
Abstract
SUMMARY: Primary AT/RT is a rare highly malignant tumor of the CNS, usually occurring in children younger than 5 years of age. The objective of this study was to characterize the CT and MR imaging findings in a series of 5 adult patients with pathologically proved AT/RT. All 5 AT/RTs were supratentorial. In 2 patients who underwent nonenhanced CT, the tumors appeared isoattenuated, and 1 of the 2 tumors contained calcifications. Solid portions of the tumors on MR imaging were isointense on T1-weighted, T2-weighted, and FLAIR images, and 1 case showed restricted diffusion on DWI. The tumors also demonstrated a bandlike rim of strong enhancement surrounding a central cystic area on contrast-enhanced T1-weighted imaging. One tumor was associated with destruction of the calvaria. Although AT/RTs can have nonspecific findings, the tumors in our series were large and isointense on T1-weighted, T2-weighted, and FLAIR images with central necrosis and prominent rim enhancement.
Abbreviations
- ADC
- apparent diffusion coefficient
- AT/RT
- atypical teratoid/rhabdoid tumor
- CNS
- central nervous system
- DWI
- diffusion-weighted imaging
- FLAIR
- fluid-attenuated inversion recovery
- L
- left
- mRNA
- messenger ribonucleic acid
- N/A
- not available
- ND
- not depicted
- OS
- overall survival
- PNET
- primitive neuroectodermal tumor
- PR
- partial resection
- R
- right
- TR
- total resection
Although AT/RT was first described as a rare, highly malignant childhood neoplasm of the kidney, it has also been reported at several extrarenal sites including the skin, chest wall, liver, thymus, optic nerve, and the CNS.1–16 When found in the CNS, it usually arises from the posterior fossa and is most commonly found in children younger than 5 years of age.17 To our knowledge, only 29 cases of primary AT/RT of the CNS in adults have been reported (On-line Table).18–30 The On-line Table summarizes the clinical and imaging data from our patients and from those in the literature.
The prognosis of patients with an AT/RT is poor, especially in patients younger than 3 years of age, with a survival time that averages 15 months in children and 38 months in adults.10,18,19,24
To our knowledge, there are only limited case reports describing the imaging features of this entity in adults.8,9,18,19,21–31 The goal of this study was to characterize the CT and MR imaging features of CNS AT/RT in 5 adults.
Materials and Methods
Patients
This study was approved by our institutional review board in accordance with standards of the National Institutes of Health. Five consecutive adult patients who received a diagnosis of AT/RT from January 2001 to October 2009 were included in the study. All patients had undergone surgical resection of their tumor and had received postoperative radiation therapy and chemotherapy. The resection specimens were collected and analyzed at 1 central pathology laboratory. Definitive diagnosis was based on histologic and immunohistochemical evaluation. The clinical and imaging characteristics of the 5 patients were analyzed, including MR images for all 5 patients and CT scans for 2 patients.
Imaging Protocol
All CT examinations were performed by using a 16-detector CT scanner (LightSpeed; GE Healthcare, Milwaukee, Wisconsin). Noncontrast axial images were obtained from the vertex to the skull base by using 2.5-mm-thick sections, a tube current of 250 mA, and a voltage of 125 kV.
All preoperative MR images were acquired by using 1 of two 1.5T MR imaging systems (Magnetom VP, Siemens, Erlangen, Germany; Gyroscan-Intera, Philips Healthcare, Best, the Netherlands). T1- and T2-weighted images and T1-weighted images with contrast administration (gadopentetate dimeglumine) were reviewed by the radiologists. For 2 patients, FLAIR images were available. A DWI sequence was performed in 1 patient.
Imaging Review
Two experienced radiologists retrospectively reviewed the CT and MR images by consensus for the location, size, presence of calcification, T1 and T2 signal-intensity characteristics, extent of vasogenic edema, and enhancement patterns.
