
Abstract
BACKGROUND AND PURPOSE: The use of Onyx in the treatment of intracranial AVMs has increased the cure rate of endovascular embolization compared with the use of liquid adhesive agents. Inadvertent occlusion of the draining veins before the complete exclusion of the nidus constitutes a major risk of bleeding. We report a case series using the technique of double simultaneous arterial catheterization as an approach to achieve the complete exclusion of the nidus before reaching the venous drainage, through a more controlled hemodynamic filling.
MATERIALS AND METHODS: Between April 2008 and November 2009, 17 patients with brain AVMs were treated by the DACT. The mean age of the patients was 32.7 years (range, 6–54 years), with 9 females and 8 males. The clinical onset was characterized by intracranial hemorrhage in 8 patients and by seizures in 7. The size of the AVMs ranged from 13 to 54 mm (average, 26.2 mm). The DACT was always used with the objective of curing the AVM.
RESULTS: All 17 patients completed the EVT. The average number of sessions conducted was 1.4 (range, 1–3 sessions), with the average injection amount of 6.9 mL of Onyx (range, 2–25.2 mL). Sixteen AVMs (94.1%) were angiographically cured by embolization. Clinical complications occurred in 2 patients (11.7%); 1 of these was permanent (5.9%). No deaths were registered.
CONCLUSIONS: This preliminary series shows that the DACT presents satisfactory results when used with curative intent.
Abbreviations
- ACA
- anterior cerebral artery
- AVM
- arteriovenous malformation
- DACT
- double arterial catheterization technique
- DMSO
- dimethyl-sulfoxide
- DSA
- digital subtraction angiography
- ECA
- external carotid artery
- EVD
- external ventricular derivation
- EVT
- endovascular treatment
- ICA
- internal carotid artery
- MCA
- middle cerebral artery
- MMA
- middle meningeal artery
- mRS
- modified Rankin Scale
- n-BCA
- n-butyl cyanoacrylate
The treatment of intracranial AVMs is complex and involves different approaches, such as endovascular embolization, neurosurgery, radiosurgery, and frequently the association of 2 or even 3 of these techniques.1
In EVT, the most adopted technique currently is the intranidal injection of a permanent liquid embolic agent, with the intent of completely excluding the AVM circulation or, when that is not possible, achieving the largest possible embolized amount of the AVM, allowing a complementary treatment by neurosurgery or radiosurgery.
n-BCA was the first liquid permanent embolic agent to be used in the EVT of brain AVMs, but it has demonstrated limited results because of its adhesive properties, which allow short injections of small amounts of embolic material during each catheterization, limiting the final results.2,3
Onyx (ev3, Irvine, California) is a nonadhesive polymer of permanent embolic agent introduced recently in the treatment of AVMs; it has shown favorable results compared with n-BCA for allowing the nidus to be filled more effectively.4–6 However, the increase in the cure rates of AVMs by EVT with Onyx has also been accompanied by considerable rates of complications, especially hemorrhagic. One of the most feared complications is the inadvertent occlusion of the draining veins of the AVM before the complete exclusion of the nidus, resulting frequently in bleeding.4,5
We describe a retrospective series of 17 patients with cerebral AVMs treated with the simultaneous DACT. The technical aspects of this approach were evaluated, as well as its immediate and late clinical and angiographic results.
Materials and Methods
Patients and AVM Demographics
Between April 2008 and November 2009, 17 patients with cerebral AVMs were selected for treatment with the DACT by using Onyx as embolic agent. We retrospectively evaluated the medical records of 11 patients treated at the Limoges University Hospital, University of Limoges, France, and of 6 patients treated at the University Hospital of the School of Medicine of Ribeirão Preto, University of São Paulo, Brazil. The mean age of patients was 32.7 years (range, 6–54 years), with 9 females and 8 males. The initial clinical presentation was secondary to rupture bleeding in 8 patients (47%), seizures in 7 (41.2%), and incidental diagnosis in 2 patients (11.8%) (Table 1). Of the 17 AVMs treated, 9 (52.9%) were located in the right cerebral hemisphere, 5 (29.4%) in the left hemisphere, 2 (11.8%) in the corpus callosum, and 1 (5.9%) in the cerebellum. The dimensions, measured along the longest axis of the AVM, ranged from 13 to 54 mm (mean size, 26.2 mm). Deep venous drainage was present in 4 AVMs. According to the classification of Spetzler-Martin,7 3 AVMs (17.6%) were classified as grade I; 5 (29.4%), as grade II; 6 (35.3%), as grade III, and 3 (17.6%), as grade IV.
