
Abstract
BACKGROUND AND PURPOSE: Devices to close a femoral arteriotomy are frequently used after catheterization for interventional radiology and cardiac procedures to decrease the time to hemostasis and ambulation and, potentially, to decrease local complications. The Mynx vascular closure device uses a sealant designed to occlude the access tract, resulting in hemostasis.
MATERIALS AND METHODS: We retrospectively reviewed all cases in which the Mynx device was used and for which follow-up angiography was available. A total of 146 devices were deployed in 135 patients. A follow-up vascular study visualizing the femoral artery was performed in 26 patients (27 studies).
RESULTS: There were 5 (5/27, 18%) cases of intravascular Mynx sealant on follow-up vascular imaging. Three pseudoaneurysms (3/27, 11%) were identified.
CONCLUSIONS: In this small study, intravascular sealant and pseudoaneurysms were found frequently after femoral arterial closure with the Mynx vascular closure device.
Abbreviations
- MAUDE
- Manufacturer and User Facility Device Experience
- PAS
- periodic-acid-Schiff
Multiple devices have been designed to close the femoral artery after access for interventional radiology and cardiology procedures. These closure devices were developed with the intention of decreasing the risk of bleeding from the artery and reducing the time of patient immobilization after catheter removal. Such devices include StarClose (Abbott, Chicago, Illinois), Perclose (Abbott), Angio-Seal (St. Jude Medical, Minnetonka, Minnesota), and, most recently, the Mynx vascular closure device (AccessClosure, Mountain View, California).
At our institution, for typical diagnostic or interventional procedures, we most frequently used the StarClose closure device. This device, while generally effective for hemostasis, frequently results in significant pain at the time of deployment. In a smaller number of patients, upper leg pain lasting weeks or longer has been noted. Finally, 1 patient (of >500 in whom the StarClose device was deployed) developed symptomatic femoral stenosis, which required surgical repair. This experience led us to try the Mynx vascular closure device, which was reported to be safe and effective and to result in very little pain at the time of deployment.1
To our knowledge, angiographic or sonographic evaluation of the femoral artery following deployment of the Mynx closure device has not been reported. In this article, we describe the results of follow-up femoral arteriography in the subset of patients in whom the femoral artery was visualized after initial closure with the Mynx device.
Materials and Methods
All patients in whom the Mynx vascular closure device was used for femoral artery closure were identified by hospital billing records. All follow-up vascular studies in which the femoral artery could be visualized (conventional angiography, CT angiography, and sonography) were then identified. Each follow-up study was subsequently reviewed retrospectively by an experienced radiologist to determine whether any vascular abnormalities of the femoral artery system were present.
The Mynx vascular closure device was deployed in the standard fashion as directed by the device manufacturer. Initially, the device was used almost exclusively during observation by the Mynx representative and was subsequently used exclusively by operators certified in the use of the Mynx device. A proctor from the company was present for most cases, even after certification. In addition, a more senior company representative observed the deployment of the device for 2 days at our institution to ensure that the proctor had provided reliable instruction in the use of the device. Throughout, our technique was judged to be adequate and no technical concerns were raised by the company proctor present for most of the device placements. Furthermore, the supervisor expressed no concerns regarding the instruction in the use of the device provided by the proctor.
Results
Between August 25, 2009, and October 19, 2009, 146 Mynx closure devices were used in 135 patients after femoral artery puncture. In 27/146 (18.5%) of cases, a follow-up vascular study visualizing the femoral artery was available. These studies were performed at a median follow-up time of 6 days (mean, 8.4 days) after the initial Mynx closure device was used.
In our practice, patients commonly undergo an initial diagnostic procedure and then return in approximately 1 week for a therapeutic intervention. Thus, most follow-up imaging studies (24/27, 89%) were femoral arteriograms performed at the conclusion of the interventional procedure before placement of a second closure device approximately 1 week after the deployment of a first closure device for the initial diagnostic angiogram. Three patients were evaluated by sonography rather than by femoral arteriography. One sonography examination was ordered for a patient with persistent severe groin pain (1/27, 4%). In addition, after concern regarding the Mynx device surfaced, surveillance sonographic examinations were performed on the 2 patients who still remained in the hospital (2/27; 7%).
In 26/27 cases with follow-up imaging, the Mynx device was deployed using a 5F sheath; none of these patients were anticoagulated for the procedure. In 1 patient, the Mynx device was deployed by using a 6F sheath following an interventional procedure in which intraprocedural heparin was given.
There were 5 definite (5/27, 18%) instances of filling defects detected by follow-up angiography (4 cases) or sonography (1 case), most likely representing intravascular Mynx sealant (Fig 1). All were asymptomatic and would not have been identified if follow-up angiography for an unrelated indication had not been performed. One of the 5 patients went to surgery for removal of foreign body (Fig 1) because of near occlusion of the superficial femoral artery, and 4 patients were observed and have remained asymptomatic. Pathologic examination of the sample obtained in the patient who underwent surgery confirmed that the filling defect was indeed intravascular Mynx sealant (Fig 2).