Results
Clinical Data
The patients' clinical data (3 men and 2 women) are summarized in the On-line Table. The patients' ages ranged from 24 to 50 years (median age, 32 years). Three patients presented with a history of headache, 2 patients presented with nausea and vomiting, and 3 patients complained of blurred vision, epilepsy, and emotional disturbance, respectively. The course of the disease ranged from 1 month to 2 years.
Pathologic Findings
All specimens of AT/RT had histologic evidence of rhabdoid cells and were characterized by discrete cell borders and eccentric reniform nuclei, often with prominent nucleoli and eosinophilic cytoplasm. Necrosis was described in the reports of 4 lesions. The rhabdoid cells consistently displayed immunoreactivity for vimentin. Positive reactions of antibodies to epithelial membrane antigen, glial fibrillary acidic protein, smooth muscle antibody, and neurofilament protein were 80%, 80%, 60%, and 60%, respectively. The labeling index for Ki-67 was >40% in all 5 lesions. Additional cytogenetic, mRNA, or protein analyses were not performed.
Tumor Location and Size
All 5 AT/RTs were supratentorial (Figs 1⇓⇓–4). Two tumors were located in the right frontal lobe, and the remaining 3 tumors were located in the right temporal lobe, the left parieto-occipital lobe, and the right temporo-occipital lobe, respectively. The tumor within the right temporo-occipital lobe was associated with overlying calvarial destruction with extension into the galea.