Characteristics of the patients treated for intracranial AVMs with DACT
Embolization Procedure
All procedures were performed with patients under general anesthesia and were conducted by the same operators in each of the 2 centers (C.M. at the Limoges University Hospital and D.G.A. at the University Hospital of Ribeirão Preto).
We selected only plexiform AVMs for this technique, and no AVMs in this series had intranidal fistulas. Therefore, only Onyx 18 was used.
Catheterization was performed by a coaxial system through a bilateral femoral approach with 6F sheaths in all patients. After femoral puncture, 3000 IU of heparin was administered intravenously, with supplements of 1000–2000 IU every 2 hours during the procedure. After completing DSA, we placed two 6F guiding catheters, according to the location of the feeding arteries of the AVMs.
Through each guiding catheter, a DMSO-compatible microcatheter (Marathon, ev3) was advanced, with the help of an 0.08-inch microguidewire (Mirage, ev3). We preferred to advance the first microcatheter to a position near the nidus and then the second one to an intranidal position. Only then was the first microcatheter finally advanced to its intranidal position. We chose this approach with the intent of preventing any hemorrhagic complication by reducing as much as possible the length of time that the microcatheter would touch the nidus before the Onyx injection.
The angiographic projections used as working views could show the microcatheters separately from each other and without superimposing the AVM nidus, thus allowing a better control of the Onyx reflux in both microcatheters during injection, as well as its progression to the venous side.
After the intranidal placement of both microcatheters, the first one was washed with 0.3 mL of DMSO, followed by slow injection of Onyx for 40 seconds to fill the microcatheter lumen. Thereafter, under subtracted fluoroscopy, we started gradual injection of Onyx, stopping when the first reflux of the material occurred. At this point, we moved to the second microcatheter and followed the same steps. As soon as we saw the embolic agent coming out of the second microcatheter, we restarted the injection through the first microcatheter (usually 2 minutes after the first break). The injection of Onyx was then performed simultaneously with a syringe in each hand. At every arterial reflux, the injection was interrupted for 1–2 minutes and then resumed. After the end of the injections, each microcatheter was gently stretched every 1–2 minutes. When the microcatheter acquired a tense and semirectified position, it was withdrawn with gentle short movements.
Postprocedural Management
After the end of each procedure, all patients underwent CT of the brain. In the absence of complications, they were extubated in the operating room and kept for 48–72 hours in the intensive care unit under strict blood pressure control. Corticosteroids were administrated orally for 5 days after the procedure.
Clinical and Angiographic Follow-Up
According to our protocol, all patients with AVM cured by endovascular surgery undergo a complete cerebral DSA 6 months after completion of treatment. Patients who undergo surgery after embolization undergo a cerebral DSA before discharge to check the complete removal of residual nidus.
The patients were clinically evaluated before and after the procedure, then daily until discharge, at angiographic follow-up 6 months after the treatment, and then annually.
Rationale and Indications for Treatment
The DACT using Onyx was applied only in cases of selected plexiform AVMs, which had an angioarchitecture favorable for a curative treatment—that is, when the embolization session was planned to be the last one. Basically, the main criterion in choosing this procedure was whether the AVM could be cured in just 1 session; it could be the first session for a small untreated AVM or the last one for a remaining nidus previously treated. We always applied the intranidal technique, intending to place the microcatheter in a position as distal as possible, where the arterial inflow of the AVM could be blocked by the microcatheter.
The hemodynamic effect caused by the blockade of 2 afferent arteries in 1 AVM with few arterial afferents (a small AVM or reduced by previous embolization) seems to favor the filling of the nidus by the embolic material before it reaches the venous side.
In large AVMs, the staged treatment was always chosen, with an interval of 2–3 months between each session. At the first session, we started with embolization of the pedicles of greater caliber, to reduce the intake pressure of the AVM. The double catheterization was performed when the AVM had reached a size eligible for curative treatment.