Intravascular Mynx sealant on femoral arteriography and sonography. A−D, Femoral angiograms in 4 patients with intravascular filling defects performed at 15 days (A), 1 day (B), 6 days (C), and 14 days (D) after placement of the Mynx device. E, Femoral sonography at 3 days after deployment of the Mynx vascular closure device demonstrates a hyperechoic foreign body within the common femoral artery.

Surgical pathology demonstrating intravascular Mynx sealant. A−D, Light (A and B) and electron (C and D) microscopy confirm the presence of Mynx sealant in a foreign body removed surgically from a patient who had undergone closure with the Mynx device. A, PAS stain (original magnification ×200) of an intravascular foreign body. B, PAS stain (original magnification ×200) of Mynx sealant embedded in paraffin. C, Electron micrograph of Mynx sealant exposed to blood in vitro (original magnification × 14200). D, Electron micrograph of an intravascular foreign body (original magnification × 14200).
An additional 3 patients (3/27, 11%) had pseudoaneurysms (Fig 3), two requiring sonography-guided thrombin injection and 1 treated conservatively. Of the pseudoaneurysms, 1 was diagnosed due to persistent pain after closure and 2 were discovered incidentally on follow-up angiography.

Pseudoaneurysms demonstrated by femoral arteriography and sonography. A and B, Follow-up femoral angiograms at 1 day (A) and 7 days (B) after Mynx deployment demonstrate pseudoaneurysms (arrows) of the common femoral artery. C, Axial arterial sonography performed 2 days after Mynx use shows the true lumen (gray arrow) and pseudoaneurysm (white arrow) of the common femoral artery.
Discussion
In 27 follow-up imaging studies after Mynx deployment, major femoral artery complications (intravascular Mynx sealant or pseudoaneurysm) were found in 29%; without follow-up vascular studies, however, only 1 of these complications would have been recognized (due to the presence of severe access-site pain). However, because follow-up examinations were obtained in less than 20% of patients, it is impossible to determine with precision the true incidence of adverse events associated with the device.
The Mynx device is designed to achieve femoral artery hemostasis by deploying a water-soluble biodegradable sealant in the femoral sheath tract while an intravascular balloon is positioned adjacent to the arteriotomy site. The apposition of the balloon to the arteriotomy site provides temporary hemostasis and theoretically prevents sealant from entering the artery. In addition to mechanical protection from the balloon, in theory, the column strength of the sealant is lost with contact to blood, resulting in horizontal spread rather than vertical spread into the blood vessel. This combination of safeguards has been reported to make it “virtually impossible to push [the sealant] forward into the artery.”1
The main publication reporting the results of the use of the current-generation Mynx vascular closure device is a prospective nonrandomized trial based in Europe.1 In this study of 190 patients, rapid hemostasis was achieved (mean, 1.3 minutes) with a success rate of 93%. Symptomatic complications were rare. A single symptomatic pseudoaneurysm was discovered (1/190), and another patient developed bleeding at the access site significant enough to require transfusion (1/190). This study did not, however, include angiographic or sonography follow-up. Thus, the frequency of asymptomatic intravascular sealant or pseudoaneurysms could not be determined. By comparison, without follow-up vascular imaging, the rate of symptomatic complications in our institutional experience would have been 1/146 devices deployed.
