroid levels and lowest at the arytenoid level with both protocols. Objective noise measurements were generally satisfactory at all anatomic levels. Venous, muscle, submandibular gland, and tongue attenuation measurements were also comparable with both protocols. Subjective image noise, image sharpness, and overall image quality were also similar with DE and SECT protocols. Overall image quality was very good at the nasopharynx and floor of the mouth levels, good at the level of arytenoids, and sufficient or good at the lower thyroid and arch-of-the-aorta levels.
The current study has some limitations: First, image quality of DE-derived WA images was just comparable with, not better than, SECT. One would question using DECT in H&N imaging. However, the radiation dose of our DE protocol was 12% lower than that of SECT. It is very likely that improved image quality with DE would be observed if radiation doses were equal. Second, we evaluated only WA images with a single weighting factor and did not explore other weighting factors, though we believe the main clinical benefit of DE scanning of the H&N is the generation of additional datasets with improved image quality and increased lesion contrast enhancement. This study, however, highlights 2 main clinical points: the feasibility of DECT of the H&N with no radiation dose penalty and with preserved image quality for routine diagnosis, and the responsibility of radiologists for balancing radiation dose and image quality before any change in CT techniques. Further studies for evaluation of different DE applications (eg, linear and nonlinear blending methods as well as iodine distribution map) in H&N imaging are recommended.
Conclusions
This study showed that DE scanning can be used for imaging of the H&N either for diagnostic or research purposes and that the WA image dataset is comparable with a standard 120-kVp acquisition even when the radiation dose is lower by 12%. DECT has the added bonus of providing multiple additional datasets.
Footnotes
A.M.T. and J.M.K. contributed equally to the manuscript and would like to share first authorship.
-
Disclosures: Josef Matthias Kerl: Speaker Bureau: Siemens AG, Consultant: Siemens AG. Ralf Bauer: Research Support (including provision of equipment or materials): Siemens AG; Speaker Bureau: Siemens AG; Consultant: Siemens AG.
References
- Received December 7, 2010.
- Accepted after revision March 21, 2011.
- © 2011 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}