Results
Anatomic Results
The 17 patients included in the study completed the series of EVTs. We performed 1–3 sessions per patient (mean, 1.4 sessions) (Table 2). The mean volume of Onyx injected per AVM was 6.9 mL (2–25.2 mL). When we analyzed only the double injections, the mean volume of Onyx injected was 5.1 mL (2–10.4 mL).
Treatment results and complications
Of the 17 AVMs treated, 16 (94.1%) could be completely angiographically excluded without any other complementary treatment besides the embolization. Only 1 patient, who had a large left parietal AVM, did not have complete treatment of the AVM exclusively by the endovascular approach. After injection of 10 mL of Onyx by using the DACT, we obtained an occlusion of about 90% of the nidus and the patient underwent surgical resection of the remaining nidus 2 days after the procedure.
All 17 double catheterizations were performed with curative intent. In 3 of the 16 patients cured by embolization, 1 last simple catheterization was necessary to complete the nidus occlusion after the double catheterization. Of those AVMs that needed 1 more last catheterization, 2 were angiographically excluded by 1 more injection of Onyx and 1 by injection of Glubran 2 (GEM, Viareggio, Italy) at a 20% dilution. In the latter case, the use of diluted Glubran 2 was preferred due to the unfavorable angioarchitecture of the access to inject Onyx.
Clinical Outcome and Complications
According to the mRS, 15 patients were functionally independent before the EVTs (mRS, 0–2). Of those, 2 patients had immediate neurologic worsening after the procedure (mRS, 3–5), though 1 of them was already independent at the time of discharge. Late clinical evaluation (6 months) was possible for 15 patients. Of those, 12 patients were independent at the time of discharge, and none of them had clinical deterioration. The 2 patients who were dependent before the procedure, as a consequence of hemorrhagic events caused by the AVMs, were independent at the time of the late clinical evaluation. The only patient who became dependent at the time of discharge maintained the same clinical state at late re-examination.
We had 2 technical complications during the treatment of the 17 AVMs included in the study, 1 resulting in permanent neurologic deficit.
One complication occurred in a 6-year-old boy harboring a previously ruptured AVM of the corpus callosum treated in a single session. After the double-catheter injection of 5 mL of Onyx through both ACAs, most of the AVM was excluded, but we could still identify circulation at the posterior region of the nidus. Through the right occipital artery, we gained access into the remaining nidus and completed the embolization with the injection of 2 mL of Onyx. However, the pedicle artery ruptured during the withdrawal of the microcatheter. The damaged artery was immediately treated with an injection of n-BCA. The CT scan after the procedure showed ventricular hemorrhage, and an EVD was placed promptly. The patient has undergone 6-month angiographic follow-up and is asymptomatic.
The other complication occurred in a 33-year-old female patient with a right posterior frontal AVM treated in 2 sessions. During the last session, a hemorrhagic complication occurred; however, it was promptly resolved by continuous injection of Onyx until complete nidus exclusion. The CT scan after the procedure showed ventricular hemorrhage. The next day the patient received an EVD, which was complicated by a basal ganglia hematoma, and the patient remained hemiplegic. Late angiographic evaluation (6 months) demonstrated total occlusion of the AVM.
Angiographic Follow-Up
Of the 16 patients who had their AVMs completely excluded by embolization, 14 (14/16, 87.5%) underwent an angiographic follow-up 6 months after the conclusion of the EVT, and all of them showed stable AVM occlusion. One patient had subtotal embolization of the AVM and underwent surgery for resection of the remaining nidus 2 days after the embolization. The angiographic evaluation before discharge showed complete resection of the residual nidus. Two patients have not undergone 6-month angiographic follow-up.
Illustrative Cases
Case 1.