Despite the theoretic barriers preventing the sealant from entering the artery, cases reported from several sources suggest that this complication does occur. A case of symptomatic embolization to the popliteal artery was recently published.2 In addition, the US Food and Drug Administration−sponsored data base designed to track possible complications from the use of medical devices (MAUDE) contains >10 additional cases of possible or probable intravascular embolization. The MAUDE data base also contains reports of several pseudonaneurysms in patients in whom the device was used for closure and a number of instances of balloon detachment.3
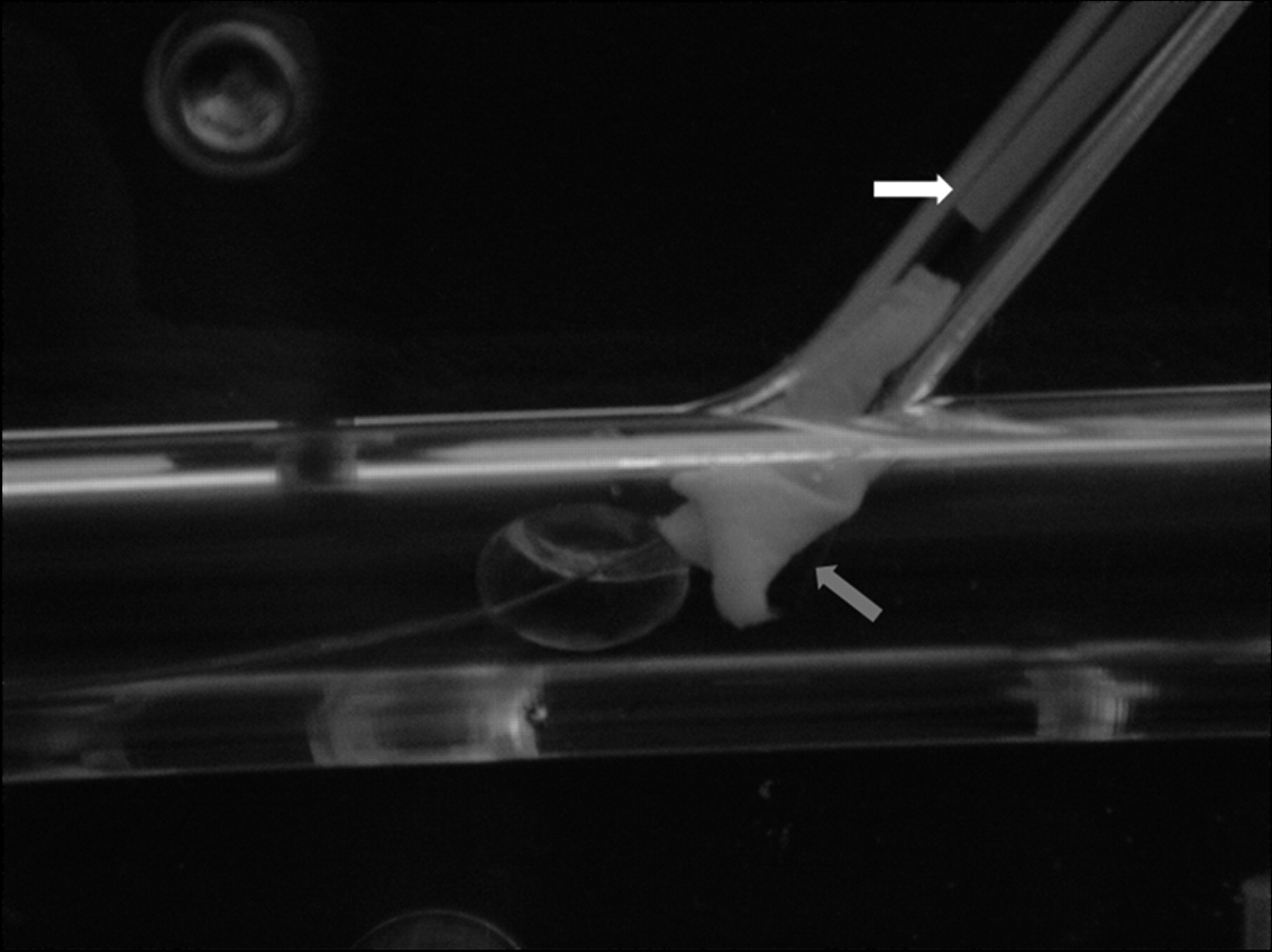
The means by which sealant may be introduced into the artery is well visualized with the plastic model developed to teach the use of the device (Fig 4). After the balloon is inflated and retracted against the arterial wall, the sealant is uncovered and released. Next, the white advancer tube is moved gently and rapidly 2 markers forward in the sheath tract. At this point, the polyethylene sealant may be advanced into the artery. Advancement of the white advancer tube could push sealant into the artery if insufficient hydration of the sealant occurs and the sealant maintains column strength. This may occur either if the balloon is not adjacent to the arteriotomy or by displacement of the balloon (if the balloon is not held firmly enough against the vessel wall). On the other hand, pulling too hard on the balloon may result in tenting of the artery and pseudoaneurysm formation; consequently, operators are instructed to limit the degree of traction. The end result is that the design does not allow one to be completely certain that the balloon is held firmly enough against the arterial wall to prevent intraluminal sealant deposition.

Plastic model demonstrating intra-arterial Mynx sealant. After the sealant is uncovered, it is advanced along the tract by the white advancer tube (white arrow). If the balloon is not pulled firmly against the arteriotomy site, an inadequate barrier results, and polyethylene sealant may be pushed into the intravascular space (gray arrow).
In our small study of patients who had follow-up examinations adequate to visualize the femoral artery following closure by using the Mynx device, we observed a high rate of intravascular Mynx sealant (5/27, 18%) and pseudoaneurysm (3/27, 11%). Because intravascular material can embolize distally and cause ischemia and because pseudoaneurysms may result in arterial rupture, we would discourage the use of this device until more data regarding its safety are available.
- Received January 4, 2010.
- Accepted after revision March 25, 2010.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Cerebral catheter angiography and its complications
- Safety and efficacy of percutaneous femoral artery access followed by Mynx closure in cerebral neurovascular procedures: a single center analysis
- Occurrence of angiographic femoral artery complications after vascular closure with Mynx and AngioSeal
- A prospective randomized single-blind trial of patient comfort following vessel closure: extravascular synthetic sealant closure provides less pain than a self-tightening suture vascular compression device