CT and MR images of a 35-year-old woman with AT/RT of the right frontal lobe. A and B, Axial CT images show a lesion with intermediate attenuation and multiple calcifications and zones of low attenuation. C, Axial T1-weighted MR image shows a lesion with marked necrosis; the necrotic component is hypointense, and the solid component is isointense. D, Axial T2-weighted MR image reveals a hyperintense cystic component and an isointense solid component. E, Axial FLAIR image demonstrates iso- and hyperintense signal intensity with mild peritumoral edema. F−H, Axial, sagittal, and coronal MR images show an irregular thick-walled tumor with bandlike rim ring enhancement surrounding central necrosis.

MR images of a 25-year-old man with AT/RT of the left parieto-occipital lobe. A, Axial T1-weighted MR image shows a hypointense lesion. B and C, Axial and sagittal T2-weighted MR images show a hyperintense lesion with an isointense tumor nodule. D, Axial FLAIR image shows a hyperintense cystic component of the lesion with mild peritumoral edema. E and F, Axial DWI and ADC MR images show the solid component to be diffusion-restricted. G and H, Axial and sagittal MR images show nodular ring enhancement surrounding central necrosis.

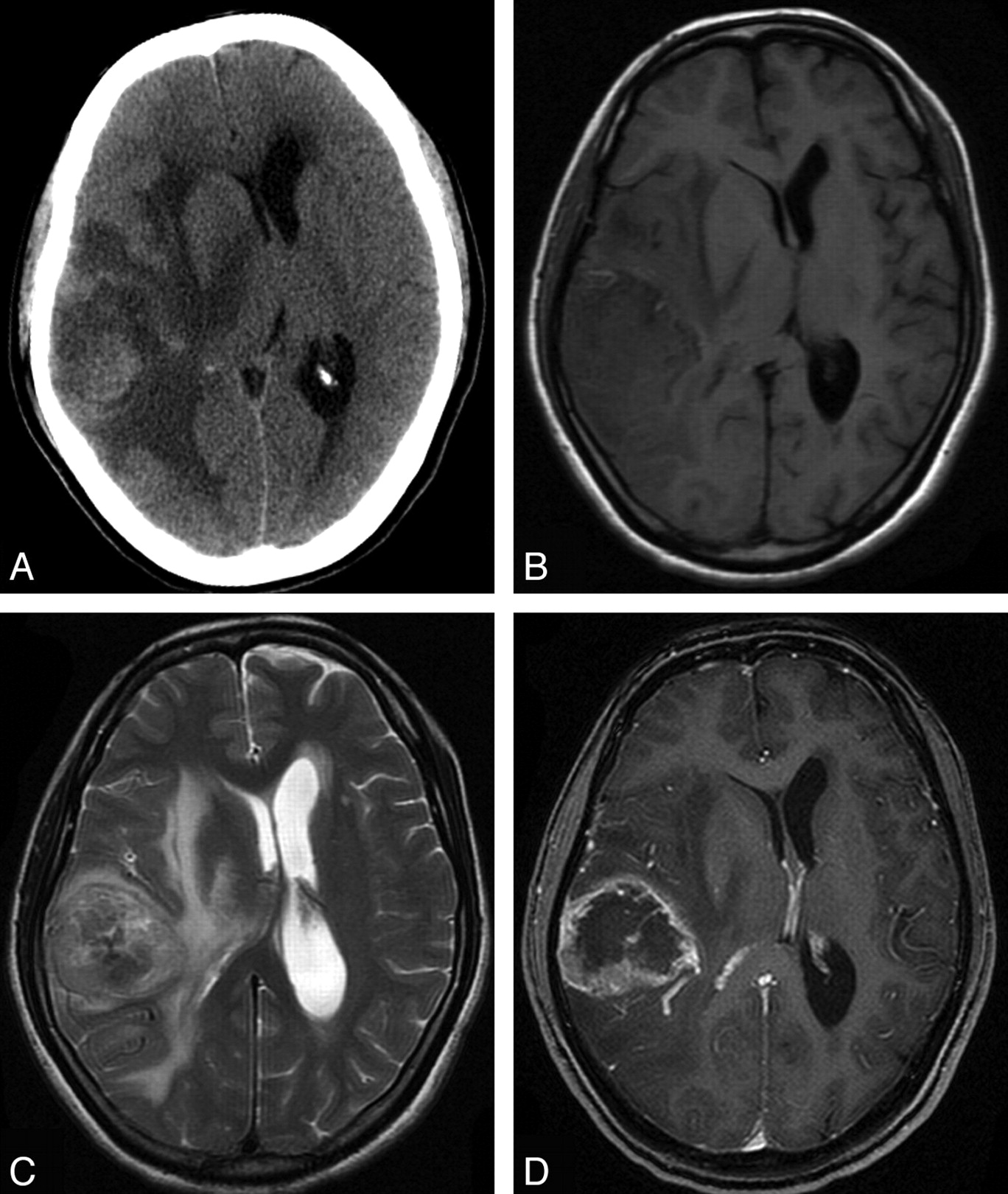
CT and MR images of a 50-year-old woman with AT/RT of the right temporal lobe. A, Axial CT image shows a lesion with intermediate attenuation and zones of low attenuation with marked peritumoral edema. B, Axial T1-weighted MR image shows a lesion with iso- to hypointense signal intensity with compression of the right lateral ventricle. C, Axial T2-weighted MR image shows a tumor with iso- to hyperintense signal intensity and with obvious edema. D, Axial MR image shows a tumor with an irregular thick wall, with ring and internal linear enhancement surrounding central necrosis.