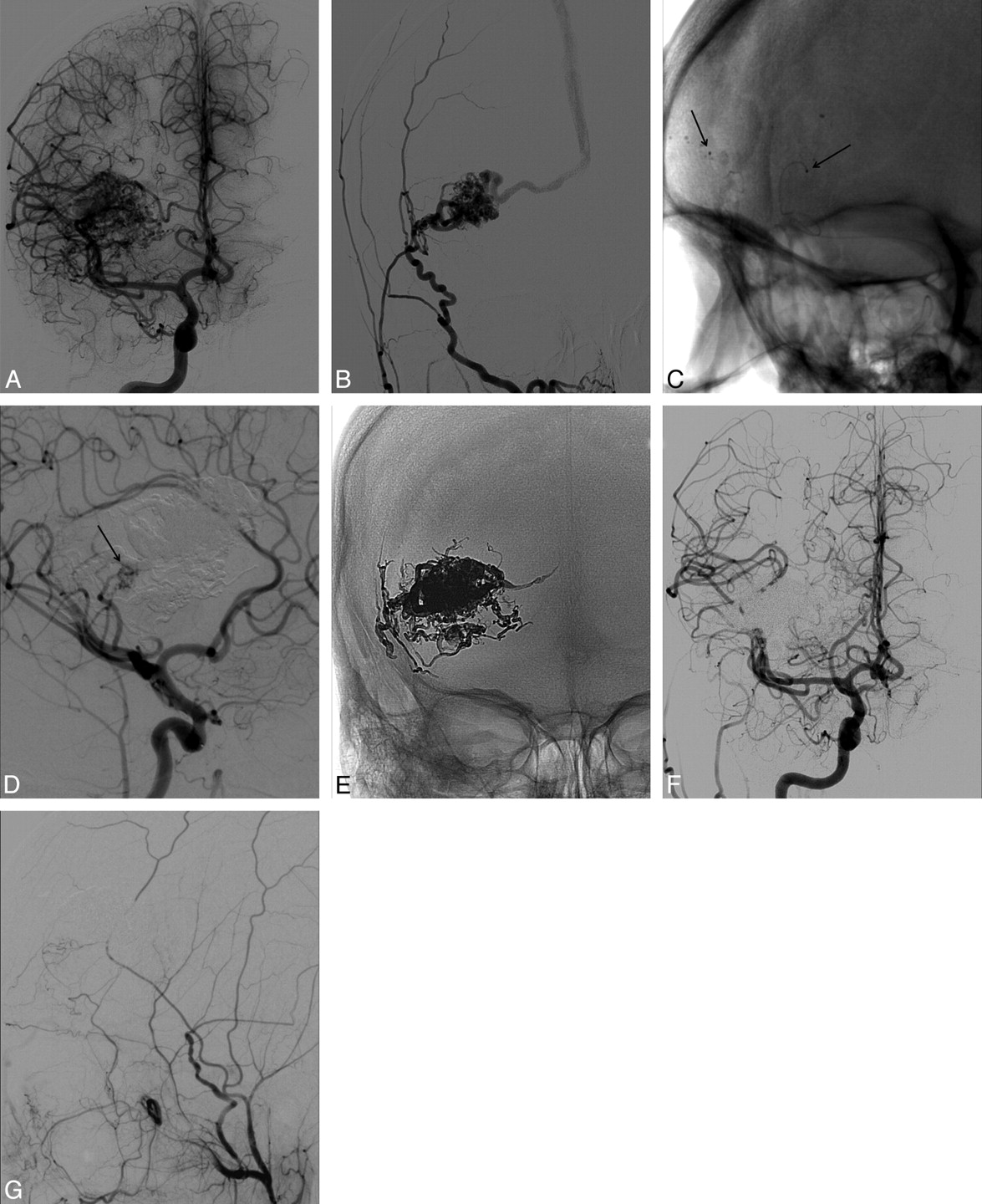
A 51-year-old female patient had a right posterior frontal AVM, which had been previously treated in another hospital with 3 sessions of embolization by using n-BCA, complemented at that time with radiosurgery. Late angiographic follow-up, performed 8 years after the last treatment, showed a large residual nidus, with vascular nourishing by afferent arteries of small caliber from the anterior and middle cerebral arteries (Fig 1A) and also nutrition through aspiration of arterioarterial anastomosis of the MMA with a frontal branch (Fig 1B). A DACT was performed with 1 access through the MCA and the other through the MMA (Fig 1C). After the injection of 3.2 mL of Onyx by double catheterization, a small residual nidus filled by the MCA was still detectable on the DSA (Fig 1D). One microcatheter was conducted into the afferent artery from the MCA, and after injection of 0.6-mL Glubran 2 diluted at 20%, a complete angiographic exclusion of the AVM was achieved (Fig 1E−G).

A 51-year-old female patient harboring a right frontal AVM previously treated with embolization with n-BCA, followed by radiosurgery in 2001. A, DSA, frontal view, right ICA injection, demonstrates the remaining nidus fed by tiny branches from the ACA and MCA. B, DSA, lateral view, right ECA, shows arterial nourishing from the MCA, through collaterals with a frontal branch of the ACA, which are filled by arterioarterial aspiration of the MMA. A superficial draining vein is also visualized. C, Plain radiography shows the 2 microcatheters, 1 placed in the MMA and the other positioned in the MCA (black arrows). D, DSA, right ICA, right oblique view, shows persistence of a small residual nidus after injection of 3.2 mL of Onyx (black arrow). E, Plain radiography, frontal view, shows the final cast of Onyx and glue after the end of the treatment. F and G, DSA, ICA frontal view (F) and ECA lateral view (G), demonstrates complete exclusion of the AVM after embolization.
Case 2.
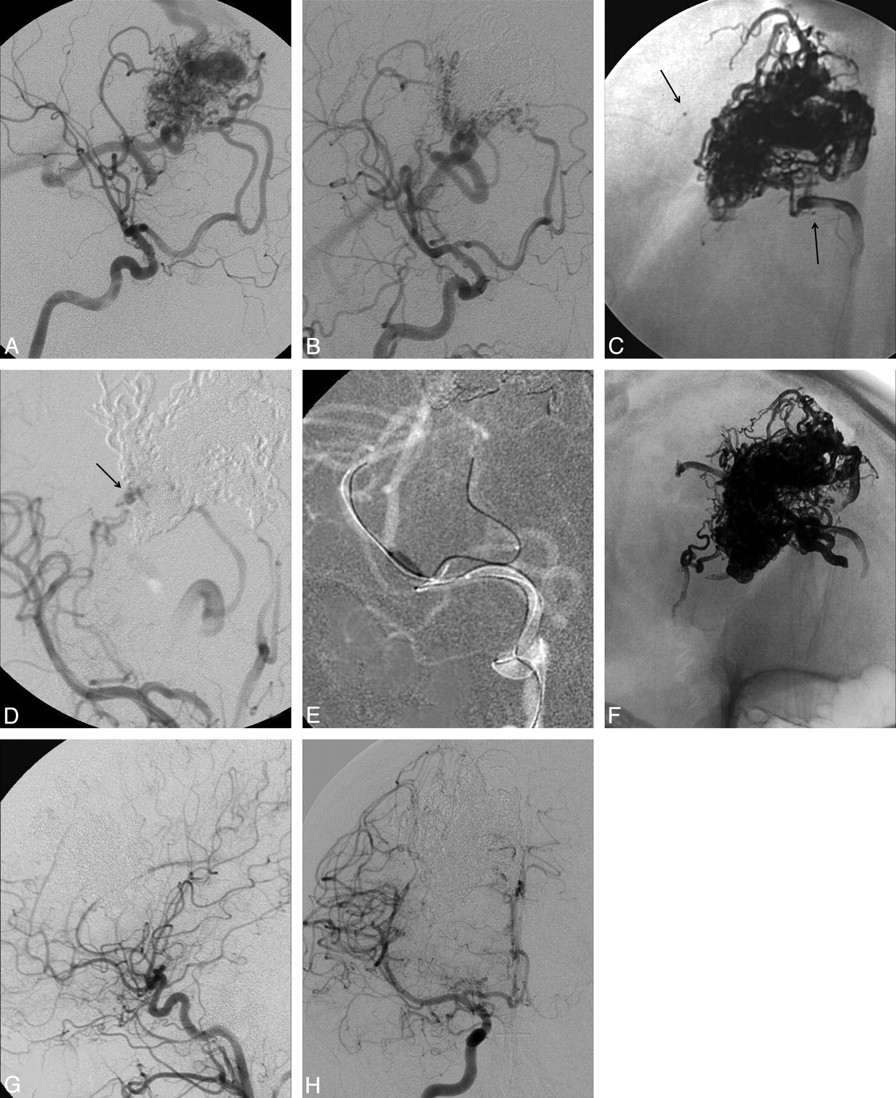
A 13-year-old girl was admitted in a coma after intraparenchymal hemorrhage and underwent surgical evacuation of the hematoma. Cerebral DSA showed a right posterior frontal AVM with superficial and deep drainage (Fig 2A). Three months later, the patient remained with a discrete left hemiparesis, and the EVT of the AVM was started. Two sessions of embolization with Onyx were performed, excluding the AVM superficial portion and superficial venous drainage (Fig 2B). In the third and last session, a DACT was performed. One microcatheter was positioned through an MCA branch, and the other, through the ACA (Fig 2C). After the injection of 9.5 mL of Onyx, only a small and deep remnant nidus, fed by a thalamic perforating artery from the MCA, could be identified (Fig 2D). The positioning of the microcatheter in the perforating artery needed to be supported by a HyperForm balloon, 4 × 7 mm (ev3), because of the angle of the artery (Fig 2E). After the new injection of 1.2 mL of Onyx, the complete angiographic exclusion of the AVM could be obtained (Fig 2F, -G). Despite the considerable amount of reflux obtained during the last injection, the microcatheter could be retrieved without any difficulty, and the patient did not show deterioration of her neurologic status (Fig 2F). The angiographic follow-up 6 months after treatment showed stable occlusion of the AVM (Fig 2H).