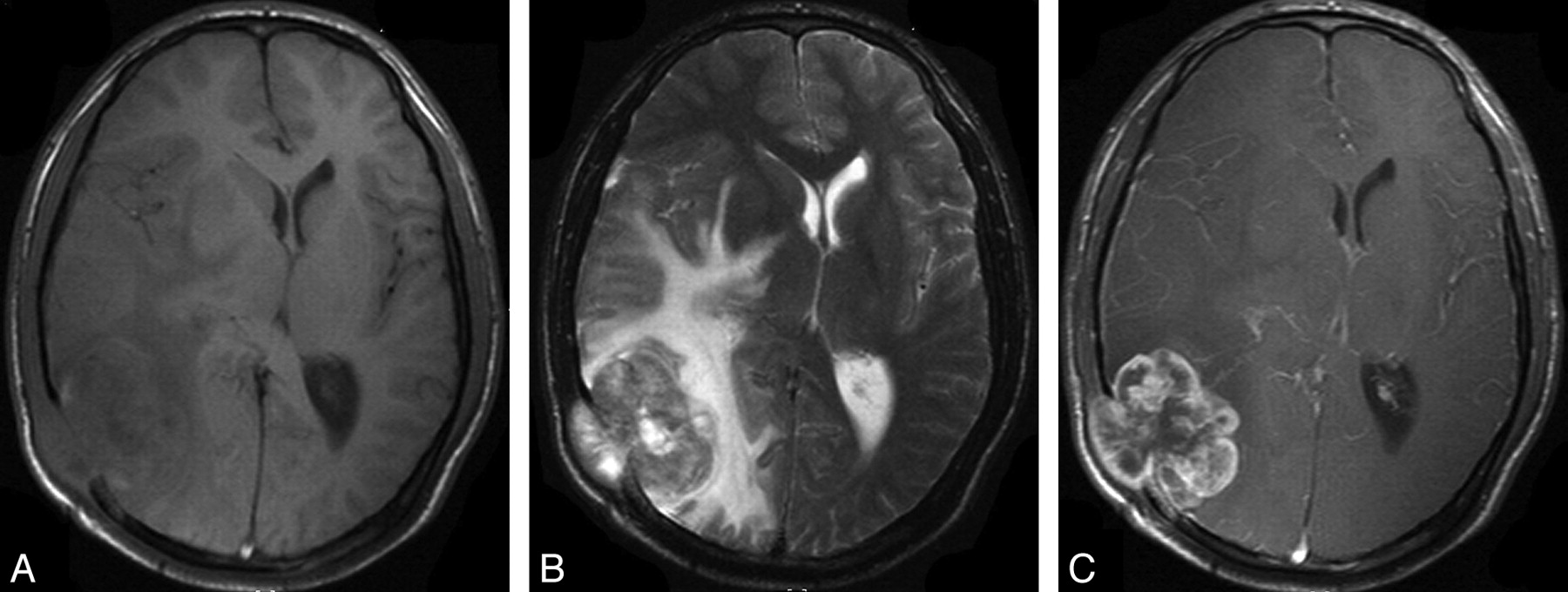
CT and MR images of a 24-year-old man with AT/RT of the right temporo-occipital lobe. A, Axial T1-weighted MR image shows a lesion with iso- to hypointense signal intensity. B, Axial T2-weighted MR image shows an iso- to hyperintense lesion with obvious peritumoral edema. C, MR image shows a tumor with irregular ring enhancement. The tumor has destroyed the overlying skull and extended into the galea.
At diagnosis, the tumors ranged from 4 to 10 cm in greatest diameter with a mean of 6.4 cm. Four tumors (80%) were >5 cm in at least 1 dimension. Only 1 tumor was <5 cm at initial presentation.
Preoperative CT and MR Imaging Characteristics
The patients' imaging findings are summarized in the On-line Table. On CT, the tumors appeared hyperattenuated compared with white matter, with a cystic/necrotic component (Figs 1A and 3A). One tumor showed lump and punctiform calcifications (Fig 1A).
Five patients had precontrast T1-weighted studies available for review. Three (60%) showed areas of both hypo- and isointensity, and 2 were hypointense. On the 5 T2-weighted studies performed, 4 (80%) showed areas of hyper- and isointensity and 1 (20%) had a mixed appearance with areas of hypo-, hyper-, and isointensity.
FLAIR images of 2 tumors before surgery were available for review. Solid portions of the tumor were iso- to slightly hyperintense (n = 2). Necrotic/cystic portions were iso- to slightly hyperintense (n = 1) (Fig 1E); the cystic portion of another tumor was hyperintense (Fig 2D).