A 13-year-old girl harboring a ruptured right frontal AVM. A, DSA, right oblique view, right ICA injection, demonstrates a frontal AVM nidus fed by branches from ACA and MCA. B, DSA, right oblique view, right ICA injection, shows a deep remnant nidus after 2 sessions of embolization. C, Plain radiography, right oblique view, shows the 2 microcatheters, 1 placed in the ACA and the other placed in the MCA (black arrows). D, DSA, right ICA, right oblique view, demonstrates the small remnant nidus after the injection of 9.5 mL of Onyx (black arrow). E, ICA roadmap image, left oblique view, shows the catheterization of the feeder artery helped by a HyperForm balloon. F, DSA, right ICA, plain radiography, right oblique view, shows the final cast of Onyx after the end of treatment. G, DSA, right common carotid artery, lateral view, at the end of treatment, demonstrates complete exclusion of the AVM. H, DSA, right ICA, frontal view at 6-month follow-up, shows the stability of the occlusion.
Discussion
AVMs are a cerebrovascular alteration that accounts for a cumulative risk of functional disability or death due to intracranial bleeding and refractory epilepsy.8 However, they may also remain silent for long periods and may never manifest any clinical symptoms. Their incidence is estimated at approximately 1–2 per 100,000 per year, with the average age at diagnosis between 30 and 40 years, affecting both sexes equally.9 The most frequent clinical presentation is intracranial hemorrhage, followed by epilepsy, chronic headache, and focal neurologic deficits unrelated to hemorrhage.10
The treatment of cerebral AVMs is complex and frequently multidisciplinary. Currently, there are 3 options of treatment for intracranial AVMs: neurosurgical resection, radiosurgery, and endovascular embolization, with frequent association of >1 method.1
Since the first report of a cerebral AVM treated by endovascular approach by Luessenhop and Spence in 1960,11 the method has evolved significantly and the pedicular embolization with solid particles and coils was substituted for intranidal injection of acrylic glue. The intranidal technique with injection of n-BCA allowed a more effective treatment of AVMs; however, due to its adhesive properties, it was still limited in obtaining angiographic cure, with the best reported results around 30% for pure plexiform AVMs.12
Only a few years ago, after the introduction of Onyx as a new nonadhesive material of permanent embolic agent, a more aggressive approach toward these lesions by EVT was possible.4,5 Thanks to its nonadhesive properties, a better control during injections could be achieved. Onyx consists of a solution comprising ethylene-vinyl alcohol copolymer dissolved in DMSO. Tantalum powder is added to the mixture to provide visualization under fluoroscopy. It presents a low precipitation rate and thus permits more controlled and longer injections compared with n-BCA.