One patient in this series had undergone preoperative DWI. The solid portion of this tumor was hyperintense on DWI relative to normal brain parenchyma, indicating restricted diffusion within this tumor. The cystic portion was hypointense on DWI and hyperintense on ADC imaging (Fig 2E, -F).
Of the 5 patients in our series, 4 (80%) had tumors that appeared relatively well-demarcated from the surrounding brain parenchyma. Contrast-enhanced T1-weighted images depicted the boundaries of the tumors most clearly. Three tumors had mild infiltration/peritumoral edema (Figs 1⇑–3). Two had extensive adjacent edema (Fig 4).
In all 5 cases, the MR images demonstrated both solid and cystic components within the tumors. Three had obvious cystic and/or necrotic areas. All 5 patients had contrast-enhanced T1-weighted MR imaging performed, and their tumors demonstrated strong heterogeneous enhancement. In all 5 patients, an enhancement pattern consisting of a mixed solid and bandlike rim of strong enhancement surrounding a cystic or necrotic area was seen (Figs 1⇑⇑–4). Two tumors demonstrated nodular enhancement in the tumor walls (Fig 2). One case demonstrated intratumoral linear enhancement (Fig 3). In 1 patient, the tumor showed lobulated enhancement with calvarial destruction (Fig 4).
Patient Outcomes
All patients underwent surgical resection with 4 total resections and 1 partial resection. Postoperative adjuvant treatment consisted of aggressive chemotherapy (n = 4) and radiation therapy (n = 5). Four patients (80%) died between 10 to 25 months (mean, 17 months) after surgery. One patient was alive at 32 months after surgery with normal neurologic examination findings and follow-up MR imaging that showed no signs of tumor recurrence.
Discussion
The initial description of a rhabdoid tumor localized to the CNS was given in 1985.32 Rorke et al,16 in 1995, first characterized this tumor as an “atypical teratoid/rhabdoid tumor,” based on the disparate combination of rhabdoid, primitive neuroepithelial, epithelial, and mesenchymal components. Although most occur in infants and young children, AT/RT is being recognized in adults with increasing frequency. AT/RT was first recognized as a malignant intracranial rhabdoid tumor in an adult patient in 1992 by Horn et al.30 From then on, approximately 30 cases of adult AT/RT have been reported.18–30 In contrast to the pediatric neoplasm, most adult CNS rhabdoid tumors are supratentorial, with only 3 tumors located in the cerebellum and 2 in the spinal cord. Most cases were diagnosed on the basis of characteristic histologic and immunohistochemical features.
Atypical teratoid/rhabdoid tumor is the only nervous system tumor for which a pathognomonic alteration of a tumor-suppressor gene has been identified. Molecular studies have revealed that AT/RTs show alteration of the INI1/hSNF5 gene on chromosome 22. This is a component of the SWItch/Sucrose Non-Fermentable chromatin remodeling complex and functions as a tumor suppressor by positively regulating transcription of a particular set of eukaryotic genes, possibly including the c-Myc target genes involved with differentiation and apoptosis.19,22,24 The loss of expression of INI1 is considered to be diagnostic for AT/RT.33 The diagnosis of AT/RT was not confirmed by cytogenetic or mRNA analysis, and this omission is a limitation of our retrospective review.
AT/RT is characterized by an aggressive clinical behavior in most children, who usually die within 7 months of initial diagnosis despite aggressive therapy.34,35 The behavior of the tumor in adults seems to differ somewhat in that survival time, based on current cases and literature review, averages 26 months (range, 1.5 months to 17 years). A recent report suggests that aggressive therapy, including surgery, radiation therapy, and multiagent chemotherapy designed for parameningeal rhabdomyosarcoma can significantly alter the course of the disease. More important, Zimmerman et al36 have reported on the first 2 survivors treated with this modified regimen, after relapse with multiagent intravenous and intrathecal chemotherapy.