The results of endovascular treatment of cerebral AVMs with Onyx are very heterogeneous. Series report from 8.3% to 53.9% of angiographic cures.4,5,13,14 This finding is partially explained by the different embolization purposes established by each group. The endovascular embolization can have a preparatory intent when used to reduce the nidus size to facilitate the completion of the treatment, whether by surgery or by radiosurgery.15,16 Such a conservative approach tended to show lower rates of complications17 but had low effectiveness in the complete treatment when analyzed as a single method. On the other hand, series of AVMs embolized with curative intent showed results as high as 49%5 and 53.9%4 of total occlusion, albeit with the onus of higher rates of complications, especially bleeding. Total angiographic exclusion is associated with higher rates of hemorrhagic complications. Despite the nonadhesive characteristics of Onyx, an absolute controlled injection is still not possible due to its liquid nature. Its unpredictable course can lead to an inadvertent occlusion of draining veins of the malformation before the total exclusion of its nidus, resulting in sudden increase of intranidal pressure and consequent bleeding.
In our series, we could obtain complete angiographic exclusion in 94.1% of cases (16 of 17 patients). This rate is higher than that in all other reports using Onyx as an embolic material in the treatment of brain AVMs. However, these results may not be directly comparable because our analysis was based on the results of a specific group of patients considered as potentially curable by EVT.
The reasoning behind the intranidal progression of Onyx in the treatment of cerebral AVMs is based on a balancing of pressures. At first, the embolic material progresses in its liquid state into the nidus (first entry). Once a small portion of the nidus is occluded and Onyx begins to solidify, it tends to flow back along the afferent artery through which the microcatheter is positioned. As the reflux occurs, the arterial access is occluded by the solidification of Onyx enclosing the microcatheter. At that point, we have the second entry, when the resistance to the Onyx flow becomes smaller within the nidus than that offered by the solidified plug in the afferent artery. It is usually during the second entry that the largest and most effective penetration of Onyx into the nidus occurs.
In the single-catheterization approach, usually when the influx of Onyx is achieved during the second entry (due to occlusion of the arterial afferent by a solidified plug), there is still direct blood inflow through other pedicles nourishing the nidus. This blood flow with high debt tends to compete with the Onyx in its liquid or semiliquid state for the intranidal filling. This arterial opposition to the progression of Onyx may lead to an early passage of the liquid embolic agent to the venous site of the AVM, toward a lower resistance zone.
Once the Onyx reaches the drainage vein, the injection can be stopped and restarted after solidification of the embolic material. At this new pressure balance, with blockage of the venous filling, the Onyx inflow should be preferentially redirected to the nidus. However, this hemodynamic response to the venous occlusion is not completely controllable and thus is potentially dangerous. If the nidus is not completely excluded, there is a high risk of bleeding as the venous drainage is impeded.
The theory of double catheterization is based on the observation that in small AVMs with few afferent arteries or in residual partially embolized AVMs, when the last remaining pedicles with large caliber are simultaneously catheterized, the reflux obtained after the first entry tends to occlude the major nourishing of the AVM. In this configuration, with occlusion of the most important afferents, only small feeder arteries and recruited collateral arteries remain open. With direct reduction of blood inflow into the nidus and hence the flow competition with the penetrating Onyx during the second entry, intranidal filling can be achieved more effectively before passage to the vein.
Thus, we use this technique only with curative intent when there are not many remaining direct afferents. In large AVMs, injection through 2 microcatheters simultaneously may not have the same effect because many other pedicles still remain open, thus competing with the Onyx inflow. In our opinion, the AVMs suited for treatment by double catheterization should be small with few afferents or previously embolized afferents.
Lopes et al18 recently described a double-catheterization technique for treatment of brain AVMs with Onyx, similar to that reported in this study. The main difference between the 2 techniques is that once the dual catheterization was completed, they just injected Onyx through 1 syringe at a time, whereas we prefer to inject the material simultaneously with 1 syringe in each hand. The effect of simultaneous double injection is then optimized, favoring, hemodynamically, the progression of embolic material into the nidus.
A hemorrhagic event is the most common complication in the endovascular treatment of AVMs with Onyx, and its frequency varies from 5.9% to 16.7%.4,5,19 Hemorrhagic complications may occur for many reasons such as perforation during catheterization, arterial rupture caused by the withdrawal of the microcatheter, venous thrombosis stasis caused by the reduction of flow in the AVM, or by inadvertent venous occlusion in a nidus partially treated.