Imaging findings in children are usually nonspecific at the time of diagnosis. CT usually shows an isoattenuated or slightly hyperattenuated mass in relation to the normal gray matter, with mild-to-marked surrounding edema.1 The CT findings in adults are similar to those in children.27,29,30 In the 2 patients in our series who underwent CT, the tumor appeared hyperattenuated, probably representing a high cellular attenuation; and the cystic/necrotic component was hypoattenuated compared with white matter. Meyers et al10 have reported that calcifications within AT/RT were seen in half of the children who underwent preoperative CT, and similar CT findings have been reported by other investigators.11,37 In our series, only 1 patient showed calcifications within the tumor.
According to the prior literature, MR imaging signal-intensity characteristics of the solid components of these tumors are similar to those of gray matter on T1- and T2-weighted images, and multiple necrotic or cystic foci are common.1,3,4,9–12,19,27 Our patients demonstrated similar imaging findings. In the 1 patient in our study who had preoperative DWI and ADC imaging, the solid portion of the tumor showed restricted diffusion.
In previous studies, AT/RT was shown to have mild-to-severe peritumoral edema. In our study, mild surrounding edema was noted in 3 patients, and 2 patients showed extensive adjacent edema.
AT/RT showed heterogeneous enhancement on our contrast-enhanced T1-weighted images. Some previous reports described AT/RT enhancement in children and adults as a bandlike wavy rim of strong and uniform enhancement completely or only partially surrounding a central cystic or necrotic area.4 Similar imaging findings were present in all our patients with central necrosis confirmed at the time of surgery, as well at pathology.
In children, leptomeningeal dissemination of tumor at diagnosis/initial staging has been previously reported in 21%–34% of patients with AT/RT by using myelography or enhanced MR imaging and CSF cytology.10 There was no dissemination of tumor in adult patients at the time of diagnosis in our series or in the prior literature, to our knowledge. In 1 of our patients, a right temporo-occipital tumor had destroyed the overlying calvaria extending into the galea, a feature also reported by Arslanoglu et al11 and Evans et al,37 which reflects the very aggressive nature of these tumors.
We considered PNET, glioblastoma, gliosarcoma, high-grade oligodendroglioma, meningioma, and metastatic disease in the differential diagnosis of our patients. Hemorrhage had been documented in many cases of PNET and in some previously reported cases of AT/RT in adult patients.19,27,29 Therefore, the presence of hemorrhage was not helpful in the differential diagnosis of these tumors. Some similarities in the imaging appearances of AT/RT and glioblastoma or gliosarcoma have been reported,38 because those kinds of tumors have a predilection for similar sites and modes of enhancement, with calcification and destruction of the skull as key distinguishing features. Calcification had been documented in high-grade oligodendroglioma and in some cases of AT/RT in adult patients, so the presence of calcification was not helpful in the differential diagnosis of these tumors. Enhanced T1-weighted images of most AT/RTs show heterogeneous enhancement, whereas most meningiomas often show homogeneous enhancement. The patient's age and the history of extracranial tumor can be useful in differentiating AT/RT from metastatic disease.
Conclusions
In summary, although extremely rare and usually fatal, primary AT/RT of the brain should be considered in the differential diagnosis of an aggressive intracerebral neoplasm in adults. AT/RT in an adult is often a supratentorial peripheral well-demarcated tumor with solid and cystic components and mild-to-moderate surrounding edema. In adult patients, AT/RT should be considered in the differential diagnosis of a tumor that is isointense on T1- and T2-weighted images, contains a bandlike rim of strong and uniform enhancement surrounding a central cystic area, contains calcifications on CT, and is associated with destruction of the skull. It is important to perform a total resection of such tumors followed by chemotherapy and radiation therapy to afford patients a better prognosis.
Acknowledgments
We thank J. Z. Chen for her technical assistance.
Footnotes
-
Drs Lu Jun Han and Ying Wei Qiu contributed equally to this work.
-
Indicates article with supplemental on-line table.
References
- Received April 12, 2010.
- Accepted after revision June 13, 2010.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}