One hemorrhagic complication (5.9%) of our series occurred by rupture of the pedicle artery during removal of the microcatheter. In this case, the bleeding was immediately resolved after a new microcatheterization and injection of n-BCA. However, it resulted in intraventricular hemorrhage, which required placement of an EVD. The other complication that occurred in our series was caused by rupture of the nidus during Onyx injection that also resulted in intraventricular hemorrhage and the necessity of an EVD. Unfortunately, the accidental misplacement of the EVD caused a permanent neurologic deficit in the patient. Although the DACT is more complex than the single injection technique, our rate of permanent morbidity of 5.9% is comparable with that in the larger series of standard embolization by using Onyx with curative intent.4,5
Because of its less adhesive characteristics, the risk of having complications during withdrawal of the microcatheter appears to be lower with Onyx than with the use of n-BCA; nevertheless, the tortuosity of the access and the amount of reflux are still limiting factors of the method and should be well analyzed before and during the injection. The reflux of Onyx around the catheter solidifies only after several minutes. However, depending on the extension of the catheter that is involved by the Onyx, the reflux can have the same adhesive effect as a glued catheter using n-BCA. Recently, Maimon et al20 reported 1 series that showed good results of brain AVM embolization with Onyx by using a microcatheter with a detachable tip (SONIC; Balt, Montmorency, France), and perhaps this is a possible solution to this problem.
No patient had early or late bleeding after treatment in our study. All 14 patients completely cured by EVT who underwent DSA 6 months after completing treatment presented with stability of the occlusion; however, because none of the patients have been studied at intervals longer than 6 months after treatment, the true incidence of cure has not been established yet.
Conclusions
Preliminary results obtained in this series of cerebral AVMs treated with the DACT showed high rates of complete angiographic exclusion by EVT as a single treatment with acceptable rates of clinical complications, and DACT should be considered as another tool in the management of this complex pathology. Nevertheless, we have to consider the lack of long-term angiographic follow-up in the study and the small size of our series, which included only selected AVMs considered as potentially curable by EVT.
References
- Received March 30, 2010.
- Accepted after revision June 12, 2010.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Advanced brain arteriovenous malformation embolization techniques
- ihtObtura: A novel liquid embolic agent with post-embolization radiopacity loss, in endovascular treatment of brain arteriovenous malformations, dural arteriovenous fistulas, and tumors: CLARIDAD trial
- ihtObtura: A novel liquid embolic agent with post-embolization radiopacity loss, in endovascular treatment of brain arteriovenous malformations, dural arteriovenous fistulas, and tumors: CLARIDAD trial
- Republished: Multiplug flow control technique as a novel transarterial curative approach for the endovascular treatment of cerebrovascular malformations
- Multiplug flow control technique as a novel transarterial curative approach for the endovascular treatment of cerebrovascular malformations
- First clinical multicenter experience with the new Scepter Mini microballoon catheter
- Endovascular treatment as the main approach for Spetzler-Martin grade III brain arteriovenous malformations
- Transarterial Treatment of Cranial Dural Arteriovenous Fistulas: The Role of Transarterial and Transvenous Balloon-Assisted Embolization
- Overview of the current concepts in the management of arteriovenous malformations of the brain
- Endovascular Treatment for Low-Grade (Spetzler-Martin I-II) Brain Arteriovenous Malformations
- Extra-small dual-lumen micro-balloon catheters can improve endovascular embolization: an experimental in vivo and in vitro study
- Investigation of a New Version of the Liquid Embolic Agent PHIL with Extra-Low-Viscosity in an Endovascular Embolization Model
- Extending the indications for transvenous approach embolization for superficial brain arteriovenous malformations
- Neurological outcomes and cure rates of embolization of brain arteriovenous malformations with n-butyl cyanoacrylate or Onyx: a meta-analysis
- Endovascular treatment of unruptured and ruptured brain arteriovenous malformations with Onyx18: a monocentric series of 84 patients
- Transarterial balloon assisted Onyx embolization of pericallosal arteriovenous malformations
- Curative Embolization of Brain Arteriovenous Malformations with Onyx: Patient Selection, Embolization Technique, and Results